

 Download:
Download:




-
Influenza vaccination represents a cornerstone of public health interventions for controlling this highly transmissible disease. However, in countries like China, where vaccination remains voluntary and lacks public funding, achieving adequate vaccination coverage presents significant challenges (1–2). The “volunteer” strategy, which depends on individuals’ self-funded participation, has consistently resulted in suboptimal coverage rates and elevated outbreak risks. This situation necessitates innovative approaches to enhance vaccination compliance. The “adherence” strategy, designed to encourage previously vaccinated individuals to maintain their vaccination status through consistent advocacy, healthcare provider interventions, and financial incentives, offers a more pragmatic alternative to mandatory vaccination policies.
While existing vaccination strategies and their corresponding models have proven effective in cost-effectiveness analyses (CEAs), they often fail to capture the complex interplay between individual behaviors, social dynamics, and economic factors (1–3). Traditional Markov models, though effective for disease progression simulation, cannot adequately represent individual-level dynamics and social interactions that significantly influence vaccination decisions. Similarly, compartmental models, such as the SEIR model, while valuable for understanding disease transmission dynamics, tend to oversimplify population heterogeneity and the nuanced aspects of vaccination behavior (4–6).
To address these methodological limitations, we propose an innovative hybrid modeling approach that integrates continuous-time agent-based models (ABMs) with Markov models. The continuous-time ABM component enables detailed simulation of disease transmission and individual interactions within populations, providing granular insights into the temporal evolution of vaccination compliance strategies (5). By combining this with a Markov model that captures the stochastic nature of vaccination decisions across multiple cycles, we can comprehensively analyze the long-term cost-effectiveness of different vaccination strategies. Our hybrid model provides a sophisticated framework for evaluating sustained vaccination compliance strategies, offering more precise and nuanced assessments of the benefits and costs associated with various vaccination approaches.
In summary, this study presents a sophisticated analytical tool that leverages the complementary strengths of continuous-time ABMs and Markov models to conduct comprehensive, long-term CEA of vaccination compliance strategies. This hybrid model demonstrates significant potential for informing evidence-based public health policy and practice.
-
We propose a novel hybrid modeling framework that integrates a continuous-time agent-based susceptible-exposed-infected-hospitalized-removed/recovered (SEIHR) model with a Markov model for the cost-effectiveness analysis of influenza vaccination compliance strategies (4-5). Schematic representations of the agent-based SEIHR and hybrid models are provided in Figures 1A and 1B, with a comprehensive description included in the Methods section of the
Supplementary Material . Figure 1.
Figure 1.Framework of the SEIHR model and the proposed hybrid model for influenza vaccination compliance strategy analysis. (A) SEIHR model. (B) The proposed hybrid model.
Note: SEIHR model with compartments or states: susceptible (S), exposed (E), infectious (I), hospitalized (H), and removed/recovered (R). For every cycle, the individual vaccination uptake is modeled through a Markov model, contingent upon infection status and prior vaccination history, followed by an ABM simulation to depict influenza spread dynamics. This iterative process repeats for each cycle.
Abbreviation: SEIHR=susceptible-exposed-infected-hospitalized-removed/recovered; ABM=agent-based model.
The SEIHR model, adapted from traditional compartmental models, simulates influenza transmission within a randomly mixed population by incorporating individual-level interactions and disease dynamics. This model has been transformed into an agent-based format, with its deterministic nature validated against stochastic ABMs through previous studies (5–6).
Our proposed hybrid model iteratively transitions between the ABM simulation of one cycle and a Markov model-based vaccination process for the subsequent cycle, continuing this sequence for a predefined number of cycles to evaluate long-term vaccination compliance strategies.
We conducted simulations to demonstrate the application of our hybrid model in long-term CEA of influenza vaccination compliance strategies. Table 1 presents the parameter configurations used in the simulation. The baseline population was stratified according to age group proportions (≤18, 20–64, and ≥65 years old) derived from the China Statistical Yearbook 2023, with the national gross domestic product (GDP) per capita set at 85,698 Chinese Yuan (CNY) (7). The population size N was established at 1,000,000. Daily utility values for each state were derived from QALYs in the literature divided by 365 (8–9). Daily costs for infected (I) and hospitalized (H) states were derived by dividing the total outpatient and inpatient costs from the literature by their respective average duration of care (3,10). For the middle age group (20–64 years), the daily hospitalization cost incorporated lost labor productivity based on GDP per capita divided by 365. Vaccine cost was fixed at 67.1 CNY per dose (1). Each cycle represented one year (365 days), with a 5% discount rate applied to both costs and utilities (QALYs) over 5 cycles (5 years) (11).
Parameters Age groups References Age group 1
(≤19)Age group 2
(20–64)Age group 3
(≥65)Baseline proportion 0.2137 0.6375 0.1488 (7) Baseline vaccination coverage, c 0.251 0.067 0.267 (12) Previous vaccination multiplier for coverage, mcv 1.5 1.5 1.5 − Previous infection multiplier for coverage, mci NI: 0.8
I: 1
IH: 2NI: 0.8
I: 1
IH: 2NI: 0.8
I: 1
IH: 2− Discount rate 0.05 0.05 0.05 (11) Rate from S to E, β 0.225 0.107 0.088 (3) Rate from E to I, λ 0.5 0.5 0.5 (3) Rate from I to H, α 0.0141 0.0193 0.0421 (13) Rate from H to R, μ 0.0847 0.0847 0.0847 (2) Rate from I to R, γ 0.1613 0.1613 0.1613 (2) Vaccination multiplier for the rate from S to E, mβv 0.36 0.41 0.42 (14–15) Vaccination multiplier for the rate from I to H, mαv 0.47 0.68 0.68 (3) Cost per day (CNY) I : 157
H: 833I: 157
H: 1068I: 157
H: 833(7,10) QALY S: 0.8434
E: 0.8434
I : 0.6216
H: 0.6132
R: 0.8434S: 0.8434
E: 0.8434
I : 0.5939
H: 0.4913
R: 0.8434S: 0.8071
E: 0.8071
I : 0.5733
H: 0.4128
R: 0.8071(8–9) Vaccination cost per dose (CNY) 67.1 67.1 67.1 (1) Attack rate 0.01 0.01 0.01 − Note: S, E, I, H, and R represent the states of the SEIHR model. For the previous infection multiplier for coverage, NI, I, and IH represent no infection, infection without hospitalization, and infection with hospitalization, respectively. A dash (“-”) indicates that the values are self-determined in the absence of relevant references.
Abbreviation: CNY=Chinese Yuan; SEIHR=susceptible-exposed-infected-hospitalized-removed/recovered; QALY=quality-adjusted life year.Table 1. Overview of vaccination compliance strategies and their parameters.
Two distinct vaccination compliance strategies were evaluated. The “volunteer” strategy served as a baseline approach, where each agent’s vaccination probability per cycle was calculated by multiplying the age group-specific baseline coverage (c) by previous infection multiplier (mci) and vaccination multiplier (mcv) when applicable (i.e., cmcimcv for previously vaccinated individuals, and cmci for those not previously vaccinated) (12–15). The “adherence” strategy differed fundamentally by implementing scheduled follow-up vaccinations in subsequent cycles for individuals who received vaccination within a particular cycle. Given the stochastic nature of the ABM, we performed 1,000 simulation replicates and conducted probabilistic sensitivity analysis (PSA) to evaluate the economic outcomes of these strategies. The analysis included the incremental cost-effectiveness ratio (ICER), cost-effectiveness plane (CEP), cost-effectiveness acceptability curves (CEACs), cost-effectiveness acceptability frontier (CEAF), and expected value of perfect information (EVPI). The PSA incorporated random variable probability distributions for attack rate, baseline vaccination coverage, QALY multiplier, and cost per day multiplier, with detailed parameter settings available in
Supplementary Table S1 .All analyses were performed using R (version 4.2.0; R Core Team, Vienna, Austria) with the ‘ABM’, ‘rcea’, ‘hesim’, and ‘ggplot2’ packages. The simulation R code is accessible in the
Supplementary Material . -
The simulation results from our proposed hybrid model are summarized in Table 2 and Figure 2, with comprehensive details provided in
Supplementary Table S1 andSupplementary Figure S1 .Outcome “Adherence” vs. “Volunteer” [Estimate (95% CI)] Incremental vaccination number 824.075 (823.988, 824.162) Decremental infection number 22.589 (22.519, 22.658) Decremental inpatient number 19.656 (19.593, 19.719) Decremental outpatient number 2.933 (2.922, 2.944) Incremental vaccination ratio (%) 133.800 (133.784, 133.816) Decremental infection ratio (%) 16.276 (16.231, 16.320) Decremental inpatient ratio (%) 15.859 (15.814, 15.905) Decremental outpatient ratio (%) 19.746 (19.679, 19.813) WTP threshold (CNY) 85,698 Incremental QALYs 0.091 (0.079, 0.102) Incremental costs (CNY) 3,067 (−3,047, 8,772) Incremental NMB (CNY) 4,699 (−1,939, 11,606) ICER (CNY per QALY) 33,847 Note: The outcome values are for every 1,000 individuals for 5 years.
Abbreviation: CI=confidence interval; CNY=Chinese Yuan; ICER=incremental cost-effectiveness ratio; NMB=net monetary benefit; QALY=quality-adjusted life year; WTP=willingness to pay.Table 2. Summary of the hybrid model simulation results for influenza vaccination strategies.
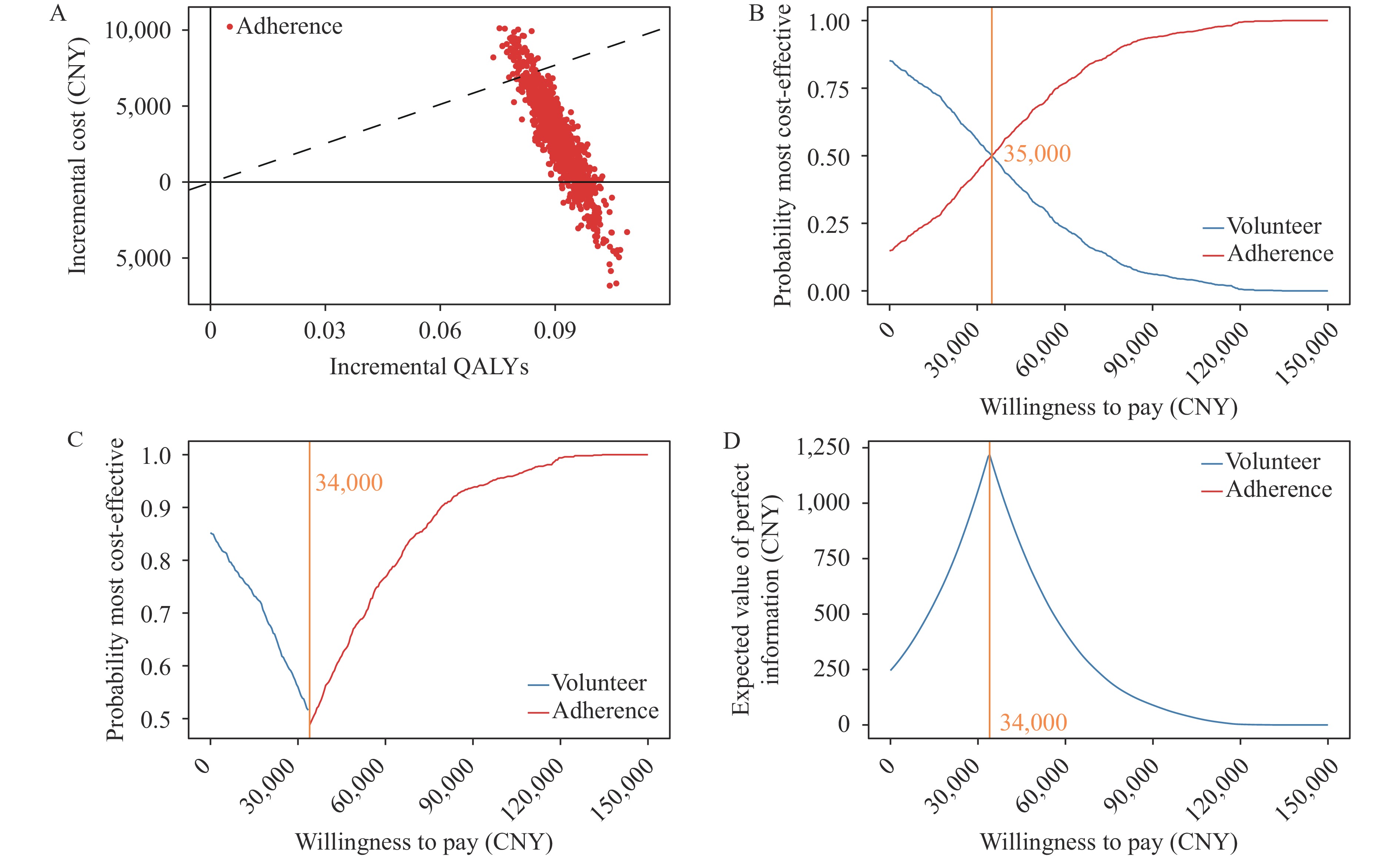 Figure 2.
Figure 2.Cost-effectiveness analysis results for the hybrid model simulations. (A) The cost-effectiveness plane; (B) The cost-effectiveness acceptability curves; (C) The cost-effectiveness acceptability frontier; (D) The expected value of perfect information.
Note: In panel A, the dashed line represents the WTP threshold (85,698 CNY). The costs and QALYs are reported for every 1,000 individuals for 5 years. The population size is N=100,000 with 1,000 simulation replicates.
Abbreviation: CNY=Chinese Yuan; QALY=quality-adjusted life year; WTP=willingness to pay.
Comparative analysis of the “adherence” and “volunteer” vaccination compliance strategies revealed an incremental vaccination ratio of 133.800%, indicating a substantial increase in vaccination coverage. The detailed vaccination coverage rates across cycles are presented in
Supplementary Table S1 andSupplementary Figure S1 . The strategy achieved significant reductions in healthcare utilization, with decremental ratios of 16.276%, 15.859%, and 19.746% for total infections, inpatient cases, and outpatient cases, respectively. These reductions demonstrate the potential public health benefits associated with enhanced vaccination coverage.The economic analysis revealed an incremental cost of 3,067 CNY and an incremental quality-adjusted life year (QALY) gain of 0.091 per 1,000 individuals over the five-year horizon. With a willingness-to-pay (WTP) threshold set at 85,698 CNY (equivalent to the national GDP per capita), the net monetary benefit (NMB) was estimated at 4,699 CNY, yielding an incremental cost-effectiveness ratio (ICER) of 33,847 CNY per QALY gained.
Comparative analysis of the long-term effects demonstrated that the “adherence” strategy exhibited superior cost-effectiveness compared to the “volunteer” strategy. This superiority was evidenced through multiple analytical tools, including the cost-effectiveness plane (CEP), cost-effectiveness acceptability curves (CEACs), cost-effectiveness acceptability frontier (CEAF), and expected value of perfect information (EVPI), across various WTP thresholds with discrete increments of 500 CNY. The results are presented in Figure 2.
The CEP (Figure 2A) illustrates the relationship between incremental QALYs (x-axis) and incremental costs (y-axis), with each point representing a distinct simulation iteration. The WTP threshold (85,698 CNY) is depicted by a dashed line, below which points are considered cost-effective. Analysis revealed that only 7.1% of points were cost-ineffective, while 14.8% demonstrated dominance (both cost-saving and health-improving).
The CEAC (Figure 2B) and CEAF (Figure 2C) demonstrate the probability of each strategy achieving optimal cost-effectiveness across different WTP thresholds. The analysis indicates that the “adherence” strategy demonstrates a higher probability of cost-effectiveness at WTP values exceeding the ICER (33,847 CNY), suggesting its preferential status compared to the “volunteer” strategy.
The EVPI analysis (Figure 2D) quantifies the potential value of acquiring additional information to reduce decision uncertainty. The analysis reveals peak EVPI values near the ICER threshold, indicating that decision-makers might find value in investing in additional research to clarify the cost-effectiveness of these vaccination strategies at this critical threshold point.
The findings of the PSA aligned with the primary analyses. Detailed results are presented in the
Supplementary Tables S3 –S4,Supplementary Figures S2 –S3 .Age group (years old) Cycle (year) Average vaccination coverage rate (%) (95% CI) “Adherence” strategy “Volunteer” strategy All ages 1 13.598 (13.596, 13.600) 13.598 (13.596, 13.600) 2 12.087 (12.085, 12.089) 22.424 (22.421, 22.426) 3 11.988 (11.986, 11.990) 29.895 (29.892, 29.898) 4 11.981 (11.979, 11.983) 36.271 (36.268, 36.274) 5 11.978 (11.976, 11.980) 41.759 (41.756, 41.762) Age group 1 (≤19 years old) 1 25.131 (25.126, 25.137) 25.131 (25.126, 25.137) 2 22.917 (22.911, 22.923) 40.395 (40.388, 40.401) 3 22.705 (22.700, 22.711) 52.522 (52.516, 52.529) 4 22.683 (22.677, 22.689) 62.165 (62.158, 62.171) 5 22.674 (22.669, 22.680) 69.839 (69.833, 69.845) Age group 2 (20–64) 1 6.699 (6.697, 6.701) 6.699 (6.697, 6.701) 2 5.592 (5.590, 5.594) 11.749 (11.747, 11.752) 3 5.562 (5.560, 5.564) 16.523 (16.520, 16.526) 4 5.562 (5.560, 5.564) 21.035 (21.031, 21.038) 5 5.563 (5.561, 5.565) 25.300 (25.297, 25.304) Age group 3 (≥65) 1 26.690 (26.683, 26.697) 26.690 (26.683, 26.697) 2 24.455 (24.448, 24.462) 42.501 (42.493, 42.508) 3 24.220 (24.213, 24.227) 54.884 (54.876, 54.892) 4 24.202 (24.195, 24.209) 64.587 (64.579, 64.595) 5 24.197 (24.190, 24.204) 72.190 (72.183, 72.197) Note: The outcome values are estimated average vaccination coverage percentages. 95% of CIs are obtained by the Clopper and Pearson method (4).
Abbreviation: CI=confidence interval; PSA=probabilistic sensitivity analysis.Table S4. Average vaccination coverage over five annual cycles of the hybrid model PSA results for the influenza vaccination compliance strategies.
-
This study introduces an innovative hybrid modeling framework that integrates a continuous-time agent-based SEIHR model with a Markov model to conduct comprehensive cost-effectiveness analyses of influenza vaccination compliance strategies. Our approach leverages the granularity of continuous-time ABMs for simulating influenza dynamics, offering enhanced precision for modeling individual interactions and disease transmission compared to discrete-time alternatives. The integration with the Markov model enables robust assessment of vaccination compliance across multiple cycles, providing a framework for evaluating long-term strategic outcomes. By more accurately reflecting real-world epidemiological contexts of influenza transmission, this hybrid model overcomes key limitations of traditional models that typically focus on short-term, single-cycle analyses of infectious disease dynamics (1,2,5,6). The versatility of our proposed framework makes it particularly valuable for evaluating a broad spectrum of infectious disease interventions.
Our findings demonstrate that the “adherence” strategy represents a cost-effective alternative to the “volunteer” strategy for influenza vaccination when considering the willingness-to-pay threshold of 85,698 CNY. These results underscore the importance of implementing vaccination compliance strategies that not only enhance vaccination coverage but also mitigate the health burden of influenza in a cost-effective manner.
Despite the robust nature of our hybrid model, several limitations warrant consideration. The assumption of random interactions among agents in the ABM does not fully capture the complexities of real-world contact patterns, including social networks and behavioral determinants. Additionally, the model simplifies certain aspects of influenza transmission dynamics by excluding protective measures, population mobility patterns, and mortality outcomes. The vaccination compliance strategies modeled also represent idealized scenarios, which may limit the generalizability of our findings.
Furthermore, while our model provides innovative insights into vaccination strategies, it has not yet been validated against real-world epidemiological data. As such, our hybrid model should be viewed as a framework to inform public health policy and practice rather than as a direct policy prescription tool. Future research directions include refining the model by incorporating more realistic contact patterns, validating against empirical data, and exploring applications to specific target populations, such as elderly individuals, healthcare workers, and those with comorbidities. The adaptability of our hybrid model framework suggests potential applications beyond influenza vaccination to a broader range of public health interventions. Future investigations could explore the integration of discrete-time agent-based models and decision trees, further enhancing the model’s flexibility and scope.
The primary contribution of this study lies in the development of a flexible hybrid modeling framework capable of evaluating diverse infectious disease interventions. Future research will focus on refining and expanding this framework to better capture the complexities of disease dynamics and vaccination behaviors, ultimately aiming to enhance population-level medical decision-making and public health outcomes.
HTML
| Citation: |

|