
 Download:
Download:




-
Candida auris (C. auris) has emerged as a significant global public health threat, leading to its classification as a Critical Priority pathogen by the World Health Organization (WHO) (1). Outbreaks of C. auris have been reported in several provincial-level administrative divisions (PLADs) in China, including Liaoning, Anhui, and Guangdong (2). This study identified 17 nosocomial cluster cases of C. auris at a teaching hospital in Beijing Municipality between March and September 2023. Whole-genome sequencing revealed a novel C. auris sublineage responsible for this outbreak, highlighting its dissemination within the city.
-
This outbreak was identified at CY Hospital, a tertiary teaching hospital in Beijing with 2,500 inpatient beds. The first C. auris case was identified on March 2, 2023, from the urine sample of a 78-year-old male patient (Pt01). Pt01 was admitted to the emergency intensive care unit (EICU) due to coronavirus disease 2019 (COVID-19), followed by severe bacterial pneumonia. He underwent a tracheotomy and was discharged on day 6 after the first positive C. auris culture. However, Pt01 was readmitted on March 31, 2023, due to an influenza A infection. During his second hospital stay, C. auris was cultured 4 times from the patient’s urine samples and once from his central venous catheter (Figure 1 and
Supplementary Table S1 ).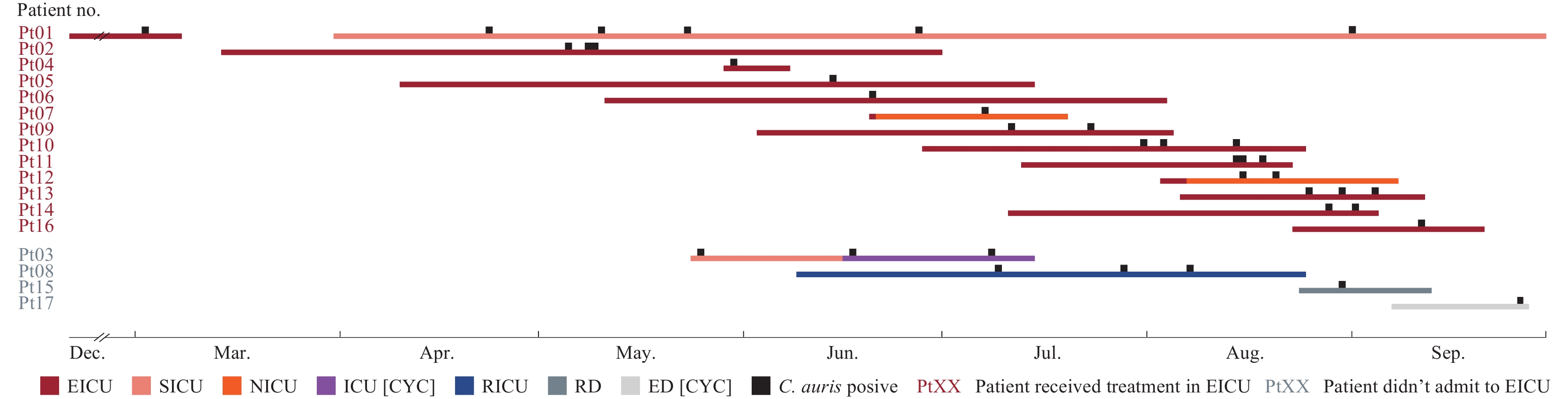 Figure 1.
Figure 1.Epidemiological timeline of Candida auris (C. auris)–positive cases identified in the CY Hospital.
Note: This timeline tracked the hospitalization duration and specific clinical wards for each patient and the C. auris culture–positive timepoints. Pt01 was admitted to the Emergency Intensive Care Unit of the hospital on December 23, 2022, and the first C. auris was isolated from Pt01 on March 2, 2023. Till September 30, 2023, 17 C. auris–positive patients were identified in total.Between March and September 2023, C. auris isolates were detected in an additional 16 patients (Pt02 to Pt17) at this hospital (Figure 1 and Supplementary Table S1). A total of 38 C. auris strains were collected from the 17 patients (Figure 2 and
Supplementary Table S2 ). The hospital’s microbiology laboratory and infection prevention team conducted a retrospective study to investigate transmission. A review of patient medical records indicated that of the 17 patients, 82.4% (14/17) were male, and 88.2% (15/17) were older than 65 years. Moreover, 82.4% (14/17) were critically ill. Notably, 76.5% (13/17) of patients had confirmed C. auris infections, including 29.4% (5/17) with candidemia and 23.5% (4/17) with C. auris colonization. Additionally, 70.6% (12/17) of patients had ≥1 positive urine culture (Supplementary Table S1 ). Figure 2.
Figure 2.Analysis of Clade I Candida auris (C. auris) isolates in China based on whole-genome sequencing. (A) Phylogenetic tree of C. auris Clade I isolates. (B) Heatmap based on genome-wide pairwise SNP analysis, with the order of strains in rows (from top to bottom) and the order in the phylogenetic tree in columns (from left to right).
Note: The first C. auris Clade I strain reported in Beijing (BJCA001) was used as root of the phylogenetic tree.Patient no. Gender Age (years) Critical condition Experienced treatment in EICU Infection or colonization Outcome Date admitted to the hospital Hospitalization days to first isolation of C. auris No. of C. auris isolates cultured from Total Urine Blood CVC Drainage Pus BALF Pt01 Male 78 Yes Yes Infection Not improved 2022/12/23 70 6 5 1 Pt02 Female 86 Yes Yes Infection Dead 2023/3/14 53 3 1 1 1 Pt03 Male 71 Yes No Infection Improved 2023/5/24 2 2 2 Pt04 Female 79 Yes Yes Colonization Not improved 2023/5/29 2 1 1 Pt05 Male 26 Yes Yes Infection Not improved 2023/4/10 66 1 1 Pt06 Female 86 Yes Yes Infection Improved 2023/5/11 41 1 1 Pt07 Male 67 Yes Yes Infection Improved 2023/6/20 18 1 1 Pt08 Male 67 Yes No Colonization Dead 2023/6/9 31 3 3 Pt09 Male 78 Yes Yes Infection Improved 2023/6/3 39 2 2 Pt10 Female 82 Yes Yes Infection Improved 2023/6/28 34 3 3 Pt11 Male 81 Yes Yes Infection Dead 2023/7/13 33 3 1 1 1 Pt12 Female 74 Yes Yes Infection Not improved 2023/8/3 13 2 2 Pt13 Male 52 Yes Yes Infection Dead 2023/8/6 20 4 1 1 1 Pt14 Female 83 Yes Yes Infection Dead 2023/7/11 49 3 1 2 Pt15 Female 84 No No Colonization Improved 2023/8/24 7 1 1 Pt16 Female 75 Yes Yes Infection Not improved 2023/8/23 20 1 1 Pt17 Male 74 No No Colonization Not improved 2023/9/7 21 1 1 Abbreviation: C. auris =Candida auris; BALF=bronchoalveolar lavage fluid; CVC=central venous catheter. Table S1. Information on 17 C. auris–positive patients from the CY Hospital.
The median duration from patient admission to the first isolation of C. auris isolates was 31 days, with an interquartile range of 16–45 days. To better understand the characteristics of C. auris nosocomial transmission at the hospital, the investigation team summarized the hospitalization timelines and associated department associations for the 17 positive patients. The investigation revealed that 76.5% (13/17) of patients had a documented history of receiving treatment in the EICU ward, indicating that the EICU may potentially mediate the spread of C. auris in the hospital (Figure 1). However, 168 culture-based environmental microbiologic surveillance cultures from the EICU ward, including samples collected before routine ward disinfections, yielded no positive results for C. auris. The team also conducted an on-site evaluation focused on infection prevention and control practices in the unit, including the use of personal protective equipment, hand hygiene, processing of reusable medical equipment, and environmental cleaning and disinfection. In general, healthcare personnel adhered to infection control regulations. However, the investigators also observed potential opportunities for contamination of mobile medical devices during patient care and that equipment surface disinfection was sometimes not properly done, which may facilitate the transmission of C. auris.
To provide more credible evidence, whole-genome sequencing (WGS) was performed on all 38 isolates using the Illumina Nova 6000 platform in PE150 (150-bp paired-end) sequencing mode (Beijing Novogene Bioinformatics Technology Co., Ltd., China). Additionally, the genomes of 54 Clade I C. auris isolates previously reported in China were acquired from the public database (
Supplementary Table S3 ). Single nucleotide polymorphism (SNP) calling and phylogenetic analysis based on WGS data were performed as described previously using the genome of C. auris B8441 (GCA_002759435.2_Cand_auris_B8441_V2) as the reference. Detailed laboratory investigation methods are provided inSupplementary Material (3).WGS analysis revealed that all C. auris strains from CY Hospital during this period belonged to Clade I, with 15 to 100 pairwise SNPs between strains (Figure 2). For isolates from the same patient, pairwise SNPs were consistently ≤50. Compared with the genomes of C. auris Clade I strains previously reported in China, the strains in this study were genetically similar to those identified from 2 other hospitals in Beijing after 2021 (pairwise SNPs ≤100) but significantly divergent from the first C. auris Clade I case reported in Beijing in 2018 (pairwise SNPs >1,000) (Figure 2B). The strains from CY Hospital were also phylogenetically distant from the sublineage of C. auris Clade I isolates from the eastern China region (Anhui, Jiangsu, and Shandong provinces) and the outbreak strains recorded in Hong Kong Special Administrative Region (SAR), China, in 2019. Additionally, the strains isolated from 12 of the 13 patients who received treatment in the EICU exhibited more conserved genomic features (pairwise SNPs ≤50) compared with phylogenetic variations against strains from other departments in CY Hospital and other hospitals in Beijing (Figure 2). This molecular evidence further suggests that the rapid dissemination of C. auris within the EICU may facilitate nosocomial transmission.
Antifungal susceptibility testing suggested that all isolates from CY Hospital were resistant to fluconazole and amphotericin B, according to US CDC tentative breakpoints (Supplementary Table S2). Moreover, WGS analysis revealed that all strains carried the amino acid substitutions Y132F on Erg11 and A583S on Tac1b, both of which are presumed to be associated with azole resistance (4-5). Of note, the Erg11 Y132F substitution was present in 100% of strains from the Beijing and eastern China sublineages, and 84.2% of strains from the Hong Kong SAR sublineage carried this substitution. In contrast, the Tac1b A583S substitution was found exclusively in the Beijing sublineage and was absent in both the eastern China and Hong Kong sublineage isolates. Additionally, 3 strains from different patients (strains Pt03B, Pt04A, and Pt17A) were echinocandin-resistant, and a key substitution, S639F, on Fks1 (6) was observed in 2 of these 3 strains. The overall outcome for these 17 patients was poor, with 35.3% (6/17) of patients dying in the hospital and 29.4% (5/17) showing no improvement before discharge (
Supplementary Table S1 ).Strain no. Patient no. Department
of isolationDate of
samplingSpecimen
typeAntifungal susceptibility (minimum inhibitory concentration, mg/L)* Genome
accession no.Key substitutions Fluconazole Voriconazole Itraconazole Posaconazole Amphotericin B Caspofungin Micafungin Anidulafungin 5-Flucytosine Erg11 Fks Pt01A Pt01 EICU 2023/3/2 Urine 128 0.5 0.12 0.03 4 0.12 0.12 0.12 0.12 SRR29824987 Y132F Pt01B Pt01 SICU1 2023/4/23 Urine 256 0.5 0.12 0.03 4 0.5 0.12 0.25 0.12 SRR29824986 Y132F Pt01C Pt01 SICU1 2023/5/10 Urine 256 0.5 0.25 0.06 2 0.25 0.12 0.25 <0.06 SRR29824972 Y132F Pt01D Pt01 SICU1 2023/5/23 Urine 256 0.5 0.25 0.03 2 0.5 0.12 0.25 0.12 SRR29824961 Y132F Pt01E Pt01 SICU1 2023/6/27 Urine 128 0.5 0.12 0.03 2 0.5 0.12 0.25 0.12 SRR29824951 Y132F Pt01F Pt01 SICU1 2023/9/2 CVC 256 0.5 0.12 0.06 2 0.5 0.12 0.25 0.12 SRR29824950 Y132F Pt02A Pt02 EICU 2023/5/5 Drainage 128 0.5 0.12 0.03 4 0.12 0.12 0.25 0.06 SRR29824949 Y132F Pt02B Pt02 EICU 2023/5/8 Urine 128 0.25 0.06 0.03 2 0.12 0.12 0.12 0.12 SRR29824983 Y132F Pt02C Pt02 EICU 2023/5/9 CVC 128 0.5 0.12 0.03 4 0.12 0.12 0.12 0.12 SRR29824982 Y132F Pt03A Pt03 SICU2 2023/5/25 Urine 256 0.5 0.12 0.03 4 0.12 0.12 0.12 0.12 SRR29824981 Y132F Pt03B Pt03 ICU2 [CYC] 2023/6/17 Urine 128 0.25 0.06 0.03 4 8 >8 >8 <0.06 SRR29824985 Y132F S639F Pt04A Pt04 EICU 2023/5/30 Urine 128 0.5 0.06 0.03 2 4 >8 4 0.12 SRR29824984 Y132F S639F Pt05A Pt05 EICU 2023/6/14 Pus 256 1 0.12 0.06 4 0.12 0.12 0.12 0.12 SRR29824980 Y132F Pt06A Pt06 EICU 2023/6/20 CVC 128 0.5 0.12 0.03 4 0.12 0.12 0.12 0.12 SRR29824979 Y132F Pt07A Pt07 NICU 2023/7/7 Pus 256 1 0.25 0.06 2 0.25 0.25 0.25 0.12 SRR29824978 Y132F Pt08A Pt08 RICU 2023/7/9 Urine >256 1 0.25 0.06 2 0.12 0.12 0.12 <0.06 SRR29824977 Y132F Pt08B Pt08 RICU 2023/7/28 Urine >256 1 0.25 0.12 4 0.12 0.12 0.12 0.12 SRR29824976 Y132F Pt08C Pt08 RICU 2023/8/7 Urine >256 1 0.12 0.06 2 0.12 0.12 0.12 <0.06 SRR29824975 Y132F Pt09A Pt09 EICU 2023/7/11 Urine 128 0.25 0.12 0.03 2 0.06 0.12 0.12 <0.06 SRR29824974 Y132F Pt09B Pt09 EICU 2023/7/23 Urine 128 0.25 0.06 0.03 2 0.12 0.12 0.12 0.06 SRR29824973 Y132F Pt10A Pt10 EICU 2023/7/31 Urine 128 0.5 0.06 0.03 4 0.12 0.12 0.12 0.12 SRR29824971 Y132F Pt10B Pt10 EICU 2023/8/3 Urine 256 1 0.25 0.06 4 0.25 0.12 0.25 0.12 SRR29824970 Y132F Pt10C Pt10 EICU 2023/8/14 Urine 256 2 0.25 0.06 2 0.25 0.12 0.25 0.12 SRR29824969 Y132F Pt11A Pt11 EICU 2023/8/14 Urine 128 0.25 0.06 0.03 4 0.06 0.12 0.12 0.06 SRR29824968 Y132F Pt11B Pt11 EICU 2023/8/15 BALF 256 1 0.12 0.12 4 0.12 0.12 0.12 0.12 SRR29824967 Y132F Pt11C Pt11 EICU 2023/8/18 Blood 128 0.5 0.12 0.03 4 0.12 0.12 0.12 0.12 SRR29824966 Y132F Pt12A Pt12 NICU 2023/8/15 Blood >256 0.5 0.12 0.03 4 0.25 0.25 0.12 <0.06 SRR29824965 Y132F Pt12B Pt12 NICU 2023/8/20 Blood 256 1 0.25 0.06 2 0.5 0.12 0.25 0.12 SRR29824964 Y132F Pt13A Pt13 EICU 2023/8/25 Blood 256 0.5 0.12 0.03 4 0.12 0.12 0.12 0.12 SRR29824963 Y132F Pt13B Pt13 EICU 2023/8/25 CVC 128 0.5 0.12 0.03 4 0.12 0.12 0.12 0.12 SRR29824962 Y132F Pt13C Pt13 EICU 2023/8/30 Wound 256 0.5 0.12 0.03 4 0.12 0.12 0.12 0.12 SRR29824960 Y132F Pt13D Pt13 EICU 2023/9/4 Urine 256 0.5 0.12 0.03 4 0.12 0.12 0.12 0.12 SRR29824959 Y132F Pt14A Pt14 EICU 2023/8/28 Blood 128 0.5 0.12 0.03 4 0.12 0.12 0.12 0.12 SRR29824958 Y132F Pt14B Pt14 EICU 2023/9/1 Urine 256 0.5 0.12 0.03 4 0.12 0.12 0.25 0.12 SRR29824957 Y132F Pt14C Pt14 EICU 2023/9/1 Blood 256 0.5 0.25 0.06 2 0.25 0.12 0.25 0.12 SRR29824956 Y132F Pt15A Pt15 RD2 2023/8/30 Urine 128 0.5 0.12 0.06 4 0.12 0.12 0.12 0.12 SRR29824955 Y132F Pt16A Pt16 EICU 2023/9/11 Blood 128 0.5 0.12 0.03 4 0.12 0.12 0.12 0.06 SRR29824954 Y132F Pt17A Pt17 ED [CYC] 2023/9/26 Urine >256 8 0.5 0.25 4 >8 2 2 0.12 SRR29824953 Y132F PtPRA† PtPR RD4 2022/3/2 Urine >256 8 0.5 0.25 8 0.5 0.25 0.25 0.25 SRR29824952 Y132F Abbreviation: C. auris=Candida auris; ED=emergency department; RD=respiratory department; ICU=intensive care unit; EICU=emergency ICU; NICU=neurology ICU; RICU=respiratory ICU; SICU=surgical ICU; BALF=bronchoalveolar lavage fluid; CVC=central venous catheter.
* Resistant results for fluconazole, amphotericin B and echinocandin agents interpreted per US CDC tentative breakpoints (https://www.cdc.gov/fungal/candida-auris/c-auris-antifungal.html) were marked in italic bold font.
† Strain PtPRA was isolated from a patient admitted to the hospital one year before the study period. This patient had been described in another report during treatment at a different hospital (Chen XF et al. 2024), and was not included in the 17 cases reported in this study.Table S2. Information on C. auris isolates identified from the CY Hospital.
-
C. auris is an emerging multidrug-resistant fungal pathogen that causes life-threatening diseases and nosocomial outbreaks. The crude mortality of invasive infections caused by C. auris has exceeded 40%, and the pathogen has rapidly spread to approximately 50 countries worldwide since it was first reported in 2008 (7). Notably, the incidence of C. auris cases has increased significantly in China since 2023, with several outbreak events reported (2). However, most C. auris cases reported in Beijing occurred as sporadic events (2,4-5).
In this nosocomial transmission event, 17 C. auris-positive patients admitted to the same hospital in Beijing during a 7-month period in 2023 were identified. More than 76% of the cases were confirmed to be C. auris infections, and all patients had typical Candida infection/colonization risk factors, for example, elderly age or underlying critically ill conditions (8-9). Patient medical records revealed that >76% of C. auris-positive patients received medical management in the EICU ward. As a nosocomial pathogen, C. auris has a predilection for colonizing patient skin and can survive on the surface of medical equipment for more than 1 month (8). Of note, >70% of patients at CY Hospital had at least one positive urine culture for C. auris, with >80% having undergone urinary catheterization. Additionally, on-site investigations in the EICU ward revealed lapses in infection control precautions, such as insufficient disinfection of medical devices and environmental surfaces, which may facilitate the transmission of C. auris within the hospital.
WGS is a powerful tool widely used for geographic epidemiology studies and outbreak investigations of microbial pathogens, including fungi. To date, six C. auris clades have been categorized globally (Clades I–VI) by WGS (7,10). In China, C. auris Clade I isolates were responsible for several outbreaks that occurred in East China (Anhui, Jiangsu) and Hong Kong SAR, China. In contrast, Clade III isolates caused independent outbreak events in northeastern China (Liaoning Province) and southern China (Guangdong Province) (2). As WGS has distinctive discriminatory power, it can provide further insights into the temporal and spatial spread of C. auris. In this report, WGS results revealed that the C. auris strains isolated in CY Hospital belonged to an emerging sublineage of Clade I, which comprised strains previously found in two other hospitals in Beijing since 2021. This Beijing sublineage had >100 bp SNP differences compared with the Clade I outbreak sublineage in East China and the sublineage spread in Hong Kong SAR. These results indicated that city-wide dissemination of a new C. auris sublineage was ongoing in Beijing. Additionally, sporadic cases caused by C. auris Clades II and III strains have also been detected in Beijing (2), suggesting multiple introductions of diverse lineages of C. auris from various sources into the city. As Beijing is a major medical hub receiving patients nationwide for medical services, enhanced surveillance of C. auris in the city’s healthcare facilities is warranted.
Globally, C. auris is highly resistant to fluconazole (>80%) and moderately resistant to amphotericin B (8%–35%) (1). Of note, 100% of the strains identified in CY Hospital, as well as strains of the same sublineage in Beijing, were resistant to fluconazole, and all these strains carried substitutions Y132F on Erg11 and A583S on Tac1b (4–5). In particular, Tac1b A583S represents a unique genomic feature of the Beijing sublineage isolates, distinguishing them from strains of the eastern China and Hong Kong SAR sublineages. Additionally, all but one isolate within the sublineage were amphotericin B resistant. However, the molecular mechanism responsible for amphotericin B resistance in C. auris remains to be investigated. Considering the high possibility of fluconazole and amphotericin B resistance among C. auris strains, treatment with echinocandins is currently the preferred method, and echinocandin resistance is rare (1). However, in this nosocomial transmission event, we further identified echinocandin-resistant isolates from 3 different patients, and a key substitution, S639F, was found on the hotspot region of Fks1 in 2 of these patients (6). Both of these echinocandin-resistant isolates were cultured from urine samples. Their concentration was significantly lower (<1.5%) in urine than in plasma due to the inherent nature of echinocandin-class agents. Consequently, the development of echinocandin resistance in C. auris could have been induced by the subtherapeutic low echinocandin concentrations present in urine during treatment (6).
A global consensus has emerged recognizing the significant challenges C. auris poses to healthcare facilities and public health. This consensus highlights the potential need for more aggressive strategies, including comprehensive surveillance, active case findings, and enhanced infection control measures (1). Currently, infection control strategies for C. auris generally adhere to standard prevention protocols for other multidrug-resistant organisms. These protocols include routine hand hygiene, environmental disinfection, and contact precautions (9). However, the efficacy of these strategies requires further evaluation.
This study has several limitations. First, all environmental samples from the EICU ward were negative for C. auris, which limited investigation of potential transmission pathways. These negative results may be due to the limited sensitivity of traditional culture-based methods; molecular tools will be incorporated in future screening efforts. Additionally, healthcare personnel and personal protective equipment have not yet been screened for C. auris. Overall, infection control investigations in this case require further enhancement.
In conclusion, as stated in this report, an emerging sublineage of multidrug-resistant Clade I C. auris disseminated in Beijing, which was responsible for nosocomial transmission in 17 patients. WGS assays can provide insights into the dynamics of C. auris transmission in addition to resistance mechanisms.
-
The WGS results of C. auris isolates in this study are deposited at the NCBI Sequence Read Archive under BioProject ID: PRJNA906339.
HTML
| Citation: |

|