
 Download:
Download:




-
Preserved ratio impaired spirometry (PRISm) is a non-obstructive spirometry phenotype described as a transient state associated with the progression of chronic obstructive pulmonary disease (COPD) (1). The prevalence of COPD is increasing in China (2). Previous studies excluded PRISm from respiratory studies (3), while recent studies on PRISm have predominantly been conducted in Western or high-income countries (1), leaving the significance of this lung function pattern in China uncertain. To address these gaps, this study analyzed the association between PRISm and all-cause and cause-specific mortality based on the China Kadoorie Biobank (CKB), a large-scale prospective cohort. Elevated risks of mortality from all-cause, cardiovascular, neoplastic, respiratory, and infectious and parasitic diseases were observed in PRISm, with rates comparable to those observed in obstructive spirometry. PRISm should be given more attention to avoid its progression to COPD.
The CKB, which has been reported previously (4), recruited 512,724 participants aged 30 to 79 from 10 areas across China at baseline from 2004 to 2008. All individuals underwent interviewer-administered questionnaires, physical measurements, and spirometry tests by trained technicians according to standard operating procedures. In the present study, participants with previously self-reported physician-diagnosed ischemic heart disease, stroke, cancer, or asthma at baseline, lost to follow-up shortly after baseline, with an FEV1/FVC ratio >1.0, or missing data for covariates were omitted from the study, leaving 484,301 participants.
For baseline spirometry, the higher of two measurements for both FEV1 and FVC was used to calculate the FEV1/FVC ratio. Predicted FEV1 was calculated using the Global Lung Function Initiative 2012 equations for the Southeast Asian and Northeast Asian populations (5). Normal lung function was defined as an FEV1/FVC ratio ≥0.7 and FEV1 ≥80% predicted, PRISm as an FEV1/FVC ratio ≥0.7 and FEV1 <80% predicted, and obstructive spirometry as an FEV1/FVC ratio <0.7.
Mortality data were obtained from official residential records and the Disease Surveillance Points system, supplemented by annual door-to-door investigations among those not linked to the database. Based on the International Classification of Disease, 10th Revision (ICD-10), the outcomes comprised death from all causes and cause-specific mortality, including circulatory diseases (ICD-10: I00–I99), neoplasms (C00–D48), respiratory diseases (J00–J99), infectious and parasitic diseases (A00–B99), ischemic heart disease (I20–I25), intracerebral hemorrhage (I61), ischemic stroke (I63), lung cancer (C34), COPD (J41–J44), pneumonia (J12–J18), and respiratory tuberculosis (A15–A16). Participants were censored upon death, loss to follow-up, or December 31, 2022, whichever occurred first.
Baseline variable means and prevalences were calculated for normal, PRISm, and obstructive spirometry groups using linear regression for continuous variables and logistic regression for categorical variables, adjusted for age, sex, and 10 study areas when appropriate. Mortality rates per 100,000 person-years for each group were standardized to the age structure of the 7th National Population Census data (2020). For all-cause mortality, stratified Cox proportional hazards regression was used to estimate hazard ratios (HRs) with 95% confidence intervals (CIs). A proportional subdistribution hazards regression model for cause-specific mortality was fitted to account for competing risks from other causes. All analyses were stratified by age (in 5-year groups), sex, and 10 study areas, and adjusted for education, occupation, household income, marital status, alcohol consumption, smoking status, passive smoking status, physical activity levels, primary cooking and heating fuel use, consumption frequency of fresh fruits, fresh vegetables, and meat, general obesity, and abdominal obesity. The proportional hazards assumption was verified using Schoenfeld residuals. Associations between mortality and PRISm were analyzed after stratification by the presence of self-reported cough or sputum, ever-smoking, physician-diagnosed bronchitis or emphysema, and tuberculosis at baseline. Subgroup analyses were conducted across sex, age (≥60 years or not), and region (urban/rural).
Competing-risk analysis was performed using SAS (version 9.4, SAS Institute Inc, Cary, NC, USA), and all other statistical analyses were performed using R (version 4.3.1, R Foundation for Statistical Computing, Vienna, Austria). All tests were two-tailed, and P<0.05 were considered statistically significant.
The study included 484,301 participants with a mean age of 51.5 [standard deviation (SD)=10.5] years at baseline, 59.1% women, and 32.3% ever-smokers. At baseline, 117,210 (24.2%) had PRISm, with a mean FEV1 % predicted of 83.9%. Compared with the normal group, individuals with PRISm or an obstructive spirometry pattern were more likely to be older, male, current or former smokers, reside in rural areas, have a lower socioeconomic level, and report poorer self-rated health status (Table 1).
Characteristics Normal PRISm Obstructive spirometry No. of participants 341,975 (70.6) 117,210 (24.2) 25,116 (5.2) FEV1/FVC [%, mean (SD)] 86.3 (5.8) 83.9 (5.9) 64.4 (5.8) FEV1 % predicted [%, mean (SD)] 96.1 (11.1) 69.8 (11.3) 62.0 (11.2) Sociodemographic characteristics Age, years [mean (SD)] 50.5 (10.4) 53.0 (10.6) 58.8 (10.4) Women 59.5 59.9 50.8 Urban 44.9 40.5 29.0 South 64.8 46.4 72.8 Education >6 years 50.4 46.1 45.1 Farmer or worker 57.5 57.9 58.7 Household income ≥20,000 yuan/year 43.9 40.3 35.7 Married 91.3 90.4 89.1 Lifestyle factors Ever smoking 31.8 32.8 36.3 Ever passive smoking 75.5 75.7 73.8 Currently drinking 15.3 14.7 14.2 Daily intake of fresh fruit 18.6 17.1 16.8 Daily intake of fresh vegetables 94.9 94.3 94.4 >4 days/week intake meat 47.6 46.8 43.9 Physical activity, MET-h/d [mean (SD)] 21.7 (12.2) 21.2 (12.5) 21.3 (12.3) BMI, kg/m2 [mean (SD)] 23.6 (3.3) 23.8 (3.4) 22.5 (3.3) Abdominal obesity 22.2 28.3 15.8 Personal medical history Self-rated poor health 8.3 10.5 13.9 Hypertension 32.7 37.5 30.5 Diabetes 5.2 6.1 4.4 Emphysema or bronchitis 1.4 3.4 8.9 Frequent coughing 6.9 9.6 15.0 Frequent expectoration 6.2 8.5 13.0 Note: Values are reported as % unless otherwise indicated and adjusted for age, sex, and study areas when appropriate. All P values for comparisons between groups were < 0.001, except for ever passive smoking (P=0.009). Lung function category definitions: normal (FEV1/FVC ratio ≥0.7 and FEV1 ≥80%), PRISm (FEV1/FVC ratio ≥0.7 and FEV1 <80%), and obstructive spirometry (FEV1/FVC ratio <0.7).
Abbreviation: PRISm=preserved ratio impaired spirometry; FEV1=forced expiratory volume in one second; FVC=forced vital capacity; SD=standard deviation; MET-h/d=metabolic equivalents of task per hour per day; BMI=body mass index; CVD=cardiovascular disease.Table 1. Characteristics of China Kadoorie Biobank participants by obstruction state at baseline of 2004–2008.
During a median follow-up of 16.0 years, 73,288 deaths were documented, and the corresponding all-cause age-standardized mortality rates for normal, PRISm, and obstructive spirometry were 1,070.5, 1,574.4, and 1,943.3 per 100,000 person-years, respectively. Compared with the normal group, PRISm had a higher adjusted all-cause (HR=1.37, 95% CI: 1.35, 1.40), circulatory disease [subdistribution hazard ratio (SHR)=1.36, 95% CI: 1.33, 1.40], neoplasm (SHR=1.07, 95% CI: 1.04, 1.11), and infectious and parasitic disease (SHR=1.47, 95% CI: 1.24, 1.73) mortality, comparable to those observed in obstructive spirometry (Table 2). For respiratory disease mortality, the SHR in PRISm was 2.45 (95% CI: 2.30, 2.60), lower than those with obstructive spirometry (SHR=5.05, 95% CI: 4.73, 5.39). For disease-specific deaths, PRISm was associated with a higher risk of death from ischemic heart disease (SHR=1.37, 95% CI: 1.31, 1.42), intracerebral hemorrhage (SHR=1.31, 95% CI: 1.25, 1.38), ischemic stroke (SHR=1.30, 95% CI: 1.20, 1.40), lung cancer (SHR=1.26, 95% CI: 1.19, 1.34), COPD (SHR=3.06, 95% CI: 2.84, 3.31), pneumonia (SHR=1.47, 95% CI: 1.28, 1.68), and respiratory tuberculosis (SHR=2.63, 95% CI: 1.82, 3.82).
Cause of death Normal PRISm Obstructive spirometry All causes No. of deaths (mortality rate) 40,099 (1,070.5) 23,791 (1,574.4) 9,398 (1,943.3) HR (95% CI) 1.00 1.37 (1.35, 1.40) 1.59 (1.56, 1.63) Circulatory diseases No. of deaths (mortality rate) 16,091 (473.7) 10,916 (738.0) 3,340 (676.2) SHR (95% CI) 1.00 1.36 (1.33, 1.40) 1.22 (1.18, 1.27) Ischemic heart disease No. of deaths (mortality rate) 6,008 (181.1 4,254 (293.2) 1,157 (250.0) SHR (95% CI) 1.00 1.37 (1.31, 1.42) 1.22 (1.14, 1.30) Intracerebral haemorrhage No. of deaths (mortality rate) 3,726 (96.7) 2,938 (186.6) 881 (169.7) SHR (95% CI) 1.00 1.31 (1.25, 1.38) 1.29 (1.19, 1.39) Ischemic stroke No. of deaths (mortality rate) 1,808 (61.0) 1,198 (84.5) 329 (64.8) SHR (95% CI) 1.00 1.30 (1.20, 1.40) 1.02 (0.90, 1.15) Neoplasms No. of deaths (mortality rate) 13,982 (316.1) 6,188 (374.5) 2,231 (461.3) SHR (95% CI) 1.00 1.07 (1.04, 1.11) 1.09 (1.04, 1.14) Lung cancer No. of deaths (mortality rate) 3,416 (77.4) 1,843 (111.8) 692 (134.8) SHR (95% CI) 1.00 1.26 (1.19, 1.34) 1.35 (1.24, 1.48) Respiratory diseases No. of deaths (mortality rate) 2,013 (69.6) 2,607 (188.5) 2,389 (481.3) SHR (95% CI) 1.00 2.45 (2.30, 2.60) 5.05 (4.73, 5.39) COPD No. of deaths (mortality rate) 1,148 (39.6) 2,009 (146.1) 2,130 (426.8) SHR (95% CI) 1.00 3.06 (2.84, 3.31) 6.81 (6.29, 7.38) Pneumonia No. of deaths (mortality rate) 582 (21.2) 380 (27.6) 125 (26.7) SHR (95% CI) 1.00 1.47 (1.28, 1.68) 1.32 (1.08, 1.63) Infectious and parasitic diseases No. of deaths (mortality rate) 445 (10.8) 275 (16.8) 101 (22.3) SHR (95% CI) 1.00 1.47 (1.24, 1.73) 1.68 (1.33, 2.11) Respiratory tuberculosis No. of deaths (mortality rate) 59 (1.5) 69 (4.9) 48 (10.2) SHR (95% CI) 1.00 2.63 (1.82, 3.82) 4.08 (2.69, 6.19) Other diseases No. of deaths (mortality rate) 7,568 (200.3) 3,805 (256.6) 1,337 (302.2) SHR (95% CI) 1.00 1.23 (1.18, 1.28) 1.15 (1.08, 1.22) Note: The mortality rate is per 100,000 person-years and is age-standardized based on the 7th National Population Census data (2020). For cause-specific mortality, other causes of mortality were considered as competing risks, and SHRs were calculated. HRs and SHRs were stratified by age (in 5-year intervals), sex, and study areas, and adjusted for education, occupation, household income, marital status, alcohol consumption, smoking status, passive smoking status, physical activity levels, cooking and heating fuel usage, consumption frequency of fresh fruits, fresh vegetables, meat, and general and abdominal obesity. Lung function category definitions: normal (FEV1/FVC ratio ≥ 0.7 and FEV1 ≥80%), PRISm (FEV1/FVC ratio ≥0.7 and FEV1 <80%), and obstructive spirometry (FEV1/FVC ratio <0.7).
Abbreviation: PRISm=preserved ratio impaired spirometry; COPD=chronic obstructive pulmonary disease; HR=hazard ratio; SHR=subdistribution hazard ratio; CI=confidence interval; FEV1=forced expiratory volume in one second; FVC=forced vital capacity.Table 2. Associations of PRISm and Obstructive Spirometry with all-cause and cause-specific mortality in China Kadoorie Biobank, 2004–2022.
When stratified by respiratory symptoms of PRISm individuals, those with frequent coughing or sputum (HR=1.62, 95% CI: 1.57, 1.68) and self-reported prior bronchitis or emphysema (HR=1.81, 95% CI: 1.72, 1.91) had a much higher risk of all-cause mortality. However, the risk of all-cause mortality in the PRISm group did not appear to be substantially affected by smoking or passive smoking status (Figure 1). Analyses of sex, age, and regional subgroups of PRISm mortality risk did not show large differences (
Supplementary Table S1 ).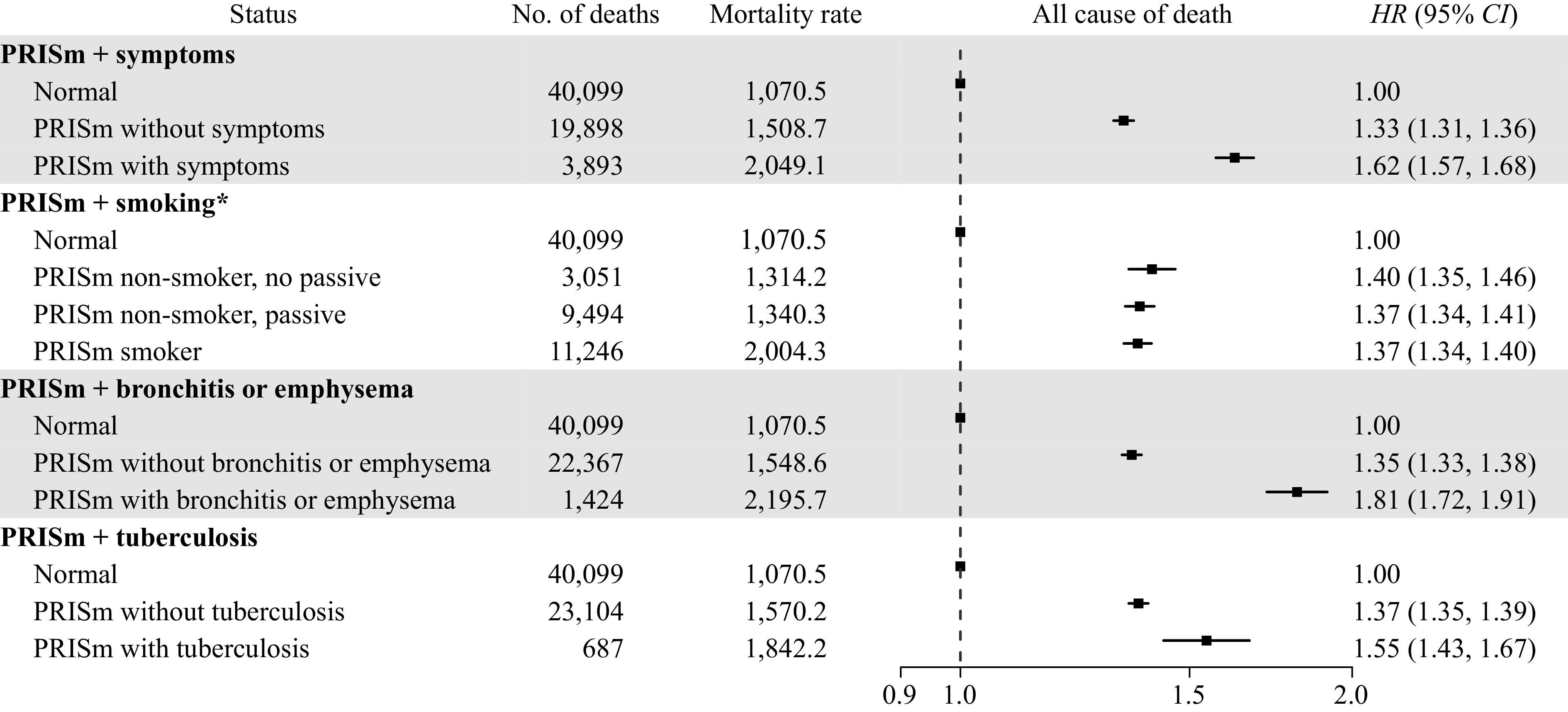 Figure 1.
Figure 1.Associations of PRISm with symptoms, smoking, bronchitis or emphysema, tuberculosis at baseline with all-cause mortality in China Kadoorie Biobank, 2004–2022.
Note: The mortality rate is per 100,000 person-years and is age-standardized based on the 7th National Population Census data (2020). HRs were stratified by age (in 5-year intervals), sex, and study areas, and adjusted for education, occupation, household income, marital status, alcohol consumption, smoking status, passive smoking status, physical activity levels, cooking and heating fuel usage, consumption frequency of fresh fruits, fresh vegetables, meat, and general and abdominal obesity. Symptoms were defined as frequent coughing or sputum. PRISm was defined as FEV1/FVC ratio ≥0.7 and FEV1 <80%.
Abbreviation: PRISm=preserved ratio impaired spirometry; HR=hazard ratio; CI=confidence interval.
*PRISm individuals were grouped according to whether they never/occasionally smoked or smoked regularly, and whether they were passively exposed to smoke.
-
Based on a large prospective cohort, this study explored the health effects of PRISm in the Chinese population, examining a comprehensive spectrum of mortality risks. The PRISm group exhibited a 1.4-fold higher risk of all-cause mortality. Risks of cause-specific death were also increased in the PRISm group; however, respiratory disease mortality in the PRISm group was lower than in the obstructive spirometry group, suggesting the reversibility of airflow obstruction development in PRISm. Moreover, respiratory-related symptoms and diseases were associated with an increased mortality risk, which could help identify high-risk individuals in the PRISm population.
A systematic review, including eight population-based cohort studies up to 2023, found that PRISm was associated with a 1.7-fold, 1.6-fold, and 2.0-fold increased risk of all-cause, cardiovascular, and respiratory mortality, respectively (1). These results were slightly higher than our findings; however, the review neglected the competing risks from other causes of death, leading to overestimation of the HRs. Evidence for disease-specific mortality risk is scarce due to the need for long-term follow-up and large sample sizes. Only one study reported that PRISm was associated with a 1.5-fold increased risk of death from stroke or heart disease (6). This study is the first to show that PRISm is associated with an increased risk of death from lung cancer, pneumonia, COPD, and respiratory tuberculosis. However, no modification effect was observed between smoking or passive smoking and the association between PRISm and mortality. Nonetheless, previous studies have shown smoking to be a strong risk factor for PRISm and its progression to airflow obstruction (7,8), suggesting that smoking cessation should be prioritized when managing PRISm to prevent premature death.
This study has several limitations. First, like other population-based epidemiologic studies (7,9), spirometry without postbronchodilator testing may overestimate the prevalence of both PRISm and obstructive spirometry. Participants with self-reported asthma at baseline were excluded to minimize such misclassification bias. Despite the potential misclassification, this study indicated that pre-bronchodilator testing is crucial and can provide significant insights, especially in resource-limited settings. Second, PRISm was employed as a single-time measurement of exposure. Given the high variability in spirometry-measured lung function observed within individuals over time (7,10), this study could not examine the relationship between longitudinal PRISm trajectories and mortality risk. Third, the generalization of results to other populations should be made with caution, as the CKB cohort sample is not nationally representative.
This study identified an elevated risk of all-cause and cause-specific mortality from PRISm in China, including circulatory, neoplasm, respiratory, and infectious and parasitic disease mortality. This finding indicates the necessity of enhancing public awareness of PRISm and taking action to prevent its progression to COPD.
HTML
| Citation: |

|