
 Download:
Download:




-
In 2022, approximately 39 million people were living with human immunodeficiency virus (HIV) globally (1), with 29.8 million receiving antiretroviral therapy (ART) to suppress HIV-1 replication. While China’s National Free Antiretroviral Treatment Program (NFATP) was fully implemented in 2004, a significant increase in transmitted drug resistance has been observed. The prevalence of resistance to overall treatments, non-nucleoside reverse transcriptase inhibitors, efavirenz, and nevirapine rose from 2.6%, 1.8%, 1.6%, and 1.8%, respectively, during 2004–2007 to 7.8%, 6.7%, 6.3%, and 6.7% during 2020–2022 (2). Integrase strand transfer inhibitors (INSTIs) represent a new class of antiretroviral drugs with high genetic barriers to resistance. The World Health Organization now recommends dolutegravir (DTG) as a component of first-line ART and advocates for genotyping both reverse-transcriptase and integrase regions of HIV-1 (3). In China, INSTI-containing regimens were recommended as first-line treatment in 2018 (4), and DTG was incorporated into the NFATP for conditional use in 2023 (5). Regional surveys of pretreatment drug resistance (PDR) in various provincial-level administrative divisions (PLADs) have reported prevalence rates of 0.53% in Beijing (6), 1.7% in Jiangsu (7), and 0.71% in Chongqing (8). However, these studies were geographically limited with small sample sizes, and no large-scale national investigation of INSTI PDR has been conducted in China. To prevent drug resistance emergence a comprehensive understanding of INSTI PDR prevalence is crucial for developing second-line therapeutic strategies and maintaining vigilance against potential increases in resistance.
Molecular transmission network analysis enables the identification of active transmission clusters through genetic analysis. While HIV-1 pol gene sequences are commonly used for transmission network characterization, some researchers have successfully employed integrase (int) gene sequences (9). However, no large-scale national studies have utilized int sequences to investigate INSTI PDR in China.
This study aimed to conduct a comprehensive national survey to determine the prevalence of INSTI PDR and characterize viral mutations among newly diagnosed HIV individuals in China, while also examining transmission networks associated with INSTI drug resistance.
-
A cross-sectional study was conducted following the World Health Organization protocol for HIV pretreatment drug resistance surveillance across China’s regions. Based on HIV incidence, PLADs were stratified into high-, moderate-, and low-prevalence regions. Clinics were randomly selected within each study area, and patients were sequentially enrolled at these sites during the study period. Sample sizes for each PLAD are detailed in
Supplementary Table S1 . To assess the prevalence of PDR to INSTIs before their widespread implementation in China, we analyzed all available int sequences from 2018, 2022, and 2023. Inclusion criteria comprised: age ≥18 years; confirmed HIV-1 diagnosis in 2018, 2022, or 2023; int sequence length ≥500 bp (HXB2 positions 4230-5096); and provided informed consent. Exclusion criteria were age <18 years or prior ART exposure. This study received approval from the Ethics Committee of the National Centre for AIDS/STD Control and Prevention, China CDC (approval number X140617334).Viral RNA extraction was performed using the QIAsymphony platform, followed by integrase fragment amplification and sequencing using an in-house PCR protocol. Sequences were aligned and filtered using BioEdit, excluding those shorter than 500 nucleotides. HIV-1 subtypes were determined through phylogenetic analysis using IQ-Tree. Drug susceptibility predictions for five INSTIs [first-generation: raltegravir (RAL), elvitegravir (EVG); second-generation: dolutegravir (DTG), bictegravir (BIC), and cabotegravir (CAB)] were generated using the Stanford HIV Database genotypic resistance interpretation system.
Molecular transmission networks were constructed using the Tamura-Nei 93 model in HIV-TRACE. Each node in the network represented an HIV-infected individual with corresponding epidemiological data. Given the slower evolutionary rate of the int gene compared to the pol gene, nodes were connected using a genetic distance threshold of 0.5% substitutions per site. Network visualization was performed using web-based tools (https://veg.github.io/hivtrace-viz/) following established technical guidelines for HIV transmission network monitoring and intervention.
Statistical analyses were conducted using SAS (version 9.4, SAS Institute Inc, Cary, NC, USA). Factors associated with drug resistance were analyzed using logistic regression, with statistical significance set at P<0.05.
-
Among the 10,654 HIV-1-infected individuals recruited over the three-year study period, 41.9% were aged ≥50 years. The study population was predominantly comprised of men (79.0%) and individuals of Han ethnicity (83.3%). Most participants (60.1%) had educational attainment at or below junior high school level, and 35.2% were single. Heterosexual transmission was the primary route of infection (61.8%). The vast majority (98.3%) had no prior antiretroviral exposure, and 68.9% presented with CD4 cell counts between 200–499 cells/mm3 before initiating treatment. The HIV-1 subtype distribution showed CRF07_BC (45.4%), CRF01_AE (27.6%), CRF08_BC (8.9%), CRF55_01B (1.1%), and subtype B (3.0%) as the predominant strains (Table 1).
Variable 2018 2022 2023 Total N Prevalence (%) N Prevalence (%) N Prevalence (%) N Prevalence (%) Total 905 100.0 2,757 100.0 6,992 100.0 10,654 100.0 Age (years) 18−29 231 25.5 629 22.8 1,630 23.3 2,490 23.4 30−49 459 50.7 1,012 36.7 2,175 31.1 3,646 34.2 ≥50 215 23.8 1,116 40.5 3,138 44.9 4,469 41.9 Unknown 0 − 0 − 49 0.7 49 0.5 Sex Male 743 82.1 2,212 80.2 5,458 78.1 8,413 79.0 Female 162 17.9 545 19.8 1,470 21.0 2,177 20.4 Unknown 0 − 0 − 64 0.9 64 0.6 Ethnicity Han 744 82.2 2,252 81.7 5,876 84.0 8,872 83.3 Others 161 17.8 502 18.2 1,063 15.2 1,726 16.2 Unknown 0 − 3 0.1 53 0.8 56 0.5 Education Junior high school or blew 386 42.7 1,679 60.9 4,334 62.0 6,399 60.1 Senior high school 249 27.5 405 14.7 972 13.9 1,626 15.3 College and above 174 19.2 653 23.7 1,612 23.1 2,439 22.9 Unknown 96 10.6 20 0.7 74 1.1 190 1.8 Marital status Single 369 40.8 987 35.8 2,389 34.2 3,745 35.2 Married or cohabiting 410 45.3 1,227 44.5 2,975 42.5 4,612 43.3 Divorced or widowed 112 12.4 520 18.9 1,554 22.2 2,186 20.5 Unknown 14 1.5 23 0.8 74 1.1 111 1.0 Risk Heterosexual 460 50.8 1,699 61.6 4,424 63.3 6,583 61.8 Homosexual 402 44.4 925 33.6% 2,327 33.3 3,654 34.3 Intravenous drug use 21 2.3 28 1.0 32 0.5 81 0.8 Others 2 0.2 4 0.1 1 0.0 7 0.1 Unknown 20 2.2 101 3.7 208 3.0 329 3.1 Prior ARV exposure No 905 100.0 2,616 94.9 6,947 99.4 10,468 98.3 Yes 0 − 76 2.8 38 0.5 72 0.7 Unknown 0 − 65 2.4 7 0.1 114 1.1 CD4 cell count before ART (cell/mm3) <200 292 32.3 1,010 36.6 206 2.9 1,508 14.2 200–499 433 47.8 1,404 50.9 5,504 78.7 7,341 68.9 ≥500 148 16.4 302 11.0 1,282 18.3 1,732 16.3 Unknown 32 3.5 41 1.5 0 − 73 0.7 Subtype CRF07_BC 319 35.2 1,305 47.3 3,208 45.9 4,832 45.4 CRF01_AE 290 32.0 712 25.8 1,940 27.7 2,942 27.6 CRF08_BC 135 14.9 245 8.9 566 8.1 946 8.9 CRF55_01B 8 0.9 49 1.8 65 0.9 122 1.1 B 34 3.8 70 2.5 217 3.1 321 3.0 URFs 38 4.2 161 5.8 395 5.6 594 5.6 Others 81 9.0 215 7.8 601 8.6 897 8.4 Abbreviation: ART=antiretroviral therapy; ARV=antiretroviral drugs; HIV=human immunodeficiency virus; CRF=circulating recombinant form; URFs=unique recombinant forms. Table 1. Demographic and clinical characteristics of newly diagnosed HIV individuals in China.
Among the 10,654 HIV-1 individuals in our study, the overall prevalence of PDR to INSTIs was 0.95% (n=101). The PDR of RAL, EVG, DTG, BIC, and CAB were 0.91% (n=97) for RAL, 0.87% (n=93) for EVG, 0.21% (n=22) for DTG, 0.15% (n=16) for BIC, and 0.34% (n=37) for CAB. We identified nine major and six accessory INSTI-related drug resistance mutations (DRM). The E138K/A mutation, conferring low-level resistance to RAL and EVG, was the most frequent major mutation (n=19). Eight cases harbored the R263K mutation, which causes low-level resistance to RAL and intermediate-level resistance to EVG, DTG, BIC, and CAB. The combination of S147G and Q148K mutations resulted in high-level resistance to RAL, EVG, and CAB. The G163R/K accessory mutation, detected in 29 cases, conferred low-level resistance to RAL and EVG (Table 2).
Antiretroviral drug Prevalence, N % (95% CI) HIV drug resistance mutations and combination of mutations, n (%) INSTIs 101 0.95 (0.76, 1.11) Major mutations Raltegravir 97 0.91 (0.73, 1.09) E138K/A : 19 Elvitegravir 93 0.87 (0.69, 1.05) E138K+L74I : 1 Dolutegravir 22 0.21 (0.12, 0.29) E138K+E92Q+R263K : 1 Bictegravir 16 0.15 (0.08, 0.22) R263K : 8 Cabotegravir 37 0.34 (0.24, 0.46) R263K+A128T :1 Y143S/C/H : 8 T66A/I : 4 T66I+E157Q : 1 N155S/T : 3 N155H+Q95K+E157Q : 1 Q146P/R/L : 3 Q146R+S153A : 1 Q148R : 2 Q148K+S147G : 1 S147G : 1 G140R : 1 Accessory mutations G163R /K: 29 G163R+E157Q : 3 S230R : 6 S230R+S153F : 1 H51Y : 4 V151A : 2 S153F : 2 E157Q+T97A : 1 Abbreviation: HIV=human immunodeficiency virus; CI=confidence interval. Table 2. Prevalence and patterns of HIV integrase strand transfer inhibitor resistance mutations among newly diagnosed individuals in China.
Multivariate analysis revealed that individuals with HIV-1 subtype B had significantly higher odds of drug resistance compared to those with CRF07_BC [adjusted odds ratio (aOR)=3.87, 95% confidence interval (CI): 1.97, 7.58]. Additionally, individuals aged ≥50 years showed increased odds of drug resistance compared to those aged 18–29 years (aOR=1.87, 95% CI: 1.03, 3.42) (Table 3).
Variable N PDR, n (%) OR (95% CI) P aOR (95% CI) P Total 10,654 101 (0.95) Age (years) 18–29 2,490 14 (0.56) 1.00 30–49 3,646 37 (1.01) 1.81 (0.98, 3.36) 0.059 1.80 (0.97, 3.35) 0.062 ≥50 4,469 49 (1.10) 1.96 (1.08, 3.56) 0.027 1.87 (1.03, 3.42) 0.041 Unknown 49 1 (2.04) 3.69 (0.48, 28.59) 0.211 3.71 (0.45, 29.08) 0.212 Sex Male 8,413 79 (0.94) 1.00 Female 2,177 22 (1.01) 1.08 (0.67, 1.73) 0.760 Unknown 64 0 (0.00) − − Ethnicity Han 8,872 85 (0.96) 1.00 Others 1,726 13 (0.75) 0.79 (0.44, 1.41) 0.417 Unknown 56 3 (5.36) 5.85 (1.79, 19.09) 0.003 Education Junior high school or blew 6,399 64 (1.00) 1.00 Senior high school 1,626 17 (1.05) 1.05 (0.61, 1.79) 0.870 College 2,439 18 (0.74) 0.74 (0.44, 1.24) 0.253 Unknown 190 2 (1.05) 1.05 (0.26, 4.33) 0.943 Marital status Single 3,745 34 (0.91) 1.00 Married or cohabiting 4,612 50 (1.08) 1.20 (0.77, 1.85) 0.422 Divorced or widowed 2,186 15 (0.69) 0.75 (0.41, 1.39) 0.364 Unknown 111 2 (1.80) 2.00 (0.48, 8.44) 0.344 Risk Heterosexual 6,583 64 (0.97) 1.00 Homosexual 3,654 32 (0.88) 0.90 (0.59, 1.38) 0.628 IDU 81 0 (0.00) − − Others 7 0 (0.00) − − Unknown 329 5 (1.52) 1.57 (0.63, 3.93) 0.334 Prior ARV exposure No 10,468 101 (0.96) 1.00 Yes 72 0 (0.00) − − Unknown 114 0 (0.00) − − CD4 cell count before ART (cell/mm3) <200 1,508 12 (0.80) 1.00 200–499 7,341 73 (0.99) 1.25 (0.68, 2.31) 0.472 ≥500 1,732 15 (0.87) 1.09 (0.51, 2.33) 0.826 Unknown 73 1 (1.37) 1.73 (0.22, 13.50) 0.600 HIV subtype CRF07_BC 4,832 44 (0.91) 1.00 CRF01_AE 2,942 22 (0.75) 0.82 (0.49, 1.37) 0.449 0.84 (0.50, 1.41) 0.510 CRF08_BC 946 10 (1.06) 1.16 (0.58, 2.32) 0.669 1.10 (0.55, 2.20) 0.799 CRF55_01B 122 0 (0.00) − − − − B 321 11 (3.43) 3.86 (1.98, 7.55) <0.001 3.87 (1.97, 7.58) <0.001 URF 594 7 (1.18) 1.30 (0.58, 2.89) 0.524 1.33 (0.60, 2.98) 0.481 Others 897 7 (0.78) 0.86 (0.38, 1.91) 0.703 0.87 (0.39, 1.93) 0.723 Diagnosed year 2018 905 7 (0.77) 1.00 2022 2,757 26 (0.94) 1.22 (0.53, 2.82) 0.640 2023 6,992 68 (0.97) 1.26 (0.58, 2.75) 0.562 Note: P values <0.05 were considered statistically significant.
“−” means not available.
Abbreviation: ART=antiretroviral therapy; ARV=antiretroviral drugs; IDU=intravenous drug use; CRF=circulating recombinant form; URFs=unique recombinant forms; HIV=human immunodeficiency virus; CI=confidence interval; aOR=adjusted odds ratio.
* P values were calculated using Pearson’s Chi-squared test.Table 3. Risk factors associated with integrase strand transfer inhibitor resistance among newly diagnosed HIV individuals in China.
Molecular transmission network analysis, using a genetic distance threshold of 0.5% substitutions per site, identified 1,257 (26.0%) CRF07_BC sequences forming 432 clusters (size range 2–217) among 4,832 analyzed sequences. Within these clusters, 11 drug-resistant sequences were distributed across 8 clusters, harboring mutations including E138K, Y143H, E157Q, G163R/K/S, and R263K. Notably, Cluster 1 contained two nodes sharing E157Q and G163R mutations, while Cluster 2 comprised three individuals with G163R (Figure 1A). Analysis of 2,942 CRF01_AE sequences revealed 811 (27.6%) sequences forming 335 clusters (size range 2–15), with two drug-resistant strains carrying E138K/A mutations distributed across two clusters (Figure 1B).
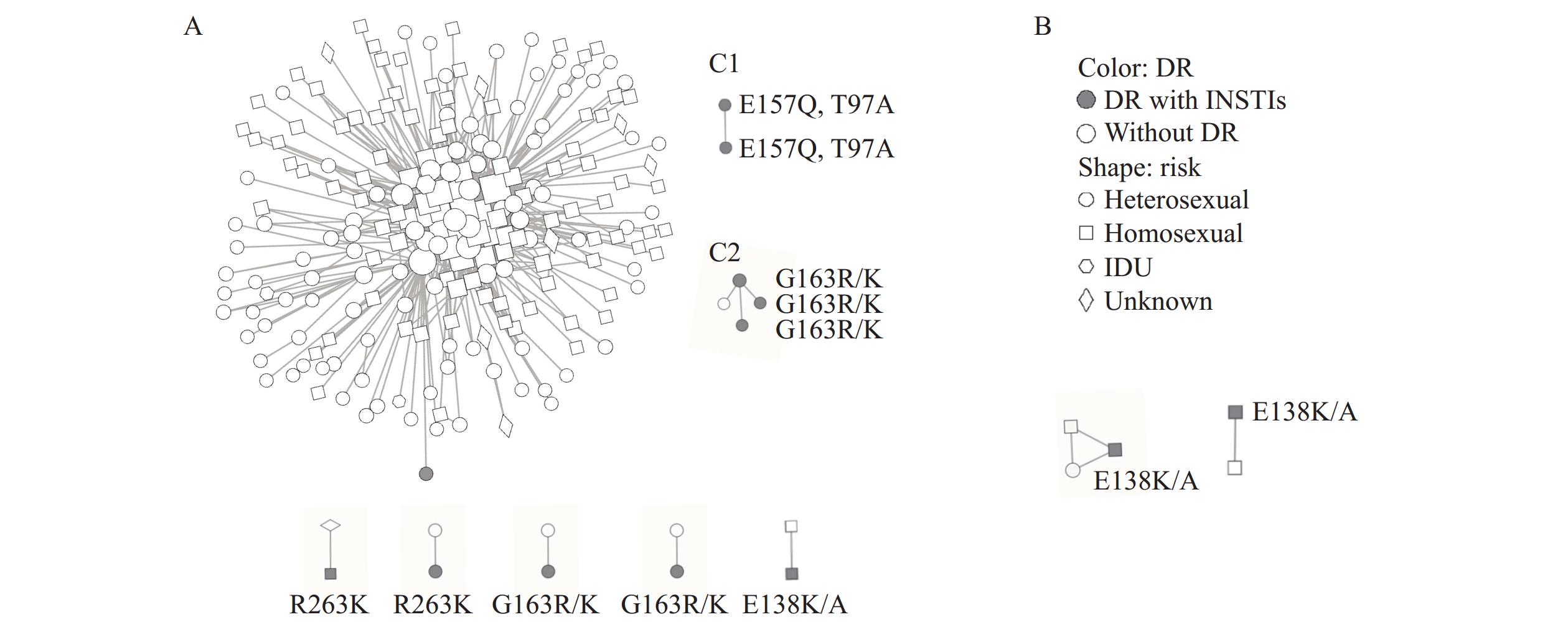 Figure 1.
Figure 1.Molecular transmission clusters containing pretreatment drug resistance to INSTIs. (A) Resistance mutations identified in HIV-1 subtype CRF07_BC; (B) Resistance mutations identified in HIV-1 subtype CRF01_AE.
-
In China, the PDR to INSTIs was 0.95%, which aligns with previous reports (10). This prevalence is marginally higher than surveys from six Chinese PLADs (0.80%) (11), Beijing (0.53%) (6), and Chongqing (0.71%) (8), yet slightly lower than reports from Jiangsu (1.7%) (7), Shenzhen (1.77%) (12), and Taiwan (2.6%) (13). The observed rates are notably lower than those reported in European and American regions, including Italy (1.5%) (14), Mediterranean Europe (2.33%) (15), Spain (2.5%) (16), and Chile (8.0%) (17). The higher PDR prevalence in Western countries likely reflects their earlier and more extensive INSTI implementation, exemplified by Chile, where approximately 60% of HIV patients receive INSTI-based therapy (17). According to WHO’s qualitative classification, China’s PDR prevalence of INSTIs remains at a low level.
The predominant DRM sites identified were E138, R263, Y143, T66, N155, G140, Q146, S147, and Q148. E138K/A emerged as the most frequent mutation, representing a non-polymorphic alteration that typically confers high-level resistance to RAL and EVG while inducing intermediate-level resistance to DTG. We also identified eight cases harboring the R263K mutation, a non-polymorphic variant selected in vitro by EVG, DTG, BIC, and CAB, which reduces susceptibility to all INSTIs (18). The prevalence of E138 and R263 as the two primary major mutations corresponds with findings from Italian studies (14). Among accessory DRMs, we detected G163, S230, H51, S153, E157, and T97. The G163R/K mutation, a non-polymorphic variant primarily selected by RAL, contributes to low-level resistance against first-generation INSTIs. This G163 mutation has also been frequently documented in other regions, including Italy, Ghana, and Chile (14–19). Continued surveillance and monitoring remain crucial for tracking the dissemination of resistant strains.
Multivariable analysis revealed that patients with subtype B had 3.87 times greater odds of PDR compared to those with subtype CRF07_BC, consistent with previous findings in China (14). This association likely stems from the initial deployment of INSTIs in Europe and the United States, where subtype B predominates. Additionally, individuals aged ≥50 years demonstrated 1.87 times greater odds of PDR compared to those aged 18–29 years. Research has indicated that older populations play a significant role in drug resistance transmission (21).
Our construction of subtype-specific molecular transmission networks using int sequences of CRF07_BC and CRF01_AE revealed notable patterns. Within the CRF07_BC network, we identified two resistance strains in Cluster 1 and three in Cluster 2. Both nodes in Cluster 1 exhibited E157Q and G163R mutations, while all three nodes in Cluster 2 displayed G163R mutations. The presence of identical DRMs within single molecular clusters suggests strong transmission relationships among these HIV-positive individuals, though additional epidemiological investigations are necessary to confirm direct transmission links.
This study has several limitations. First, incomplete information from drug-resistant individuals may have affected the analytical accuracy. Second, the use of Sanger sequencing limited detection to drug-resistant variants present at frequencies above 20%. Additionally, the slower evolutionary rate of the HIV int gene compared to the pol gene necessitates further methodological evaluation for molecular transmission network construction using integrase sequences.
In conclusion, the prevalence of PDR to INSTIs in China remains low. While INSTIs represent a relatively new and effective class of antiretroviral drugs, patients harboring resistant strains will maintain these mutations indefinitely and potentially transmit them to others, thereby compromising therapeutic efficacy. Given the increasingly widespread use of INSTIs, continuous surveillance of these individuals is essential to provide optimal preventive interventions and therapeutic strategies. Furthermore, achieving the global objective of eliminating AIDS as a public health threat by 2030 requires coordinated national and provincial efforts in regular PDR surveillance.
-
The staff members at the provincial Centers for Disease Control and Prevention for their contributions to data collection and laboratory testing.
HTML
| Citation: |

|