
 Download:
Download:




-
Under globalization, emerging infectious diseases (EIDs) can spread rapidly across countries and regions in a short time (1). Prioritization decisions for prevention and management are critical when facing potential outbreaks of EIDs. Responding to and controlling epidemics is costly due to limited resources and time. Risk assessment is the most common tool for assessing and responding to outbreaks of EIDs. It helps to identify risk factors, detect high-risk areas and possible spreaders, and enable health workers to take timely action to prevent and curb the spread of infectious disease.
Common risk assessment methods include expert consultation, Delphi, risk matrix, and analytical flowcharting. However, these methods have limitations (2). For example, the Delphi method requires complex preparation and consumes substantial time, human resources, and materials. Risk matrix is a decision support tool for visualizing and prioritizing risks (3). The Borda count method enables ranking risk events within the same risk level identified using a risk matrix (4–5). The integrated application of these two methods can guide resource allocation and has been used in diverse fields such as economics, medicine, engineering, business, and space operations (3,6). However, their application in assessing the importation risk of EIDs is limited.
In recent years, international cooperation for trade and personnel exchange between China and numerous countries has increased following the implementation of the “Belt and Road” initiative launched by China in 2013 (4,7). This increased interaction facilitates the cross-border transmission of EIDs. Lassa fever (LF) remains a substantial health concern in West Africa, presenting as an acute viral hemorrhagic illness with a high case fatality rate of 15%–30% (8-9). The virus transmits to humans through direct or indirect contact with infected rodents or contaminated materials (8). Severe infections manifest as respiratory distress, mucosal bleeding, hearing loss, and multiorgan failure. Generally, all populations are susceptible to LF (8). Currently, no licensed vaccines or specific treatments are available (8). From 1996 to 2023, over 50 outbreaks of LF occurred in West Africa, with at least 18 imported cases of LF reported in several European countries (1). Notably, previously reported imported cases were primarily travelers and physicians diagnosed with LF after returning from epidemic areas (1). However, the importation risk of LF to China remains unclear. Therefore, this study used LF as an example to illustrate the application of risk matrix and Borda count method in assessing the risk of EIDs being imported to China.
-
This study assessed the risk of EIDs importation using a mixed-methods approach, combining multi-source data with a risk matrix and Borda count method.
-
Data were obtained from the World Health Organization Disease Outbreak News (1), which includes the number of LF cases, deaths, imported cases, and fatality rates from 9 African countries from 1996 to 2023. Data on the annual number of African students in China were obtained from the 2018 Concise Statistics of International Students in China dataset (10). Data on the annual number of inbound and outbound tourists were obtained from the United Nations World Tourism Organization (11). Data on the number of persons sent for foreign economic cooperation, including the number of foreign contracted workers and personnel for labor service cooperation, were obtained from the China Statistical Yearbook 2019 (12) (Table 1).
Country Cumulative cases Cumulative fatality rate (%) The number of African students entering China The number of African tourist arrivals to China by country The number of persons sent by China to African countries for economic cooperations The number of outbound Chinese tourist arrivals to African countries The time lag between the latest outbreak of Lassa fever and 2024 by country (years) Benin 125 24.00 634 4,503 917 10,233 8 Guinea 2 0 861 8,695 2,838 4,993 2 Liberia 39 41.03 802 3,832 2,954 NA 6 Nigeria 9,906 8.74 6,845 45,367 6,694 151,616 1 Sierra Leone 1,160 18.88 983 4,276 275 2,014 5 Togo 2 0 <500 4,517 83 6,490 2 Burkina Faso 1 100.00 <500 7,871 226 2,765 7 Ghana 14 7.14 6,475 22,890 963 7,917 1 Mali 2 0 788 4,868 422 4,671 7 Note: The number of African students entering China, the number of African tourist arrivals to China by country, the number of persons sent by China to African countries for economic cooperations, and the number of outbound tourists from China arriving in African countries: above data available were from the year of 2018; Cumulative cases and cumulative fatality rate (%) of Lassa fever are from the year of 1996–2023.
Abbreviation: NA=not appliable.Table 1. Variables for the importation risk assessment of Lassa fever.
-
A risk matrix was applied to assess the risk of LF importation to China based on two dimensions: importation possibility and severity (Table 2) (4). Based on literature reviews (8,13-14), key indicators of these dimensions were identified. Importation possibility indicators included the time lag in years between the latest LF outbreak and 2024 and the number of cross-border migrants, including foreign students, tourists, labor workers, and other workers. Importation severity indicators included cumulative cases and the cumulative fatality rate. Scores for the risk assessment indicators were then determined in three steps. First, previous literature on infectious disease importation risk was reviewed (4). Second, the epidemiological characteristics of LF and the major populations undergoing cross-border mobility between China and Africa were summarized. Finally, expert consultation and discussion were conducted. Detailed information is shown in Table 3.
Importation possibility Importation severity Negligible Minor Moderate Severe Catastrophic Inevitable H H E E E Likely M H H E E Possible L M H E E Unlikely L L M H E Rare L L M H H Abbreviation: L=low importation risk; M=moderate importation risk; H=high importation risk; E=extremely high importation risk. Table 2. Risk matrix assessment index.
Assessment indicators Factors Classification Risk score Importation possibility The time lag between the latest outbreak of Lassa fever and 2024 by country (years) ≤1 5 2–3 4 4–5 3 6–9 2 ≥10 1 The number of African students entering China ≤999 1 1,000–4,999 2 5,000–9,999 3 10,000–14,999 4 ≥15,000 5 The number of African tourist arrivals to China by country ≤4,999 1 5,000–9,999 2 10,000–29,999 3 30,000–49,999 4 ≥50,000 5 The number of persons sent by China to African countries for economic cooperations ≤999 1 1,000–2,999 2 3,000–4,999 3 5,000–9,999 4 ≥10,000 5 The number of outbound Chinese tourist arrivals to African countries ≤4,999 1 5,000–9,999 2 10,000–49,999 3 50,000–149,999 4 ≥150,000 5 Importation severity Cumulative cases (cases) ≤49 1 50–499 2 500–999 3 1,000–4,999 4 ≥5,000 5 Cumulative fatality rate (%) ≤9 1 10–29 2 30–49 3 50–69 4 ≥70 5 Note: The number of African students entering China, the number of African tourist arrivals to China by country, the number of persons sent by China to African countries for economic cooperations, and the number of outbound Chines tourist arrivals to African countries: above data available were from the year of 2018; Cumulative cases and cumulative fatality rate (%) of Lassa fever are from the year of 1996–2023. Table 3. Risk assessment indicators of importation possibility, severity, and corresponding scores.
The formulas for importation possibility and severity of LF are as follows. First, the importation possibility score was calculated as: the score of the time from the last outbreak to 2024 + (the score of the number of African students entering China × 30% + the score of the number of African tourist arrivals to China × 30% + the score of the number of persons sent for African economic cooperation × 20% + the score of the number of Chinese tourist arrivals to Africa × 20%). This study then derived the importation possibility risk score using 5 levels: rare (0–2 points); unlikely (3–4 points); possible (5–6 points); likely (7–8 points); and inevitable (9–10 points). The time lag in years between the latest outbreak of LF and 2024 was calculated by country as 2024 minus the outbreak year. Second, the importation severity score was calculated as the cumulative case score plus the cumulative fatality rate score. Cumulative cases were equal to the total number of cases in countries with LF from 1996 to 2023.
$$\begin{aligned} & {\mathrm{Cumulative\; fatality\; rates}} = \\ & \dfrac{{\mathrm{cumulative\; deaths\; from\;1996\;to\;2023}}}{{\mathrm{cumulative\;cases\;from\;1996\;to\;2023}}} \times 100\% \end{aligned}$$ This study classified the final importation severity risk score into 5 levels: negligible (0–2 points); minor (3–4 points); moderate (5–6 points); severe (7–8 points); and catastrophic (9–10 points). Third, according to the importation possibility and severity levels in the risk matrix assessment index (Table 2), the importation risk of LF into China was divided into 4 levels (low, moderate, high, and extremely high), which corresponded to green, yellow, orange, and red zones, respectively. Finally, this study used the Borda count method to rank the LF importation risk (4).
-
This study used the Borda count method (4-5) to rank LF importation risks. First, the Borda points for each importation risk were calculated as the sum of the rank of its importation possibility and the rank of its severity risk level. This study then sorted the Borda points from largest to smallest and assigned corresponding counts of 0, 1,…, N-1. A lower Borda count indicates a greater likelihood of LF importation to China and potentially more severe consequences. Borda points were calculated using the following formula:
$$ {b}_{i}=\sum _{k=1}^{m}(N-{r}_{ik}) $$ Where N equals the total number of at-risk countries, this study defined at-risk countries as those with LF importation risk. Therefore, this study set N as 9. The variable m equals the 2 dimensions of risk assessment.
$ {r}_{ik} $ equals the number of countries posing a higher risk than the risk for indicator i under criterion k, and$ {b}_{i} $ equals the Borda points of assessment indicator i. -
This study scored and ranked the risk of LF importation from 9 countries that experienced LF outbreak from 1996 to 2023. It considered global importation possibility and severity to derive overall importation risks (Table 4). Using a risk matrix diagram, this study then visualized these total risks, with red, orange, yellow, and green representing extremely high, high, moderate, and low importation risk, respectively (Figure 1). Its integrated application of the risk matrix and Borda count method demonstrated that China faces a risk of LF importation. Regarding importation possibility, Nigeria presented the highest risk (score=8.7), while Mali presented the lowest (score 3.0). Concerning importation severity, Nigeria, Sierra Leone, and Burkina Faso exhibited the highest risk (score=6), whereas Mali had the lowest (score=2) (Table 4). Nigeria posed the highest LF importation risk (Figure 1) due to the highest Borda points of 18 and ranking first. Sierra Leone, Burkina Faso, and Ghana presented moderate importation risks, while Guinea, Togo, Benin, Liberia, and Mali had low importation risks (Figure 1). Mali exhibited the lowest Borda points of 9 and ranked ninth (Table 4).
Country name The importation possibility score The importation severity score Risk levels Borda points Borda
countRisk sequence of importation Nigeria 8.7 6 H 18 0 1 Sierra Leone 4.0 6 M 14 1 2 Burkina Faso 3.3 6 M 14 2 2 Ghana 7.4 2 M 13 3 4 Guinea 5.5 2 L 11 4 5 Togo 5.2 2 L 11 5 5 Benin 3.4 4 L 11 6 7 Liberia 3.2 4 L 11 7 7 Mali 3.0 2 L 9 8 9 Abbreviation: L=low importation risk; M=moderate importation risk; H=high importation risk; E=extremely high importation risk. Table 4. Importation risks from countries with Lassa fever outbreaks to China from 1996–2023.
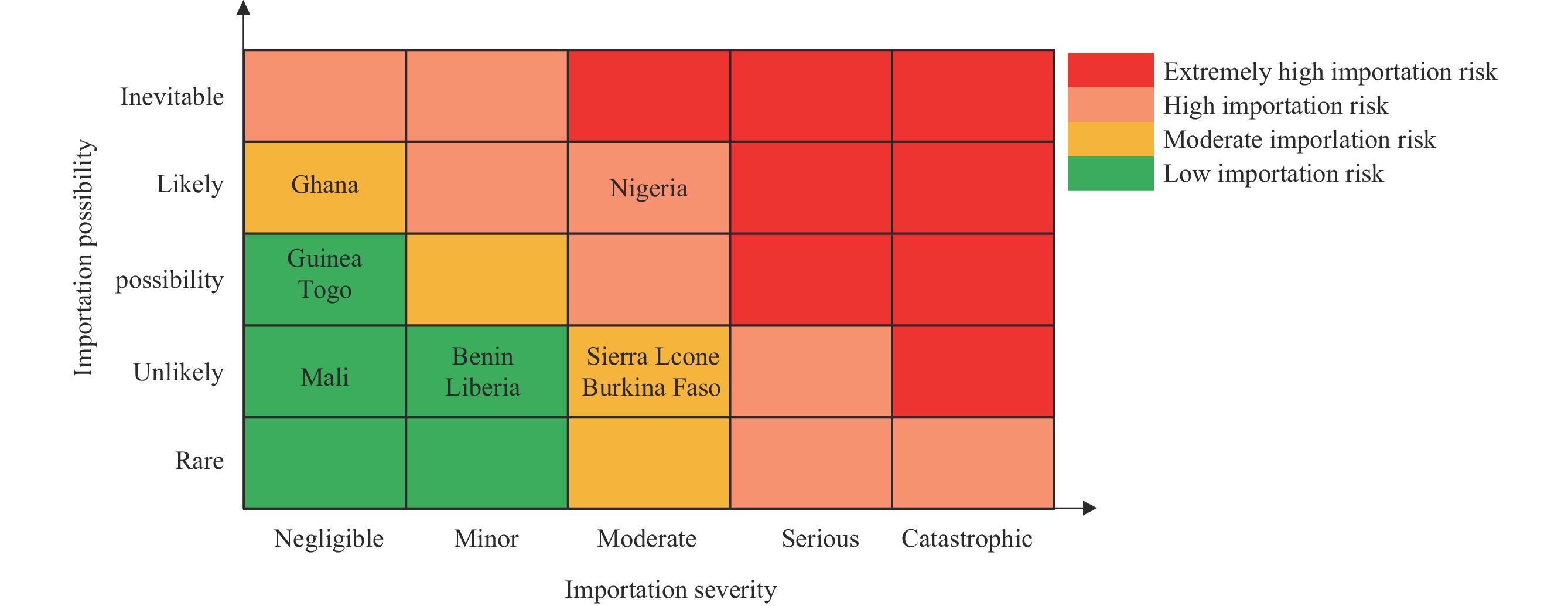 Figure 1.
Figure 1.Importation risk of Lassa fever.
-
Risk assessment is foundational to preventing and containing the spread EIDs, and the risk matrix and Borda count method seem to be promising tools for assessing the importation risk of a disease. This study attempted to assess the importation risk of EIDs to China, using LF as an example. Its authors believe that the method applied in this study may significantly supplement expert consultation and Delphi methods. Additionally, the method is more suitable for application in the early stages of a disease outbreak and offers advantages in assessing the potential risk of outbreaks under conditions of limited information and multi-source data.
This study leveraged multi-source data from multiple sectors, including tourism, international students, and cross-border labor, in addition to the health sector. Incorporating data such as flight information and the number of entrants from epidemic areas into the risk matrix could increase the accuracy of risk assessments. Furthermore, the effectiveness of the risk assessment hinges on the quality, timeliness, and type of multi-source data used; more comprehensive, timely, and accurate data sources yield more reliable results.
In this study, it was found that Nigeria presented a high risk of LF importation to China, with moderate importation severity and likely importation possibility. Currently, the LF epidemic status in Nigeria is worrisome. A significant increase in the number of suspected and confirmed LF cases was reported in Nigeria from 2021 to 2023 (1,14). LF infection rates exhibited seasonal variability in Nigeria, with significantly higher rates in the dry season than in the wet season (15). During the dry season, human activities such as bush burning are commonly practiced in the Forest and Savannah regions to hunt rodents, including Mastomys natalensis, for food (15). Mastomys natalensis, a natural host of Lassa virus, has a high reproductive rate in West Africa and plays a significant role in rodent-to-human transmission of the virus (8,15). Bush burning destroys rodent habitats, encouraging their movement from bushes to human dwellings in search of shelter and food, which may increase the risk of LF exposure for humans (15). Other factors, including nosocomial transmission, travel and migration, inadequate public health infrastructure, the effects of civil war and conflict, and social factors may also contribute to the re-emergence of LF epidemics in Nigeria (14). Additionally, among nine countries, Nigeria has the largest number of entrants to China, including international students and tourists. China has also sent a large number of workers to Nigeria for economic cooperation projects, and many Chinese tourists travel to Nigeria. Globalization and the implementation of China’s “Belt and Road” strategy will likely lead to a significant increase in the volume and speed of travel between the two countries (4,7). Consequently, the cross-border spread of LF is facilitated.
In this study, the risk matrix and Borda count method were applied to assess the importation risk of LF to China and distinguish risk levels. High-risk importation areas can thus be quickly identified. These results facilitate the government to make plans, allocate limited resources, and develop preventive strategies for LF. Furthermore, the risk matrix and Borda count method may be used to assess and rank the risk of various imported EIDs with descending order of risk. This ranking can then inform the determination of the disease with the highest risk. The final risk assessment results may provide evidence for China to develop and optimize preparedness strategies, improve the efficiency of risk management and infectious disease prevention, and help prevent or curb future outbreaks. Currently, the Chinese Center for Disease Control and Prevention has established a risk assessment group (16). This group uses expert consultation to assess the risk of public health emergencies that may occur in or be imported from abroad each month (16). Finally, the integrated application of the risk matrix and Borda count method presented in this study may enrich the current toolbox of public health countermeasures and inform future risk management of imported EIDs.
This study has some limitations. First, while this study introduced the integrated risk matrix and Borda count method, other methods exist but were not included. Additionally, expert consultation and Delphi methods should be employed to assess the importation risk of EIDs more comprehensively. Second, this study focused on LF importation risk for the entire Chinese population. Due to the unavailability of cross-national data for the whole population, the populations used to assess LF importation risk — students, tourists, businesspeople, and laborers — were primarily young and middle-aged adults. Compared with the whole population, these groups may have a lower LF importation risk due to better hygiene knowledge and protection awareness, stronger immunity, and a lower LF infection risk. Therefore, the actual levels in this study may be underestimated. Finally, the risk matrix relies on multi-source data; the wider and more accurate the data sources, the better the model's application. This study used LF, a skin-to-skin contact infection, as an example. The risk matrix and Borda count method can also be applied to the importation risk assessment of vector-borne diseases and infectious diseases with other transmission types. For example, assessing malaria would require data on the host, medium, climate, and environment.
HTML
Data Acquisition
Risk Matrix Assessment

Borda Count Method



| Citation: |

|