
 Download:
Download:




-
Achieving 95% human immunodeficiency virus (HIV) testing coverage represents the crucial first step in meeting the 95-95-95 targets for eliminating HIV transmission (1). HIV self-testing has emerged as a promising strategy to overcome testing barriers (2). In 2019, China introduced a self-administered rapid HIV urine antibody test that demonstrated high sensitivity (99.17%) and specificity (100.00%) under trial and laboratory conditions (3). However, its real-world diagnostic performance in clinical practice and self-administered scenarios requires further empirical validation, and preferences regarding HIV self-testing methods remain unexplored. This study evaluated the accuracy of the self-administered rapid HIV urine test compared to the blood rapid test in a real-world setting. Additionally, a discrete choice experiment (DCE) survey was conducted to identify key attributes and preferences for HIV self-testing (4). Our findings revealed that the urine rapid test exhibited lower accuracy than the blood rapid test, particularly when self-administered by participants. The results indicated preferences for HIV self-testing using finger prick samples, standard instruction text, and lower-cost options. These findings suggest that urine-based self-testing requires additional validation before integration into routine screening protocols, and future HIV self-testing development should prioritize user-friendliness to enhance testing accessibility.
This study was conducted in Guangzhou City, Guangdong Province, China, from July 2020 to February 2021. Men who have sex with men (MSM) participants were recruited through convenience sampling at a peer-friendly HIV test clinic (5). Each participant independently collected their urine sample, performed the urine rapid test, and interpreted the results. Subsequently, staff members conducted a second urine rapid test and interpretation using the same sample. Participants then underwent the standard blood rapid test, with positive results confirmed through western blot testing. For the DCE design (6), attributes and their corresponding levels are presented in
Supplementary Table S1 , with eight DCE choice sets detailed inSupplementary Table S2 . MSM testers who were permanent residents of Guangzhou and aged 18 years or older were invited to complete the DCE survey. The study was approved by the Ethics Committee of Sun Yat-sen University (Institutional Review Board number 054/19; February 28, 2019) and written informed consent was obtained from the participants.Differences in sensitivity and specificity among the three rapid tests (blood rapid test, staff-conducted urine rapid test, and participant-conducted urine rapid test) were evaluated using Cochran’s Q test. The Delong method was employed to assess differences in the area under the curve (AUC). For the DCE analysis, we utilized the conditional logit model, willingness to pay (WTP), and choice probability to identify participants’ preferences for HIV self-testing attributes and levels. Statistical significance was set at P<0.05. Multiple comparisons between the three rapid tests were adjusted using the Bonferroni method, with significance level α set at 0.017 (0.05/3). All analyses were performed using R software (version 4.0.2, R Core Team, Vienna, Austria).
Among the 1,094 participants who underwent rapid urine test accuracy assessment (Table 1), 46 (4.20%) were confirmed HIV-positive by western blot.
Types of HIV rapid self-tests Western blot result Total Sensitivity (%) (95% CI) Specificity (%) (95% CI) Positive Negative Blood rapid test Positive 46 2 48 100.00 (92.29, 100.00) 99.81 (99.31, 99.95) Negative 0 1,046 1,046 Total 46 1,048 1,094 Staff-conducted
urine rapid testPositive 41 1 42 89.13 (76.96, 95.27) 99.90 (99.46, 100.00) Negative 5 1,047 1,052 Total 46 1,048 1,094 Participant-conducted
urine rapid testPositive 38 3 41 82.61 (69.28, 90.91) 99.71 (99.16, 99.90) Negative 8 1,045 1,053 Total 46 1,048 1,094 Abbreviation: HIV=human immunodeficiency virus; CI=confidence interval. Table 1. The accuracy of the blood rapid test, staff-conducted urine rapid test, and participant-conducted urine rapid test (N=1,094).
The blood rapid test demonstrated optimal performance with 100.00% sensitivity [95% confidence interval (CI): 92.29, 100.00] and 99.81% specificity (95% CI: 99.31, 99.95). The staff-conducted urine rapid test showed 89.13% sensitivity (95% CI: 76.96, 95.27) and 99.90% specificity (95% CI: 99.46, 100.00), while the participant-conducted urine rapid test exhibited 82.61% sensitivity (95% CI: 69.28, 90.91) and 99.81% specificity (95% CI: 99.16, 99.90). Sensitivity differed significantly among the three rapid tests (P=0.002), whereas specificity did not (P=0.549). Multiple comparisons revealed significantly lower sensitivity in the participant-conducted urine rapid test compared to the blood rapid test (P=0.013). No significant differences were found between the staff-conducted urine rapid test and either the blood rapid test (P=0.074) or the participant-conducted urine rapid test (P=0.249). The AUC analysis showed significant differences (P=0.008) among the blood rapid test (0.9990) (Figure 1A), staff-conducted urine rapid test (0.9452), and participant-conducted urine rapid test (0.9116). Further pairwise comparisons revealed significantly lower AUC for the participant-conducted urine rapid test compared to the blood rapid test (P=0.002) (Figure 1B), marginally significant differences between the staff-conducted urine rapid test and blood rapid test (P=0.020) (Figure 1C), and no significant difference between staff-conducted and participant-conducted urine rapid tests (P=0.317) (Figure 1D).
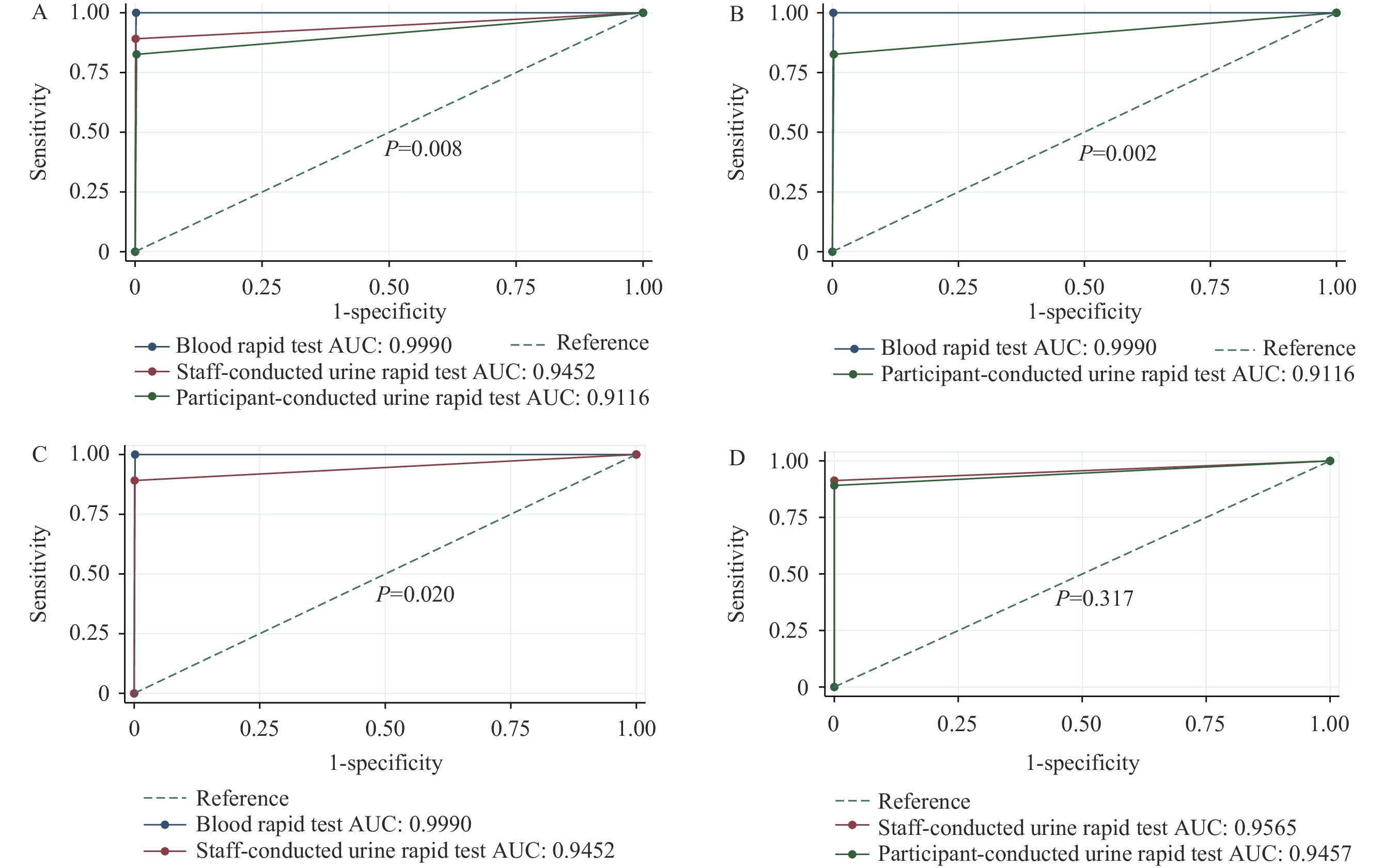 Figure 1.
Figure 1.Comparison of AUC among blood rapid test, staff-conducted urine rapid test, and participant-conducted urine rapid test. (A) Overall AUC comparison among the three test methods; (B) AUC comparison between blood rapid test and staff-conducted urine rapid test; (C) AUC comparison between blood rapid test and participant-conducted urine rapid test; (D) AUC comparison between staff-conducted and participant-conducted urine rapid tests.
Note: Panels B, C, and D represent post-hoc analyses following the overall comparison in panel A. Results were adjusted using the Bonferroni method (P<0.017 was considered statistically significant).
Abbreviation: AUC=area under the curve.
Of the 1,094 participants, 846 completed the DCE questionnaire. Compared to reference conditions (Table 2), participants showed significant preferences for finger prick sampling [odds ratio (OR)=1.470, 95% CI: 1.338, 1.616, P<0.001], regular instruction text (OR=1.169, 95% CI: 1.044, 1.308, P=0.007), and lower cost (OR=0.980, 95% CI: 0.977, 0.981, P<0.001). No significant preferences emerged regarding test result interpretation (OR=1.063, 95% CI: 0.928, 1.218, P=0.466). Willingness-to-pay analysis revealed participants would pay an additional $2.823 for finger prick sampling over urine sampling, and $1.141 more for regular instruction text compared to instructional video. Detailed hierarchical DCE analyses are presented in
Supplementary Tables S3–S4 , with choice probabilities for test type and instruction method shown for the total sample and subgroups inSupplementary Figure S1 .Attributes and levels OR 95% CI P WTP (USD)† Type of test Finger prick 1.470 (1.338, 1.616) <0.001* 2.823 Urine sample (reference) − − − − Instructions on how to conduct the test Regular instruction text 1.169 (1.044, 1.308) 0.007* 1.141 Instructional video (reference) − − − − The interpretation of test result By themselves 1.063 (0.928, 1.218) 0.381 0.446 By clinic staff (reference) − − − − Cost of the test§ 0.980 (0.977, 0.981) <0.001* − Note: “−” means this level is the reference level and there are no corresponding parameter values. This indicates the baseline category for comparison in the regression model.
Abbreviation: WTP=willingness to pay; OR=odds ratio; CI=confidence interval; USD=United States dollar; DCE=discrete choice experiment.
* P<0.05.
† $ {WTP}_{fingerprick} $=$ -{\beta }_{fingerprick}/{\beta }_{price} $.
§ The cost attribute was treated as a continuous variable in the DCE analysis to calculate willingness to pay, although it was constrained to four discrete values: 0 USD, 3 USD, 7.5 USD, and 12 USD.Table 2. Estimation of DCE in the total population (N=846).
-
Our study revealed that the urine rapid test demonstrated lower accuracy compared to the blood rapid test in real-world settings, particularly when self-administered by participants. The findings also indicated that participants expressed preferences for HIV self-testing using finger prick samples, conventional instruction text, and lower-cost options.
Previous evaluations of urine rapid tests have predominantly been conducted in controlled laboratory settings (7-8), with limited evidence of their diagnostic performance in real-world conditions. The underlying mechanism of urine rapid tests relies on detecting HIV antigens or nucleic acids through antibody-antigen binding or nucleic acid amplification. However, urine samples inherently contain lower concentrations of HIV antigens and nucleic acids compared to blood samples. Our study population likely included individuals in various stages of infection, including the incubation period with fluctuating viral loads, contrasting with laboratory studies that typically focus on confirmed positive cases. The reduced accuracy in real-world settings may be attributed to lower and more variable HIV antibody levels in non-blood samples, compounded by environmental variables absent in laboratory conditions. Furthermore, the visual interpretation of the urine rapid test strip bands presented additional challenges. Due to insufficient professional training and experience, coupled with the relatively weaker band intensity in some positive results, participants were more prone to misclassifying positive results as negative compared to trained staff. Staff surveys also revealed that positive results consistently showed weaker band intensity on urine rapid test strips compared to blood rapid test strips.
While extensive research exists on oral HIV self-testing (9), studies examining urine-based tests remain limited. Our DCE results demonstrated that high-risk populations in China preferred traditional blood-based testing methods with standard instruction text and affordable pricing. This aligns with previous research on oral tests, where participants similarly favored blood-based testing (1). These preferences may reflect limited awareness and uncertainty regarding novel testing methodologies. Nevertheless, some individuals preferred non-blood self-testing methods, citing advantages such as rapid results and painless administration (9). The preference for traditional instructional text over video formats may be attributed to its efficiency, accessibility, and independence from electronic devices. Future development efforts should prioritize creating user-friendly HIV test kits with clear instructions and streamlined procedures.
This study has several limitations. First, its geographical scope was restricted to a single city in Guangdong Province, China, potentially limiting the generalizability of our findings. Additionally, the DCE methodology did not include an opt-out option, consistent with similar DCE studies (10).
In conclusion, test accuracy is significantly influenced by detection methodology and test brand characteristics, highlighting the necessity for further validation of rapid urine testing. Furthermore, the development of user-friendly, cost-effective test kits with clear instructions is essential for enhancing HIV testing uptake among high-risk populations.
HTML
| Citation: |

|