
 Download:
Download:




-
Human life expectancy is currently at its highest and is expected to continue rising. In China, there are 240 million individuals aged 60 years and older, and this number is projected to exceed 400 million, constituting roughly one-third of the total population by 2035 (1). Addressing the diverse health-related issues associated with this demographic shift presents a significant challenge for society.
Health status is a multidimensional composite state that includes physical health, mental well-being, and social adaptation (2-3). The health status of older individuals is influenced by various factors throughout their lives. Cohort studies are scientifically valuable for providing in-depth insights into the mechanisms of health changes and development, as well as for formulating effective intervention measures.
In 2015, the World Health Organization (WHO) released the “World Report on Ageing and Health” (2-3). The report emphasized that the goal of Healthy Aging is to aid in “developing and maintaining the functional ability necessary for health in old age.” The core framework comprises two key concepts: “intrinsic capacity” and “functional ability,” along with the interaction between the individuals and their environment. The maintenance of functional ability is fundamental to achieving healthy aging, and functional performance is a crucial factor in promoting it.
This study aims to understand the development and evolution of health status across the lifespan by establishing a comprehensive, health-oriented cohort of individuals aged 25 to 89 from seven major geographical regions in China. The cohort focuses on improving functional ability in older adults and identifying various positive factors throughout the life course. Additionally, the study will incorporate advanced multimodal analysis to measure biological aging, contributing to the prevention and/or delay of functional decline.
-
The PENG ZU Study on Healthy Aging in China is a prospective observational study.
-
The primary objectives of the PENG ZU cohort are: 1) to establish a high-quality aging cohort with standardized data collection of key variables and biospecimens; 2) to use real-world data to understand the realistic processes in Chinese health status brought about by aging (natural course); 3) to evaluate functional decline associated with aging, particularly the deterioration of intrinsic capacity, identifying its trajectory over time and correlation with various health outcomes; 4) to uncover the underlying mechanisms of systemic aging and intrinsic capacity decline by identifying and validating multidimensional aging biomarkers; and 5) to develop a novel approach for big data analysis of health information, and to build evaluation and prediction models for functional decline, with translational applications.
This study focuses on key composite health events throughout the life course, including: 1) the trajectory of functional decline (e.g., intrinsic capacity, functional ability, disabilities) and its relationships with associated factors; 2) disease occurrence (e.g., heart disease, cancer, diabetes); and 3) mortality.
The goal of this project is to understand current health conditions and related influencing factors, dynamically monitor changes in population health, promptly detect age-related functional changes and health risks, provide intervention guidelines, slow functional decline and disease occurrence, as well as maintain overall health levels.
-
The PENG ZU cohort is an observational study that examines health status in a real-world setting. Given the exploratory objectives of the PENG ZU cohort, calculating an epidemiological sample size is unnecessary. To ensure an adequate number of participants for follow-up visits, the study aims to recruit at least 26,000 community-based participants aged 25 to 89 years. These participants are stratified into 13 five-year age groups, each consisting of approximately 1,000 males and 1,000 females. Recruitment occurs across seven major geographical regions in China (Northeast, North China, Central China, East China, South China, Southwest, and Northwest), reflecting diverse geographical distributions and lifestyle habits. For participants aged 60 and above, follow-up visits occur biennially, whereas for those under 60, follow-up visits take place every four years. Figure 1 presents a schematic overview of the study procedures.
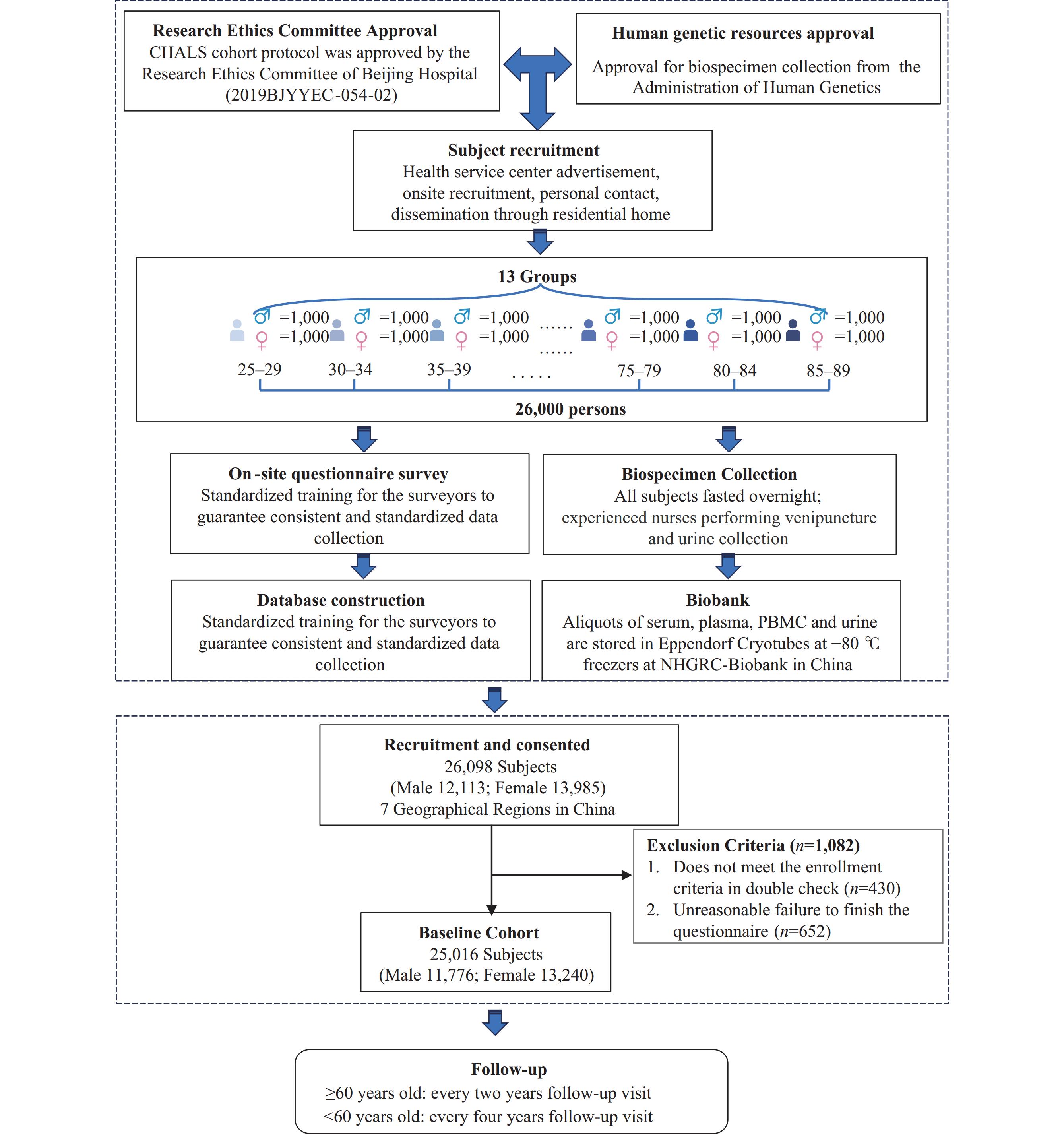 Figure 1.
Figure 1.The PENG ZU cohort baseline: first wave of data collection.
The inclusion criteria were as follows: 1) aged 25–89 years; 2) provided signed informed consent; 3) locally residing individuals of appropriate age with stable employment and residence; 4) free from acute diseases; 5) no progressive life-threatening diseases; 6) no mental disorders; 7) no history of alcohol or substance abuse; and 8) no criminal record. Exclusion criteria included individuals: 1) at risk of migration or relocation; or 2) with any physical or mental functional impairments preventing survey completion.
-
Participants were recruited for the study through advertisements placed in health examination centers and community settings. Volunteers from the medical examination centers are considered representative of the general population, showing consistency with community residents in terms of physical health, mental health, and social adaptation. Health information data, including demographics, physical and mental health status, and socio-economic-environmental conditions, were collected at baseline and during follow-up visits. Table 1 outlines the PENG Zu cohort study flow chart and details all data collected at baseline.
Categories Variables Baseline Follow-up Recruitment √ Informed consent √ Eligibility criteria checked √ Demographic information Age, sex, education, religion, marital status, occupation √ Lifestyle information Life satisfaction, working and leisure, physical activity, sedentarily time, smoking, alcohol consumption, health production supplementation, food frequency, sleep status, social participation √ √ Physical condition Self-health satisfaction, vision loss, hearing loss, tooth loss, appetite, stools and urination, discomfort (fatigue/dysphoria/inattention/impulse/self-reported visceral pain/ allergy), ADL, IADL (4–5) self-reported disease history, medication, vaccination, and health consciousness √ √ Physical examination Body mass index, waist and hip circumference, blood pressure, grip strength, gait speed (comfortable and maximal), TUG, balance test,Chair-stand test, VRT √ √ Mental condition TIPI (6–7), DAP-R (8), mental health (9), aging attitude (10–11), mental health for interpersonal communication/self-awareness/emotional experience/cognitive efficacy (12), DASS-21 (13), Mini-MoCA √ √ Social economic and environment state Family relationship, colleagues’ relationship, friendship, demand and usage of social services, economic state, insurance, Living environment, housing condition, supporting facilities √ √ Other examinations* Clinical laboratory examination (47 indicators): complete blood count, blood biochemistry indexes, blood ions, hormones, tumor biomarkers, etc.; BIA, chest CT electrocardiogram, MRI √ √ Abbreviation: ADL=activities of daily living; IADL=instrumental activities of daily living; TUG=timed up and go test; VRT=visual reaction test; DAP-R=death attitude profile-revised; TIPI=ten-item personality inventory; DASS-21=depression anxiety stress scales; Mini-MoCA=mini montreal cognitive assessment 5-minute; BIA=body composition; CT=computed tomography; MRI=magnetic resonance imaging.
* Other examinations are proposed for a partial number of participants.Table 1. The PENG ZU cohort flowchart.
-
Biospecimens, including blood and urine, were collected at baseline and follow-up visits. Samples from various satellite centers were transported via express cold chain logistics to the National Human Genetic Resources Center Biobank (NHGRC-Biobank) in China, where they were stored in smaller aliquots at −80 ℃. The PENG ZU cohort biobank is overseen by the National Health Commission of the People’s Republic of China.
Blood sample collection: After an overnight fast, all participants donated 10 mL of blood via venipuncture into two 5 mL vacuum plastic blood collection tubes: one coated with EDTA anticoagulant (Greiner Bio-One, Austria) and one with coagulant (Greiner Bio-One, Austria). The samples were processed to isolate plasma, serum, and peripheral blood mononuclear cells (PBMCs).
Urine sample collection: Participants were instructed to collect midstream first-morning urine samples in sterile screw-top containers. The urine samples were then transferred into 10 mL vacutainer tubes (Gongdong Medical Technology, China) and transported via express cold chain logistics to the NHGRC-Biobank. There, urine aliquots were prepared and stored in a −80 °C freezer within the NHGRC-Biobank.
-
The design of the prototype system has resulted in a standardized aging health database for data collection, analysis, and sharing. This platform integrates data from various sources, utilizing outlier handling algorithms and offering multidimensional analysis for clear insights. It features secure data sharing with multi-level permissions and watermark technology for traceability. The system includes user and administrator modules, with extensive data storage and large-scale parallel computing for efficient health data processing and visualized analysis.
A scientific committee has been established for the biobank and database to define scientific trajectories and research priorities. Its responsibilities include evaluating ongoing projects and their progress, addressing ethical or methodological issues arising from the studies, and assessing the relevance, feasibility, and execution of proposed analyses. Additionally, the committee ensures that the transfer of biospecimens is regulated by Material Transfer Agreements (MTAs). Data disclosure will adhere to strict anonymity protocols by utilizing coded and traceable information.
-
A comprehensive statistical analysis plan was developed to address the study’s specific aims. To investigate potential significant differences in certain indicators across various age groups and sexes, differential analysis methods, including independent sample t-tests and Kolmogorov-Smirnov tests, will be employed. The multidimensional correlation among indicators will be examined using Pearson’s correlation and regression analysis. Machine learning techniques will be considered to handle the extensive and diverse data collected from questionnaire surveys, clinical evaluations, biospecimen multi-omics examinations, and digital assessments. Statistical significance will be determined at P≤0.05.
-
To ensure data quality, we established a standardized workflow encompassing subject recruitment, on-site questionnaire surveys, physical examinations, biospecimen collection, biobanking protocols, clinical testing, and data collection.
Recruitment strategies: Baseline recruitment primarily utilizes the following strategies: advertisements at community health service centers, onsite recruitment, personal contact, and dissemination through residential homes. These strategies are monitored and updated as necessary throughout the recruitment period.
Questionnaire design: The team comprised geriatric specialists, psychologists, and sociologists, who collaborated extensively to draft the preliminary version of the questionnaire. A small-scale test involving 150 participants across all age groups was conducted to refine the draft, ensuring all questions were clear, concise, and free from ambiguity, and to confirm the questionnaire’s length was suitable to prevent respondent fatigue.
On-site questionnaire survey: All surveyors were recruited from nurses, technicians, and medical students with medical backgrounds. The project team provided standardized training to ensure consistent data collection. Additionally, supervisors were appointed to regularly visit each site to monitor the survey process and provide feedback to surveyors, ensuring adherence to the prescribed standards for conducting questionnaire interviews.
A specialized data management team oversaw the entire data management process of the study, which included reviewing procedures for data collection, validation, and cleaning. Data encryption technology was utilized in constructing the database to prevent unauthorized access, tampering, or data leakage.
Biospecimen collection: To ensure the quality of biosamples during collection, transportation, division, and storage, corresponding technical specifications were established. Standardized operating procedures for various types of biosamples have been implemented to meet the timeliness requirements of testing projects.
-
The PENG ZU Cohort Study adhered to the Declaration of Helsinki, embodying the fundamental principles of clinical research ethics. The study protocol received approval from the Beijing Hospital Research Ethics Committee (2019BJYYEC-054-02) in March 2019. In line with the regulations of the People’s Republic of China on the Administration of Human Genetics, the collection of biospecimens was conducted under the authorized collection of human genetic resources.
-
Baseline recruitment concluded in October 2021. Collaborating with around 1,000 team members from nine cohort recruitment sites across seven major geographical regions in China, this study successfully recruited 26,098 participants. Quantitative and qualitative data, along with biological samples, were collected from 25,016 individuals. All participants consented to biobanking. Detailed baseline information for the participants is provided in Table 2.
Variables Total (n, %) Male Female Age (years) 54.9±17.4 55.0±17.6 54.7±17.2 Total 25,016 11,776 (47.07) 13,240 (52.93) Area Urban 16,448 (65.75) 7,705 (65.43) 8,743 (66.00) Rural 8,568 (34.25) 4,071 (34.57) 4,497 (34.00) Education Illiteracy 1,889 (7.55) 565 (4.80) 1,324 (10.00) Primary Education 3,870 (15.47) 1,672 (14.20) 2,198 (16.60) Secondary Education 11,860 (47.41) 5,982 (50.80) 5,878 (44.40) Higher Education 7,397 (29.57) 3,557 (30.20) 3,840 (29.00) Marital Status Single 1,980 (7.91) 1,119 (9.50) 861 (6.50) Married (Living Together) 18,856 (75.38) 9,138 (77.60) 9,718 (73.40) Married (Separated) 868 (3.47) 471 (4.00) 397 (3.00) Divorced 778 (3.11) 341 (2.90) 437 (3.30) Widowed 2,534 (10.13) 707 (6.00) 1,827 (13.80) Living status Living alone 2,250 (9.00) 1,072 (9.10) 1,178 (8.9) Living not alone 22,766 (91.00) 10,704 (90.90) 12,062 (91.1) Table 2. Baseline information of participants in PENG ZU cohort.
The average age of the volunteers was 54.9 years. Among the participants, 11,776 were male (47.07% of the total population) and 13,240 were female (52.93% of the total population). Additionally, 16,448 participants resided in urban areas, while 8,568 lived in rural areas.
The educational background of the surveyed participants revealed that 1,889 individuals (7.55%) were illiterate, 3,870 (15.74%) had primary education (elementary school), 11,860 (47.41%) had secondary education (middle school, high school, or vocational school), and 7,397 (29.57%) had higher education (junior college, undergraduate, master’s, or doctorate degrees).
Of the total surveyed population, 1,980 individuals (7.91%) reported being unmarried; 18,856 (75.38%) reported being married and living together; 868 (3.47%) reported being married but living separately; 778 (3.11%) were divorced, and 2,534 (10.13%) were widowed. Concerning living status, 2,250 individuals (9.0%) reported living alone, while more than 90% lived with others.
-
The PENG ZU cohort biobank was established to provide a crucial platform for researching molecular biomarkers of aging. Biological samples collected from 25,016 participants were aliquoted and stored at −80 °C. The objective is to identify aging biomarkers that align with the characteristics of aging in the Chinese population.
-
This project has successfully completed data collection, cleaning, and storage, culminating in the automatic generation of reports. A statistical analysis plan for aging data has been developed, including current status descriptions (absolute trend analysis, relative trend analysis, and data visualization). Single-dimensional, single-index analysis has been performed using regression analysis and change-point detection methods to assess aging trends.
-
The PENG ZU cohort exhibits a wide geographical distribution and significant diversity in its characteristics. This extensive database encompasses information on physical health, mental well-being, and social adaptation. Unlike other established cohorts such as China Health and Retirement Longitudinal Study (CHARLS), English Longitudinal Study of Ageing (ELSA), and Korean Longitudinal Study of Aging (KLoSA), which typically include participants aged 45 or 50 and above, the PENG ZU cohort includes individuals aged 25 to 89 years. Benoit et al. identified three peaks at ages 34, 60, and 78 in plasma proteome profiles, indicating that aging processes may begin as early as the thirties (14). To achieve successful health aging, it is essential to intervene early in life. Furthermore, this study differentiates itself from previous research that predominantly focused on health outcomes by emphasizing the understanding of physical and cognitive functional decline during aging. It aims to elucidate the interrelationships among social, psychological, physiological factors, and lifestyle. The PENG ZU cohort has also developed an extensive biobank and database, offering an ideal research platform for comprehensive analysis and screening of aging biomarkers. Presently, both baseline and laboratory data analyses have been completed. The findings from this study will provide technological support for understanding health changes over time due to aging and offer recommendations for efficient and effective interventions to maintain functional ability and promote healthy aging in China.
HTML
Objectives
Study Population
Data Collection
Biobanking
Database Construction
Statistical Methods
Quality Control
Ethics Approval and Human Genetic Resources
Recruitment Status
Biobanking and Biomarker Mining
Data Collection and Analysis
| Citation: |

|