
 Download:
Download:




-
Coronavirus disease 2019 (COVID-19), a contagious illness caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has imposed an unprecedented burden on public health systems worldwide. As of mid-July 2023, there have been over 768 million confirmed cases of SARS-CoV-2 infection, resulting in more than 6.9 million deaths globally (1). The rapid increase in new cases continues to be fueled by various genomic variants of the virus. Notably, the recent emergence of the BA.1 through BA.5 and XBB (Omicron) variants, classified as the sixth variant of concern, demonstrates increased transmissibility and resistance to immunity (2).
SARS-CoV-2 transmits among humans via respiratory droplets and aerosols during actions such as sneezing, talking, or coughing (3). The rapid and widespread dissemination of SARS-CoV-2 across geographical and species boundaries highlights the critical need for adopting the One Health approach to effectively tackle public health emergencies. Central to managing the COVID-19 pandemic is the development and implementation of swift and accessible diagnostic tools. Currently, real-time reverse transcription-polymerase chain reaction (RT-PCR) is considered the benchmark for COVID-19 diagnosis; however, challenges persist in its practical use. Notably, during the collection of nasopharyngeal secretions, the recommended one-meter distance between the healthcare provider and the patient is often not maintained, potentially heightening the risk of COVID-19 transmission. Furthermore, RT-PCR can take several hours to yield results and may result in false negatives (4). Consequently, developing a rapid detection method is imperative for timely isolation of suspected SARS-CoV-2 cases and minimizing the transmission risk.
The SARS-CoV-2 antigen rapid diagnostic test (Ag-RDT) has been crucial in the early detection of cases, containment strategies, and reducing transmission (5–7). Multiple studies have assessed Ag-RDTs’ diagnostic accuracy across different populations and clinical environments, revealing varied results (8–10). Ag-RDTs demonstrate high sensitivity during the initial week following symptom onset and exhibit excellent specificity when viral loads are elevated (5). Currently, Ag-RDTs are accessible to the general public, delivering results within 15−30 minutes. Consequently, they serve as a supplementary method to RT-PCR for the quick, economical, and straightforward identification of SARS-CoV-2 infections. Furthermore, Ag-RDTs are effective as point-of-care tests (POCT) for diagnosis in the disease's early stages, providing a significant advantage in curbing SARS-CoV-2 spread.
In the conceptual design phase, our ALLtest distinguishes itself from other Ag-RDTs through its innovative utilization of IgM antibodies targeting the nucleocapsid (N) protein. The N protein is integral to various stages of the replication cycle and serves as a serological marker for SARS-CoV-2 infection (11). This technique enhances early-stage infection detection and provides deeper insights into transmission dynamics. By incorporating this novel element into antigen diagnosis, the ALLtest enables a more comprehensive evaluation of SARS-CoV-2 infection, thereby facilitating improved public health interventions and mitigation strategies. In this study, nasopharyngeal swabs (NPS) were collected from suspected COVID-19 cases and subjected to diagnostic RT-PCR in the United States (US), Sweden (SE), and Poland (PL) from July 2021 to January 2022. All samples were subsequently analyzed using the ALLtest to conduct a detailed correlation analysis among various diagnostic assays. Furthermore, we explore the challenges and limitations of IgM-based antigen diagnosis, underscoring the necessity for versatile diagnostic approaches to effectively address the global health crisis. By elucidating the details of this innovative methodology, we not only enhance our comprehension of COVID-projected diagnostics but also contribute to establishing a more robust and proactive global health response.
-
The nucleocapsid protein (NCBI: NC_045512.2) was expressed under identical conditions as described in our previous study (12). BALB/c mice, ranging in age from 4 to 8 weeks, were intraperitoneally injected with 50 µg of N antigen per mouse for the initial immunization, followed by 100 µg per mouse for the second and third immunizations at biweekly intervals. Spleen cells from mice with high antibody titers were fused with myeloma cells to produce hybridoma cells. These cells were then injected into BALB/c mice to generate mAbs specific for the SARS-CoV-2 N protein. The titers of these mAbs were evaluated using indirect ELISA on plates coated with 5 µg/well of N antigen. We tested 12 distinct mAbs, initially diluted from 1∶10 to 1∶108 starting from a concentration of 1 mg/mL. Pair screening of the mAbs was conducted using the ForteBio Octet® Red96 system, where the response value (nm) indicative of specific binding to the SARS-CoV-2 N antigen was recorded for each mAb pair. High-titer mAbs demonstrating effective pairing were further characterized for their isotypes using the multiple antibody isotypes kit from Proteintech Group Inc., China (Cat No. PK20003), which includes IgG1, IgG2a, IgG2b, IgG3, IgA, IgM, kappa light chain, and lambda light chain.
-
The SARS-CoV-2 Ag-RDT was developed using the immunochromatographic method to detect the SARS-CoV-2 N antigen in NPS samples. The structural design of the Ag-RDT cassette is principally similar to that used in the ALLtest for antibody detection (13). The process begins by placing the sample and buffer on the sample pad. The fluid then migrates from left to right, sequentially interacting with the conjugation pad that contains labeled colloidal gold-mAb17, the NC membrane where specific antibodies are immobilized at distinct lines [test (T) line with mAb16 at 1 mg/mL, and control (C) line with goat anti-mouse IgG at 1 mg/mL], and finally the absorption pad.
-
To assess the sensitivity of the ALLtest Ag-RDT Assay, preparations were made using 1.0×106 median tissue culture infectious doses (TCID50)/mL of the SARS-CoV-2 Shenzhen/02/2020 strain and 1 mg/mL of full-length nucleocapsid protein (NCBI: NC_045512.2). For specificity validation of the same assay, samples from four human coronaviruses (HCoV-229E, HCoV-HKU1, CoV-OC43, HCoV-NL63), parainfluenza viruses 2 and 3, influenza A and B, adenovirus types 3 and 7, human rhinovirus 2, 14, and 16, measles virus, mumps virus, and respiratory syncytial virus were prepared. Furthermore, to evaluate potential interference, substances, including budesonide nasal spray, mucin, dexamethasone, flunisolide, mupirocin, oxymetazoline, phenylephrine, rebetol, relenza, tamiflu, tobramycin, and whole blood, were spiked with negative and weak positive SARS-CoV-2 samples. Swabs spiked with virus tissue cultures, nucleocapsid protein, various virus strains, and interfering substances at specified concentrations were tested under defined reaction conditions.
-
To assess the sensitivity of the ALLtest Ag-RDT Assay across various SARS-CoV-2 variants, including Alpha, Beta, VUI-21ARP-03, Gamma, Delta, and Omicron, these strains were prepared in dilutions using 0.5% BSA-PBS to create different concentration solutions. A volume of 30 µL from each solution was applied to the tip of a nasal swab, subsequently immersed in extraction buffer. Three to four drops of this mixture were then placed into the sample well of the test cassette. Results were visually read from the cassette after 15 minutes, according to the protocol specified by the manufacturer.
-
Antigen tests were conducted on 1,030 individuals suspected of having COVID-19 across three international centers: Phamatech, Inc. in America (PI-US), iLab in Sweden (I-SE), and Uniwersyteckie Centrum Kliniczne in Poland (UCK-PL) from July 2021 to January 2022. Participant data from these centers is compiled in Table 1. Each participant provided two NPS specimens. One swab was analyzed immediately using the ALLtest Ag-RDT Assay or processed using sample lysates without protein denaturant and stored at either 4 ℃ for up to 24 hours or below –70 ℃ for extended storage. The second swab was preserved in universal transport medium and tested for ORF1a/b through quantitative reverse transcription PCR (qRT-PCR) within 24 hours. The Ct values from the qRT-PCR were documented for subsequent analysis. This research received ethical approval from the Ethical Committee of Phamatech, Inc. in America (Approval No. 21-HANG-101) and Uniwersyteckie Centrum Kliniczne in Poland (Approval No. NKBBN/710/2021). The requirement for informed consent was waived for the clinical trial conducted by iLab in Sweden.
Parameter PI-US I-SE UCK-PL RT-PCR positive
(n=44)RT-PCR negative
(n=247)RT-PCR positive
(n=100)RT-PCR negative
(n=114)RT-PCR positive
(n=223)RT-PCR negative
(n=302)Age in years, mean (SD) 34.6 (18.9) 33.3 (17.5) − − 47.8 (21.7) 46.2 (24.5) Gender (%) Male 20.0 (45.5) 99.0 (40.1) − − 115.0 (51.6) 144.0 (47.8) Female 24.0 (54.5) 148.0 (59.9) − − 108.0 (48.4) 158.0 (52.3) Cycle threshold (%) <15 0 (0) 1.0 (1.0) 0 (0) 15 to <20 5.0 (11.4) 6.0 (6.0) 178.0 (79.8) 20 to <25 12.0 (27.3) 8.0 (8.0) 15.0 (6.7) 25 to <30 20.0 (45.5) 29.0 (29.0) 10.0 (4.5) 30 to <35 7.0 (15.9) 56.0 (56.0) 20.0 (9.0) ≥35 0 (0) 0 (0) 0 (0) Note: “−” means information not recorded.
Abbreviation: PI-US=Phamatech, Inc. in USA; I-SE=iLab in Sweden; UCK-PL=Uniwersyteckie Centrum Kliniczne in Poland; RT-PCR=real-time reverse transcription-polymerase chain reaction; SD=standard deviation.Table 1. Summary of participant information from three centers.
-
The sensitivity and specificity served as the primary metrics for assessing our antigen test. Sensitivity, or the true positive rate, was determined by dividing the number of positive cases identified by the ALLtest by the number of true positive cases confirmed by the RNA test. Specificity, or the true negative rate, was calculated by dividing the number of negative cases identified by the ALLtest by the total number of true negative cases. The 95% confidence intervals (CIs) were derived using exact binomial tests.
To determine factors strongly correlated with antigen test outcomes, participants were divided into two categories according to their test results. Factors in each category were then compared for significance. For categorical variables such as sex and Ct category, Pearson’s chi-square test was utilized. For continuous variables including age, symptom duration, and Ct value — depending on their distribution — either the T-test or the Wilcoxon test was employed. All statistical analyses were performed using R software (version 3.6.0, R Core Team, Vienna, Austria).
-
The PCR amplification of the SARS-CoV-2 N gene resulted in a 1,200 bp band, as observed through 1% agarose gel electrophoresis (Figure 1A). Following immunization and cell fusion, 12 mAbs were produced against the SARS-CoV-2 N protein (Figure 1B). The titers for five of these mAbs were notably high, approximately 1∶102,400, whereas the titers for the remaining mAbs were around 1∶25,600 (Figure 1C). Subsequent to pair-wise screening (Figure 1D), mAbs N1, N12, N15, N16, and N17 were chosen for further analysis to identify antibody subtypes and develop the Ag-RDT Assay, due to their effective pairing performance and elevated titers. Notably, N16 and N17 were classified as IgM, while the other mAbs were identified as IgG1 subtype (Figure 1E).
 Figure 1.
Figure 1.Characterization and paired screening of mAbs against the N protein. (A) Electrophoresis analysis of PCR products from pET-28a (+)-N. M: marker, L1: SARS-CoV-2 N gene; (B) SDS-PAGE analysis of SARS-CoV-2 N mAbs. M: marker, L1–L17: purified mAbs of SARS-CoV-2 N; (C) Titer detection of mAbs; (D) Heat map presenting paired results of mAbs; (E) Histogram of ELISA identification of mAbs subtypes N1, N12, N15, N16, and N17; (F) Identification of SARS-CoV-2 N mAbs subtypes using a monoclonal antibody subtyping kit.
Abbreviation: PCR=polymerase chain reaction; SARS-CoV-2=severe acute respiratory syndrome coronavirus 2; SDS-PAGE=sodium dodecyl sulfate polyacrylamide gel electrophoresis; ELISA=enzyme linked immunosorbent assay. -
The Ag-RDT assay was constructed using paired mAbs based on the standard schematic for colloidal gold test strip assembly, as illustrated in Figure 2A. One mAb was conjugated with colloidal gold while its counterpart served as the capture line (T-line) antibody. Sensitivity varied across different antibody pairs when assessing both positive and negative samples. The assay achieved maximal detection sensitivity and specificity when colloidal gold was conjugated with N17 and the T-line utilized N16, as shown in Figure 2B. Testing with the optimized Ag-RDT assay on virus tissue culture and recombinant SARS-CoV-2 N protein antigen at varying dilutions identified the lowest detection limits: 100 TCID50/mL for heat-inactivated SARS-CoV-2 virus (Figure 2C) and 0.1 ng/mL for the recombinant N antigen.
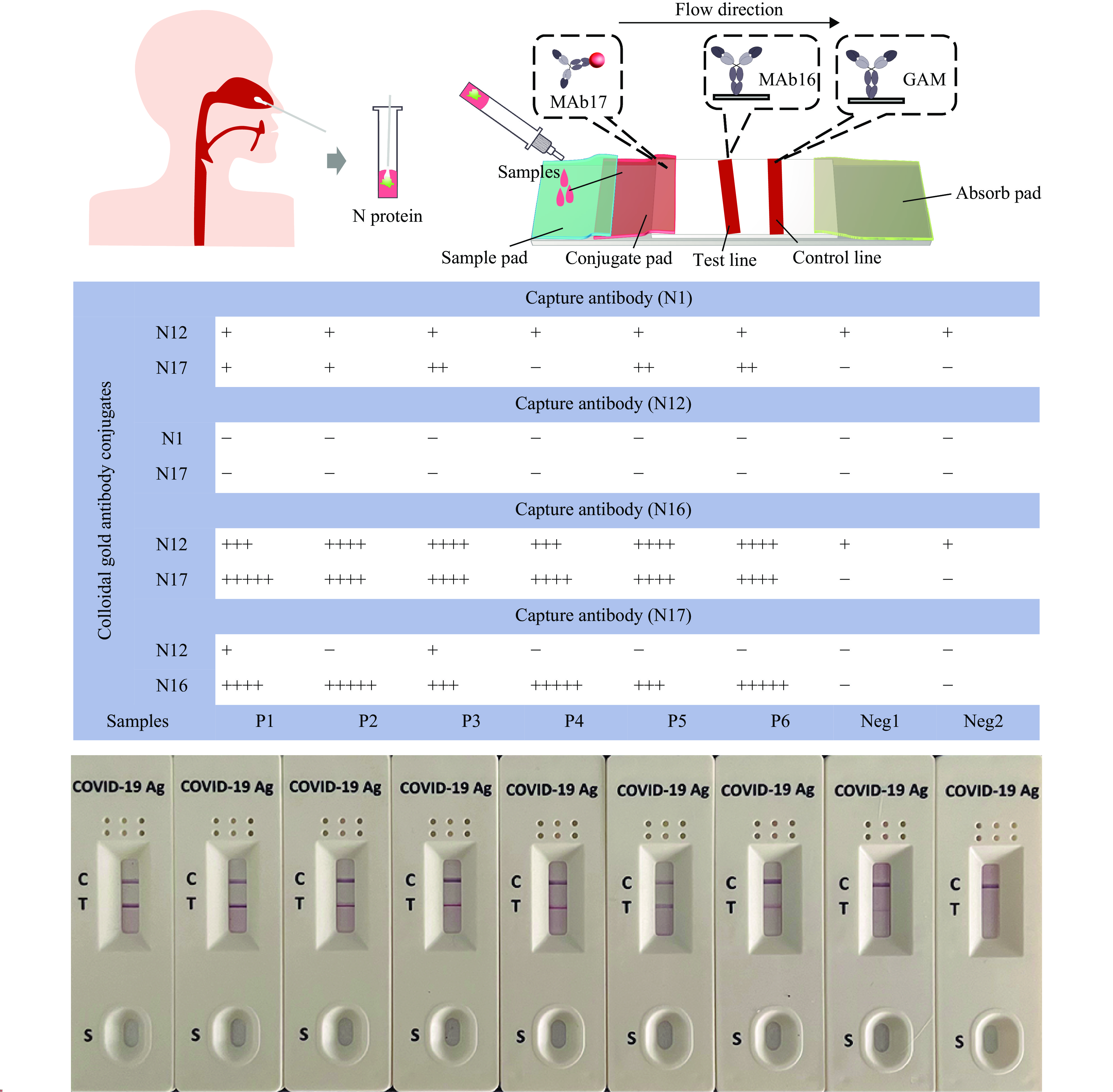 Figure 2.
Figure 2.Sensitivity detection of the Ag-RDT assay for COVID-19. (A) The principal diagram of the colloidal gold test strip assembly and sample detection process; (B) Detection sensitivity and specificity using colloidal gold labeling and T-line labeling with various paired monoclonal antibodies (mAbs); (C) Sensitivity detection of the Ag-RDT assay for the heat-inactivated SARS-CoV-2 virus.
Note: In panel C, Lines 1–9 indicate concentrations ranging from 109 to 10 TCID50/mL; Line 8 indicates that the minimal limit of detection is 100 TCID50/mL.
Abbreviation: Ag-RDT=antigen early rapid diagnostic test; COVID-19=coronavirus disease 2019; SARS-CoV-2=severe acute respiratory syndrome coronavirus 2; TCID=tissue culture infectious doses.
To verify the specificity of the Ag-RDT assay, we tested it against four other human coronaviruses and 13 viruses that cause respiratory illnesses. The results, which showed no cross-reactions (
Supplementary Table S1 ), confirmed the assay’s specificity for detecting the SARS-CoV-2 antigen. Additionally, various substances including budesonide nasal spray, mucin, dexamethasone, flunisolide, mupirocin, oxymetazoline, phenylephrine, rebetol, relenza, tamiflu, tobramycin, and whole blood were demonstrated not to interfere with the Ag-RDT results at the concentrations used (Supplementary Table S2 ). -
To assess the detection limit of the Ag-RDT assay for various SARS-CoV-2 variants, including Alpha, Beta, Gamma, Delta, and Omicron, each variant was subjected to testing. Results presented in
Supplementary Table S3 demonstrate that the Ag-RDT assay can effectively detect SARS-CoV-2 variants such as B.1.1.7, B.1.351, B.1.617.3, P.1.2, B.1.617.2, B.1.1.529, BA.2, BA.4, and BA.5, down to specific dilution rates and concentrations. -
The ALLtest antigen test was assessed across three centers, as detailed in Table 2. Within the PI-US cohort of 291 participants, the ALLtest correctly identified 41 out of 44 confirmed cases and showed no false positives among excluded cases, achieving a sensitivity of 93.18% and a specificity of 100%. Similarly, the test demonstrated high clinical efficacy in the I-SE and UCK-PL cohorts, with sensitivities of 100% and 97.31%, and specificities of 100% and 99.67%, respectively. Notably in the PI-US center, the sensitivity increased to 97.30% (95% CI: 85.84%, 99.93%) for samples with Ct values below 30, and to 96.77% (95% CI: 83.30%, 99.92%) for patients displaying symptoms within the first week. Additionally, the UCK-PL center reported a higher sensitivity of 99.51% (95% CI: 97.29%, 99.99%) for samples with Ct values below 30.
Antigen test results PI-US I-SE UCK-PL + − Total + − Total + − Total Positive 41 0 41 100 0 100 217 1 218 Negative 3 247 250 0 114 114 6 301 307 Total 44 247 291 100 114 214 223 302 525 Test evaluation, % (95% CI) Sensitivity 93.2 (81.3, 98.6) 100.0 (96.4, 100.0) 97.3 (94.2, 99.0) Specificity 100.0 (98.5, 100.0) 100.0 (96.8, 100.0) 99.7 (98.2, 100.0) Note: “−” means negative. “+” means positive.
Abbreviation: PI-US=Phamatech, Inc. in USA; I-SE=iLab in Sweden; UCK-PL=Uniwersyteckie Centrum Kliniczne in Poland; RT-PCR=real-time reverse transcription-polymerase chain reaction; CI=confidence interval.Table 2. Sensitivity and specificity of ALLtest.
-
Clinical factors including age, sex, duration of symptoms, and Ct values of participants were assessed for correlations with results from the ALLtest antigen assay, as shown in
Supplementary Table S4 . Across three centers, results were consistent. A significant number of participants exhibited low viral loads that precluded RNA detection by PCR, regardless of the number of amplification cycles performed. Therefore, artificial cutoff values were employed to categorize Ct values. In PI-US and UCK-PL settings, both actual Ct values (Figure 3A and 3B; P=0.026, P=9.74×10−5) and categorized Ct values (Ct<35 versus Ct≥35; P<2.2×10−16) demonstrated a significant correlation with antigen test outcomes. The timing of symptom onset correlated with antigen results exclusively in UCK-PL (P=0.0018; Figure 3C). No significant correlations between age or sex and antigen test results were identified.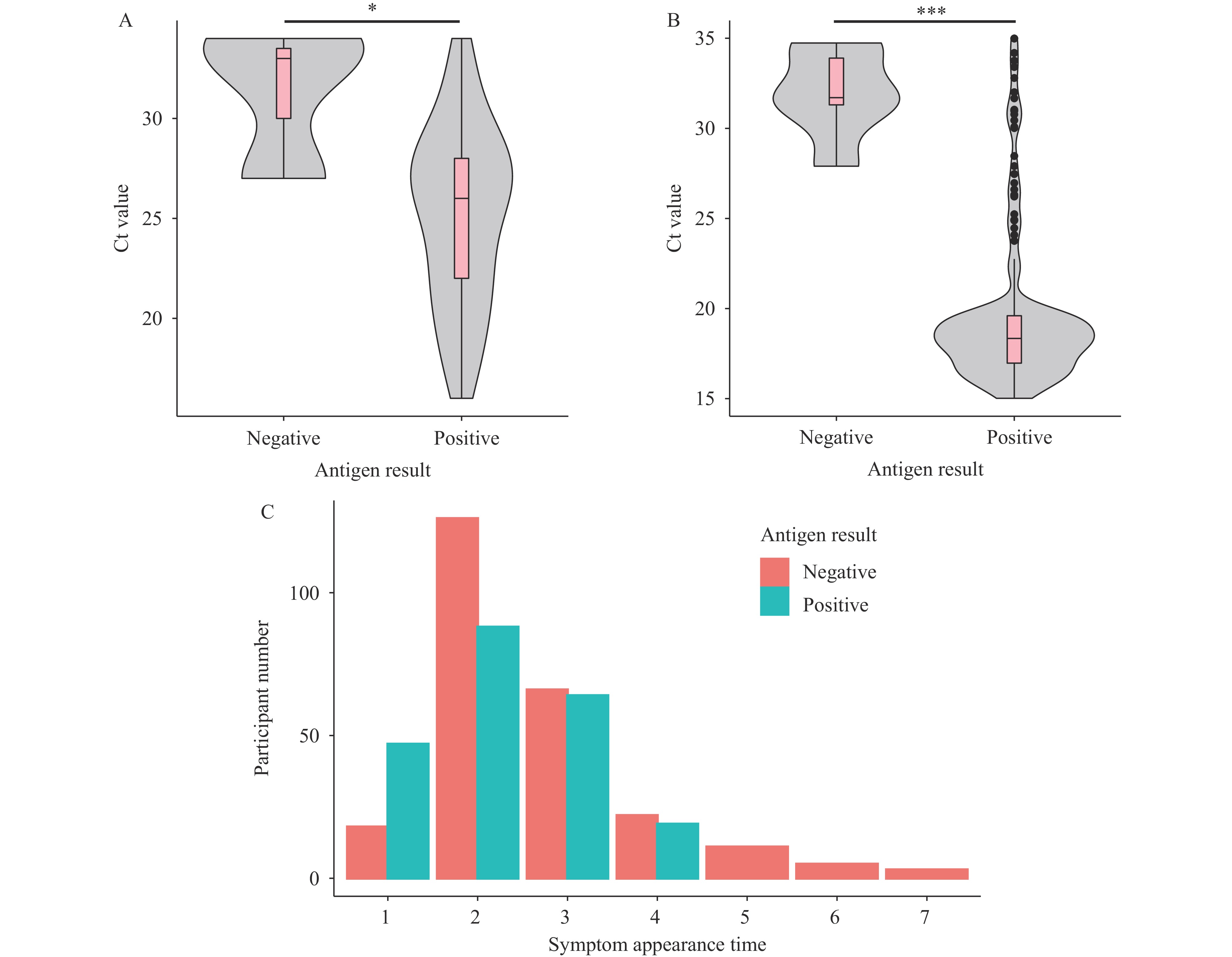 Figure 3.
Figure 3.Correlation factors associated with ALLtest results. (A) Ct value distributions among participants from PI-US categorized by differing antigen test results (P=0.026); (B) Ct value distributions among participants from UCK-PL categorized by differing antigen test results (P=9.74×10−5); (C) Distributions of symptom onset among participants from UCK-PL with varying antigen test outcomes (P=0.0018).
Abbreviation: Ct=cycle threshold; UCK-PL=Uniwersyteckie Centrum Kliniczne in Poland; PI-US=Phamatech, Inc. in USA. -
The SARS-CoV-2 pandemic continues to pose significant challenges, necessitating effective strategies to curb its spread. Antigen testing has been crucial in early detection, containment, and the reduction of transmission rates. Furthermore, its integration with the One Health approach emphasizes the interconnection of human, animal, and environmental health, highlighting the need for a robust and unified global health framework. Recent literature indicates varying findings regarding the application of antigen tests in diagnosing COVID-19. A meta-analysis of antigen tests developed before September 30, 2020, showed that under specific conditions, despite varied sensitivity, rapid antigen tests could serve as alternatives to RT-PCR (13). Conversely, Greub et al. reported mixed performances among 30 antigen tests, advocating for comprehensive validation before official adoption (8). Similarly, while Navero-Castillejos et al. recommended using antigen tests solely for identifying highly infectious individuals (10), Regev-Yochay et al. observed high sensitivity across symptomatic and asymptomatic patients alike (14). Kohmer et al. also noted a significant correlation between antigen test outcomes and cell culture infectivity, underscoring their potential utility in managing COVID-19 (9).
Adding to this body of work, we employed our Ag-RDT (ALLtest) in a substantial cohort across three international centers. Our findings revealed high clinical sensitivities (93.18%–100%) and specificities (99.67%–100%) in suspected COVID-19 cases when compared to RT-PCR. This outperformed six other commercial rapid antigen tests, which showed sensitivities ranging from 65% to 79% (10). According to WHO standards — a sensitivity of ≥80% and specificity of ≥97% — our ALLtest demonstrated excellent efficacy in all three centers, meeting the criteria for SARS-CoV-2 detection. However, historical data revealed that ALLtest was grouped among those with low sensitivity (16.7%) in a review of 122 Ag-RDTs by Nubling et al. (15). Nonetheless, recent studies, such as those by Moons et al. and Sivro et al., show more promising results, with higher sensitivities observed in nasal versus saliva samples (83.9%) and reasonable detection (about 74%) of Omicron BA.4 and BA.5 variants (16–17). Overall, the ALLtest exhibits generally qualified performance amid evolving epidemiological landscapes.
The Ct value, indicative of the quantity of viral RNA, has been recommended for inclusion alongside binary RT-PCR outcomes to enhance their clinical utility (18). Bullard et al. observed that no viable viral cultures were produced from samples with a Ct value greater than 24 (19). Additionally, studies have shown that samples with a Ct value exceeding 30 (2.17×105 E gene copies/mL) are typically not cultivable (20). The sensitivity of the ALLtest correlates with viral loads, consistent with previous findings (21–22). Similar to other research (14), the sensitivity of ALLtest was higher in samples with a Ct value of 30 or less (99.30%, 95% CI: 97.48%, 99.91%) and increased to 100% (95% CI: 98.38%, 100%) in samples with a Ct value of 25 or less. Significantly lower Ct values were also observed in ALLtest-positive cases among participants with detectable Ct values across all three centers (Figure 3A, 3B, and
Supplementary Table S4 ). According to Kucirka et al., RT-PCR sensitivity and viral load typically increase within 5–7 days post-infection, stabilize for 1–2 weeks, and subsequently decrease (4). Furthermore, a significant difference in the timing of symptoms was found between ALLtest positive and negative groups, with those displaying symptoms earlier (2.25 days vs. 2.64 days) more likely to test positive with ALLtest (P=0.0018).In this study, we exclusively utilized NPS for both Ag-RDT and RT-PCR. This limitation may affect the generalizability of the results, as the performance of the Ag-RDT could vary with other sample types, such as oropharyngeal swabs or saliva. And due to the difficulty of collecting enough number of participants infected by the recent coronavirus strain, we only validated the detection effect of ALLtest on those strains in lab. In the future, multiple commonly used Ag-RDT will be tested compared with ALLtest on a larger COVID-19-infected population.
We developed and validated the ALLtest antigen test for the early diagnosis of COVID-19 across three international centers. Given its high sensitivity and specificity, we propose that the ALLtest can serve as a reliable adjunct to the RT-PCR test.
HTML
Preparation and Characterization of Monoclonal Antibodies (mAbs) Against SARS-CoV-2 N Protein
The Design of Ag-RDT Assay for COVID-19
Determination of the ALLtest Ag-RDT Assay Sensitivity and Specificity
Evaluation of the Application of the SARS-CoV-2 Variant Strains
Validation of Clinical Samples
Statistical Analysis
Preparation and Characterization of mAbs Against N Protein
The Assessment of the Sensitivity and Specificity of the Ag-RDT Assay
Performance Evaluation of the Ag-RDT Assay with SARS-CoV-2 Variants
The Clinical Validation of the Ag-RDT Assay
Factors Correlated with Our Antigen Results
| Citation: |

|