
 Download:
Download:




-
Tuberculosis (TB) infection manifests as a prolonged immune response to Mycobacterium tuberculosis (M. tb) exposure without presenting clinical symptoms of TB (1). Between 5% and 15% of these infected individuals are at risk of developing TB disease over their lifetime, thus targeting this reservoir could significantly contribute to TB elimination efforts (2). The Belt and Road Initiative, launched in 2013, has notably enhanced interactions and partnerships between China and various countries, regions, and populations. However, this increased bonding also raises the potential risk of respiratory infections, including TB, largely transmitted via airborne or droplet routes from infected persons (3). This situation highlights the imperative for strengthened TB prevention and control measures within China. Therefore, a comprehensive evaluation of TB infection prevalence and trends in countries along the Belt and Road is essential. Such assessments will help these countries develop robust TB surveillance, prevention, and control strategies, ultimately reducing TB incidence.
As of June 2023, 152 countries had entered into cooperation agreements with China as part of the Belt and Road initiative. Data on the age-standardized prevalence of TB infections from 2013 to 2021, standardized using the global standard population, were obtained from the Global Burden of Disease 2021 (GBD 2021). The trend in TB infection prevalence over this period was analyzed using the estimated annual percentage change (EAPC) and visualized through forest plots. All statistical analyses were conducted using R software (version 4.3.1, R Foundation for Statistical Computing, Vienna, Austria). EAPC was determined by fitting a linear regression model, y = α + βx + ε, where the year served as the independent variable (x) and the natural logarithm of TB infection prevalence as the dependent variable (y). The formula for EAPC is given by EAPC = 100 × (eβ – 1). A negative upper limit of EAPC [95% confidence interval (CI)] signifies a significant declining trend in TB infections, whereas a positive lower limit indicates a significant increasing trend (4).
By June 2023, China had established cooperation agreements through the Belt and Road Initiative with 152 nations across six continents. Table 1 presents the prevalence of TB infection in these countries for 2021, ranked from highest to lowest. The top five countries with the highest TB infection prevalence in 2021 were South Africa, Kiribati, Viet Nam, Solomon Islands, and Papua New Guinea, with prevalence of 44.63%, 43.54%, 43.33%, 41.36%, and 41.31%, respectively. Additionally, Figure 1 shows that most of these countries had a TB infection prevalence between 10% and 30%, with 9 countries (5.92%) having a prevalence below 10% and 8 countries (5.26%) reporting a prevalence of 40% or higher. Regarding the prevalence of TB infection across continents, Oceania exhibited higher infection prevalence, followed by Africa, North America, and Asia, while Europe and South America had comparatively lower prevalence. The top five countries in each continent for TB infection prevalence are shown in
Supplementary Table S1 .Continents N (%) Countries Asia 40 (26.32) Viet Nam(No.3)*, Philippines(No.7)*, Timor-Leste(No.10)*, Myanmar, Indonesia, Cambodia, Malaysia, Sri Lanka, Maldives, Tajikistan, Nepal, Iran, Thailand, Brunei Darussalam, Mongolia, Turkmenistan, United Arab Emirates, Uzbekistan, Yemen, Azerbaijan, Kyrgyzstan, Afghanistan, Georgia, Kazakhstan, Armenia, Turkey, Lao People's Democratic Republic, Saudi Arabia, Pakistan, Palestine, Iraq, Singapore, Republic of Korea, Syrian Arab Republic, Oman, Bahrain, Lebanon, Qatar, Kuwait, Bangladesh Africa 52 (34.21) South Africa(No.1)*, Central African Republic(No.8)*, Uganda, Ethiopia, Democratic Republic of the Congo, Angola, Congo, Seychelles, Egypt, Kenya, Gabon, Lesotho, Equatorial Guinea, Burundi, Eritrea, Mozambique, Madagascar, South Sudan, Guinea-Bissau, Chad, Comoros, Niger, Guinea, Rwanda, Ghana, Burkina Faso, Mali, Zambia, Namibia, Somalia, Sierra Leone, Djibouti, Benin, Cameroon, Togo, Nigeria, Senegal, Cote d'Ivoire, Sudan, Liberia, Morocco, Mauritania, Sao Tome and Principe, Gambia, Libya, Botswana, Tanzania, Cabo Verde, Malawi, Tunisia, Zimbabwe, Algeria Europe 27 (17.76) Ukraine, Moldova, Bulgaria, Russian Federation, North Macedonia, Latvia, Lithuania, Albania, Bosnia and Herzegovina, Romania, Poland, Belarus, Serbia, Slovakia, Hungary, Estonia, Montenegro, Czechia, Croatia, Slovenia, Italy, Greece, Portugal, Malta, Cyprus, Luxembourg, Austria North America 13 (8.55) Honduras, Nicaragua, Dominica, Dominican Republic, El Salvador, Grenada, Panama, Trinidad and Tobago, Jamaica, Costa Rica, Antigua and Barbuda, Barbados, Cuba South America 9 (5.92) Guyana, Suriname, Venezuela, Bolivia, Argentina, Uruguay, Ecuador, Chile, Peru Oceania 11 (7.24) Kiribati(No.2)*, Solomon Islands(No.4)*, Papua New Guinea(No.5)*, Vanuatu(No.6)*, Micronesia(No.9)*, Fiji, Samoa, Tonga, Niue, Cook Islands, New Zealand Note: The asterisks (*) indicate the ranking of the top 10 countries for the prevalence of TB infection among 152 Belt and Road Partner countries.
Abbreviation: TB=Tuberculosis.Table 1. The prevalence of TB infection in 152 Belt and Road Partner countries by continent in 2021, ranked from highest to lowest.
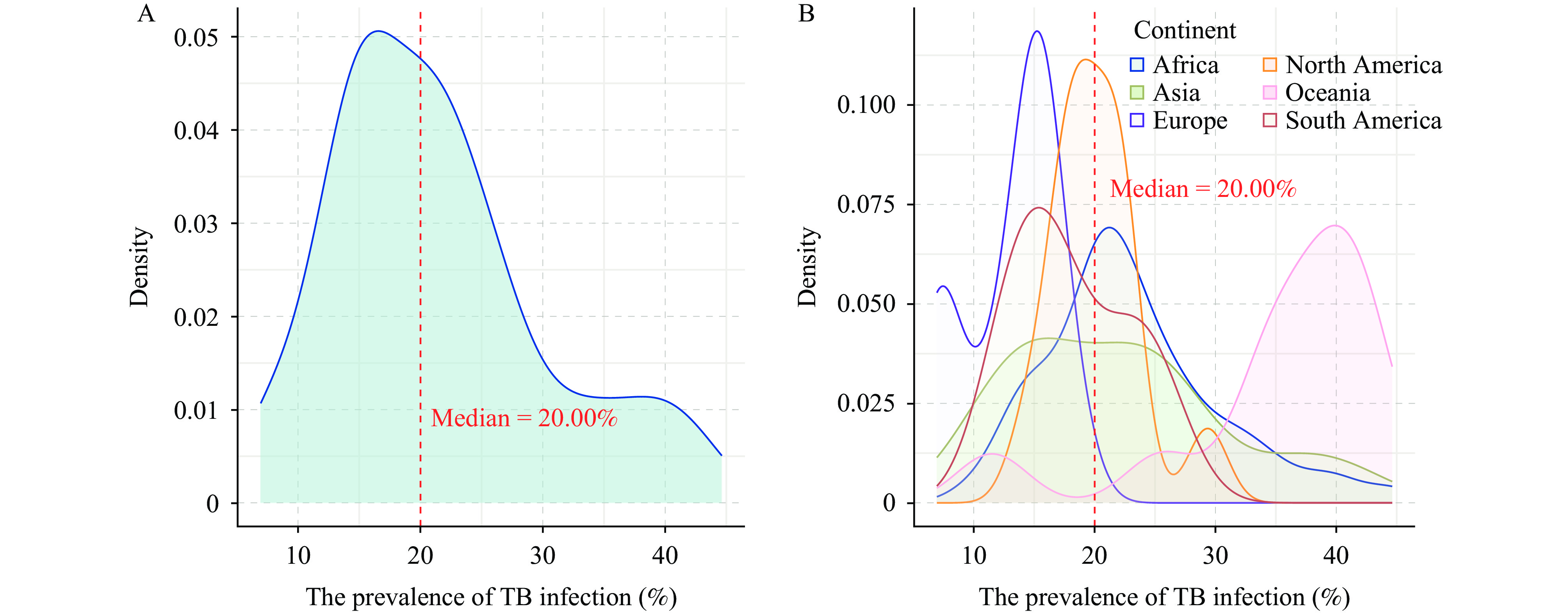 Figure 1.
Figure 1.The prevalence of TB infection in 152 Belt and Road Partner countries in 2021. (A) TB infection prevalence across all countries; (B) TB infection prevalence by continent.Abbreviation: TB = Tuberculosis.
The analysis of TB infection prevalence from 2013 to 2021 revealed a significant declining trend in 149 countries, accounting for 98.03% of the total. As shown in Figure 2 and
Supplementary Table S2 , the top 20 countries with the most pronounced declines were all in Africa, with Mauritania showing the largest decrease (EAPC = −4.48, 95% CI = −4.54, −4.42), followed by Sao Tome and Principe (EAPC = −4.32, 95% CI = −4.41, −4.22), Cote d'Ivoire (EAPC = −4.19, 95% CI = −4.44, −3.93), Cameroon (EAPC = −4.17, 95% CI = −4.32, −4.02), and Djibouti (EAPC = −4.13, 95% CI = −4.27, −3.99). In contrast, countries in Oceania exhibited relatively smaller declines, such as Vanuatu (EAPC = −0.13, 95% CI = −0.18, −0.08), Papua New Guinea (EAPC = −0.12, 95% CI = −0.17, −0.08), and Micronesia (EAPC = −0.11, 95% CI = −0.15, −0.08). Only two countries in Asia exhibited an increasing trend: Sri Lanka (EAPC = 1.19, 95% CI = 1.06, 1.32) and the Philippines (EAPC = 0.04, 95% CI = 0.03, 0.06). However, Timor-Leste (EAPC = −0.02, 95% CI = −0.05, 0.02) in Asia showed no significant change in infection prevalence.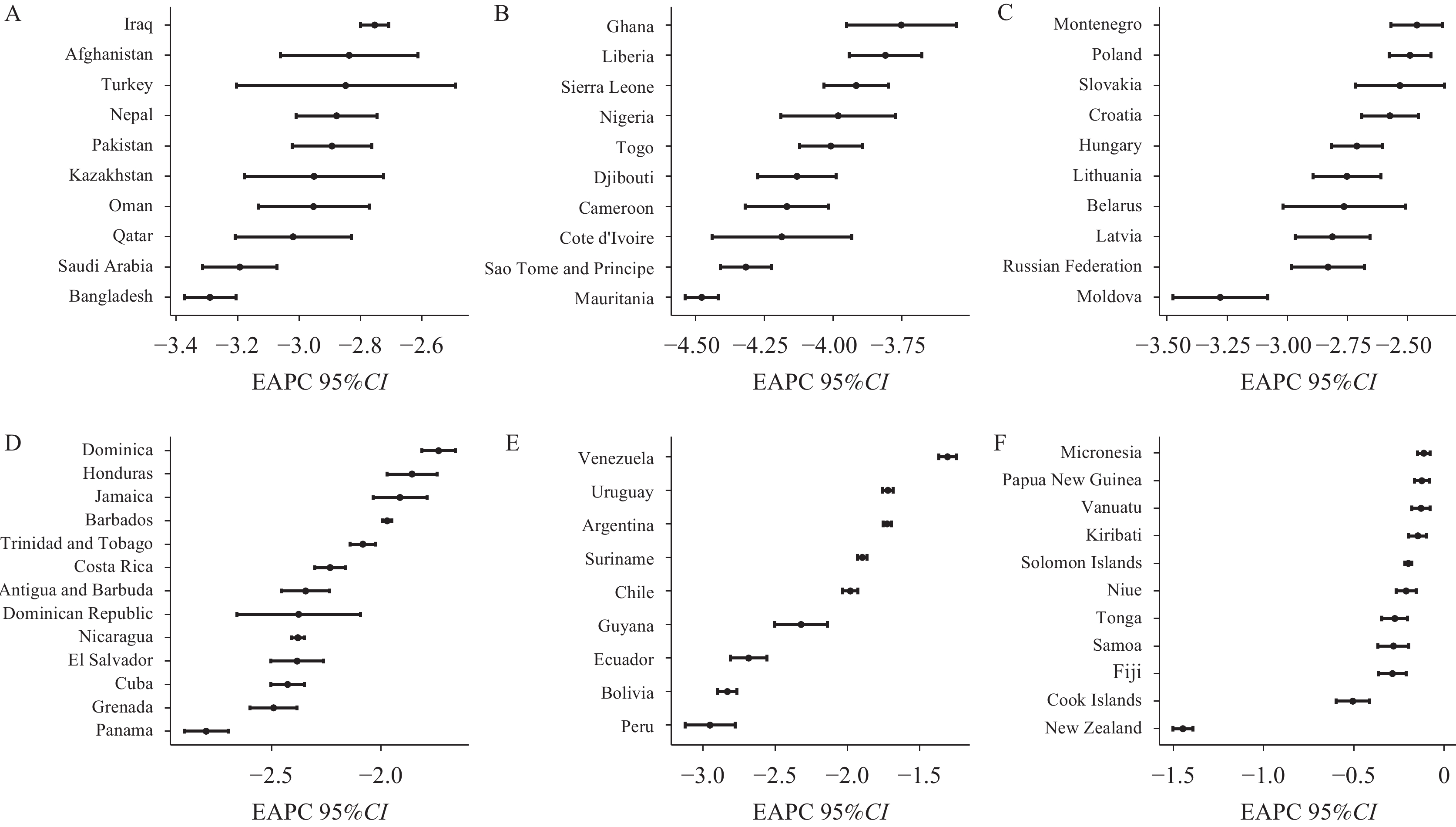 Figure 2.
Figure 2.Epidemic trends of TB infection in 63 Belt and Road Partner countries, 2013-2021. (A) Asia; (B) Africa; (C) Europe; (D) North America; (E) South America; (F) Oceania.
Note: Asia, Africa, and Europe show the distribution of the top 10 countries by descending EAPC absolute values. Abbreviation: TB=Tuberculosis; EAPC= Estimated annual percentage change. -
Achieving the End-TB Strategy by 2035 relies on implementing interventions designed to reduce the incidence of TB. Critical to this effort is the enhancement of surveillance strategies to effectively prevent and control TB infections, as these infections substantially contribute to the development of TB disease.
This study indicates that countries with high TB infection prevalence are predominantly concentrated in Asia, Oceania, and Africa. In particular, the incidence of tuberculosis in certain Oceanian countries, such as Kiribati, continues to exhibit an upward trend (5). This substantial burden may be attributed to low coverage of tuberculosis preventive treatment (TPT). A key factor contributing to this poor TPT coverage, and consequently to the high TB incidence, is the inadequate knowledge among Asian healthcare professionals about the World Health Organization (WHO) and national TB management guidelines and the critical need for monitoring and treating TB in at-risk populations. Additionally, healthcare providers are often hesitant to prescribe TPT to individuals infected with TB due to fears of potential side effects and the emergence of drug resistance (6). Moreover, some regions continue to face shortages in the supply of TB medications. Issues such as drug availability and the lengthy duration of TPT may cause some infected individuals to discontinue their treatment, thereby facilitating ongoing TB transmission (7). In Africa, 34 countries (65.38%) reported a TB infection prevalence of 20% or higher. The continent grapples with challenging economic conditions, widespread poverty, malnutrition, and suboptimal living environments. These socioeconomic factors contribute to the increased vulnerability to TB infection among disadvantaged populations, exacerbated by overcrowded living conditions, limited access to education, and greater social susceptibility. South Africa experiences a significant burden of HIV-associated TB, with the majority of new cases in 2019 being HIV-infected drug-susceptible TB (HIV-DS-TB) (8). Furthermore, in regions heavily burdened by TB, national policies often focus more on managing TB disease rather than controlling TB infection.
This study demonstrated a decline in TB infection prevalence from 2013 to 2021 in the majority of countries (149 out of 152), primarily attributed to enhanced policies and the implementation of coordinated measures. Adherence to WHO guidelines and public health strategies was integral to the effective management of TB infections. However, focusing solely on isolated factors and interventions may be insufficient to improve the current situation of TB infections. Strategic adjustments and the implementation of a multifaceted intervention approach are crucial to reduce the impact of TB infections. Several countries in Southern Africa including Botswana, South Africa, and Zambia, have adopted stringent legal and regulatory measures to curb infections, inclusive TB. Moreover, expanding TB infection screening and promoting TPT is vital for achieving the objectives of the End-TB Strategy.
The prevalence of TB infection in the Philippines and Sri Lanka is on the rise, although the increase is not markedly sharp. The Philippines, ranked fourth worldwide in terms of TB burden, faces considerable challenges. With almost 10 million people residing in urban slums, limited access to education and healthcare heightens the vulnerability to TB infection. A particularly high prevalence of TB is observed among individuals aged 0–24 years, especially within the 10– 24 year-old age group, who are often in densely populated school environments that facilitate TB transmission. Additionally, youth in this age group are more prone to discontinuing TB treatment (9). The increasing incidence of HIV among young people could further aggravate the situation. Given these factors, the Philippine government urgently needs to implement proactive social protections for vulnerable and young populations, utilizing a comprehensive whole-of-society and whole-of-government strategy to address the TB challenges (10).
This study is subject to some limitations. First, the TB infection data were sourced from the GBD website. The accuracy and reliability of our findings depend on the quality and scope of the data used in the modeling process, potentially leading to an overestimation or underestimation of the actual TB infection burden. Moreover, the detailed information and reasons behind the increasing trends observed in certain countries could not be fully explained by the available data. Additionally, the ongoing coronavirus disease 2019 (COVID-19) pandemic has adversely affected access to TB diagnosis and treatment, causing a resurgence in TB infection and disease prevalence in some countries post-2020.
In conclusion, TB infection remains prevalent across all 152 countries participating in the Belt and Road initiative, with the highest rates in Oceania, Africa, and Asia. Fortunately, the majority of these countries are experiencing a declining trend in TB infections. As a staunch supporter and advocate of the Belt and Road initiative, China is committed to collaborating closely with participating nations to maintain high public health standards. Historically, China has been actively involved in cross-border prevention of infectious diseases and in responding to health emergencies. Looking ahead, China is dedicated to reducing TB infections and enhancing TPT efforts. Furthermore, China plans to strengthen existing health policies in collaboration with other countries that have a high burden of TB, and will facilitate the exchange of technologies related to the diagnosis, treatment, prevention, and control of TB. Additionally, it will promote collaborative scientific research and the development of health resources to further the achievement of the End-TB Strategy.
HTML
| Citation: |

|