
 Download:
Download:




-
Thallium (Tl) is a highly toxic metal that has been designated as a priority environmental pollutant by the United States Environmental Protection Agency and included in China’s 12th and 13th Five-Year Plans (1). While Tl is known to be nephrotoxic in cases of acute and subacute exposure, data on nephrotoxicity resulting from chronic exposure remain limited (2). The global incidence and prevalence of chronic kidney disease (CKD) have increased dramatically, making it a significant public health concern. In 2017, there were 697.5 million cases of CKD at all stages worldwide (3). Given China’s large population, the economic and disease burden posed by CKD on both society and the national healthcare system are considerable (4). Consequently, extensive epidemiological studies are urgently needed to identify risk factors for CKD. Prior research has identified significant associations between Tl exposure and decreased kidney function (5-6), though the findings have not been consistent. This study investigates the association between urinary Tl and renal function, and further evaluates the potential mediating effect of inflammatory biomarkers, using data from the China National Human Biomonitoring (CNHBM) program.
In this study, participants younger than 18 years old and those with missing data on urinary Tl, serum creatinine (SCr), and inflammatory biomarkers were excluded. Following these exclusions, a total of 9,238 participants were included in the final analysis. The concentration of urinary Tl was measured using multi-element analysis via inductively coupled plasma mass spectrometry (ICP-MS) (PerkinElmer NexION 350, Turku, Finland).
This study utilized the Modification of Diet in Renal Disease (MDRD) equation to calculate the estimated glomerular filtration rate (eGFR), incorporating SCr, age, and gender. This method provides significant advantages in distinguishing various stages of CKD. The GFR measures the rate at which the glomeruli filter metabolites, waste, and toxins from plasma to produce ultrafiltrate, serving as a comprehensive indicator of kidney function. Clinical guidelines use eGFR for diagnosing and staging CKD, classifying eGFR values of less than 60 mL/[min·(1.73 m2)] as indicative of CKD (7).
Continuous variables were presented as weighted mean (standard error, SE) or median (P25–P75), while categorical variables were represented as weighted percentages. Differences between continuous variables were assessed using analysis of variance or the rank sum test, depending on data distribution, and chi-square tests were employed for categorical variables. P<0.05 were considered statistically significant. Detailed definitions of covariates are provided in the Supplementary Material. The association between urinary Tl and CKD was examined using a multiple logistic regression model. Subsequently, a multiple linear regression model was applied to estimate the regression coefficients (β) and 95% confidence interval (CI) of eGFR with respect to urinary Tl levels. A restricted cubic spline (RCS) with knots at the 25th, 50th, and 75th percentiles was utilized to explore dose-response relationships. To evaluate the role of inflammatory biomarkers, such as hypersensitive C-reactive protein (CRP), neutrophils, lymphocytes, and white blood cells (WBC), in the relationship between urinary Tl and eGFR, a mediation analysis was conducted using the mediation R package. Subgroup and sensitivity analyses were also performed, with detailed results available in the
Supplementary Material .The weighted median (P25–P75) of urinary Tl was 0.27 (0.16, 0.45) μg/L. The prevalence of CKD was 7.75%, and the weighted mean value of eGFR was 93.89 mL/[min·(1.73 m2)]. Additional baseline characteristics of the participants are detailed in
Supplementary Table S1 .The highest quartile of urinary Tl was associated with an increased risk of CKD, exhibiting an adjusted odds ratio (OR) of 1.77 (95% CI: 1.04, 3.02) compared to the lowest quartile. Furthermore, for each additional interquartile range (IQR) of urinary Tl, the risk of CKD increased by 14% (OR=1.14, 95% CI: 1.02, 1.26) (Table 1). There was also a negative relationship between urinary Tl and eGFR, with a decrease in eGFR of 1.45 units (β=−1.45, 95% CI: −2.88, −0.02) for each unit increase in urinary Tl (
Supplementary Table S2 ).Urinary Tl OR (95% CI) Crude model Model 1* Model 2† Model 3§ Model 4¶ Q1 (Reference) 1.00 1.00 1.00 1.00 1.00 Q2 0.93 (0.72, 1.20) 1.16 (0.88, 1.52) 1.14 (0.86, 1.50) 1.18 (0.90, 1.55) 1.14 (0.86, 1.51) Q3 0.92 (0.66, 1.26) 1.27 (0.90, 1.80) 1.24 (0.87, 1.76) 1.29 (0.90, 1.87) 1.19 (0.81, 1.76) Q4 1.51 (1.01, 2.24)** 2.08 (1.34, 3.24)** 1.99 (1.28, 3.10)** 2.09 (1.26, 3.48)** 1.77 (1.04, 3.02)** Per IQR 1.14 (1.04, 1.24)** 1.19 (1.09, 1.30)** 1.18 (1.07, 1.29)** 1.19 (1.07, 1.31)** 1.14 (1.02, 1.26)** Note: Q1=urinary Tl ≤0.16 μg/L; Q2=0.16 μg/L<urinary Tl≤0.28 μg/L; Q3=0.28 μg/L<urinary Tl≤0.46 μg/L; Q4=urinary Tl>0.46 μg/L.
Abbreviation: CI=confidence interval; CKD=chronic kidney disease; Tl=thallium; OR=odds ratio; IQR=interquartile range; BMI=body mass index; UCr=urine creatinine; TC=total cholesterol; Cd=cadmium; Pb=lead; Hg=mercury; As=arsenic.
* Adjusted for age, sex, education, residence, marital status, and household income.
† Additionally adjusted for smoking status, drinking status, meat consumption, and vegetable consumption.
§ Additionally adjusted for hypertension, diabetes, BMI, UCr, and TC.
¶ Additionally adjusted for urinary Cd, urinary Pb, urinary Hg, and urinary As.
** P<0.05.Table 1. Weighted odds ratios (95% CI) of CKD associated with urinary Tl concentration among Chinese adults in 2017–2018.
Urinary Tl exhibited a positive linear dose-response relationship with the risk of CKD within the RCS (P for linearity <0.05). Furthermore, RCS analysis indicated a negative downward dose-response association between urinary Tl and eGFR (P for linearity <0.05) (Figure 1).
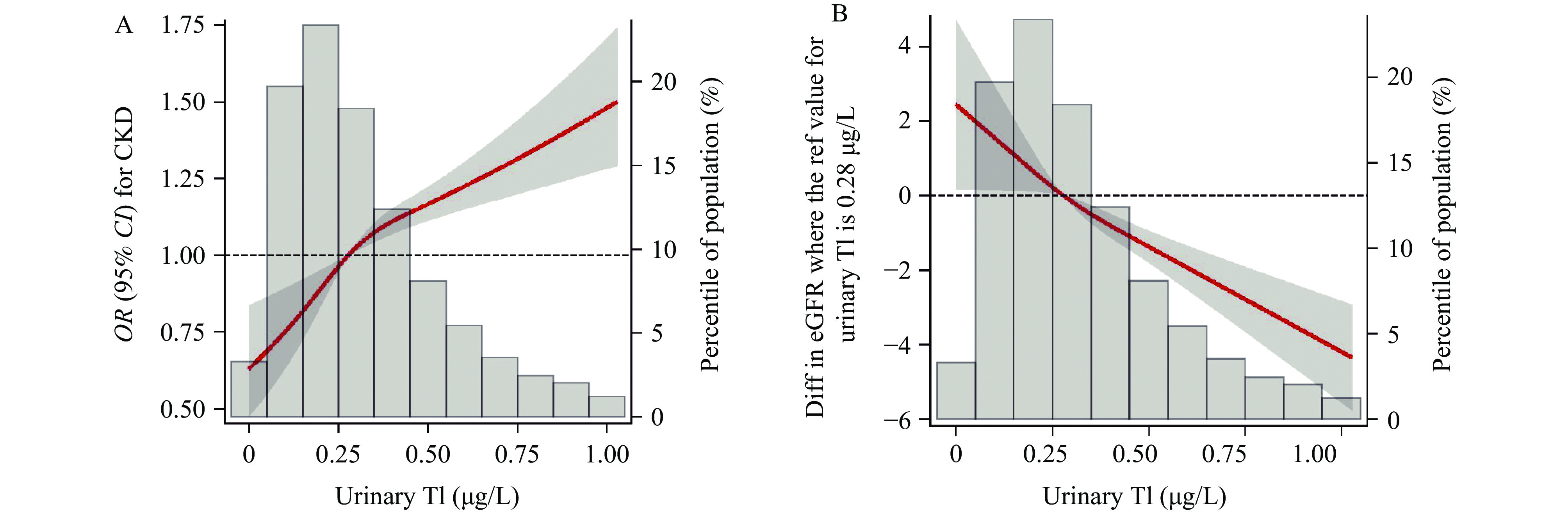 Figure 1.
Figure 1.Restricted cubic spline for the association of urinary Tl with CKD and eGFR among Chinese adults in 2017–2018. (A) the dose-response relationship between urinary Tl and CKD; (B) the dose-response relationship between urinary Tl and eGFR.
Note: In the Figure 1A and 1B, the reference value was set at the 50th percentage of urinary Tl. Models were adjusted for age, sex, education, residence, marital status, household income, smoking status, drinking status, meat consumption, vegetable consumption, hypertension, diabetes, BMI, UCr, TC, urinary Cd, urinary Pb, urinary Hg, and urinary As.
Abbreviation: OR=odds ratio; CI=confidence interval; Tl=thallium; CKD=chronic kidney disease; eGFR=estimated glomerular filtration rate; BMI=body mass index; UCr=urine creatinine; TC=total cholesterol; Cd=cadmium; Pb=lead; Hg=mercury; As=arsenic.
Compared with the lowest quartile of urinary Tl, the second, third, and highest quartiles were all positively associated with the neutrophil ratio (P<0.05). Additionally, the third and highest quartiles of urinary Tl exhibited a negative relationship with the lymphocyte ratio (P<0.05) (Table 2). Each unit increase in the lymphocyte ratio corresponded with a 0.69 mL/[min·(1.73 m2)] (95% CI: −1.30, −0.09) decrease in eGFR (
Supplementary Table S3 ). However, mediation analysis results indicated no mediating role for the lymphocyte ratio in the association between Tl and eGFR (Supplementary Table S4 ).Urinary Tl β (95% CI) CRP Neutrophil ratio Lymphocyte ratio WBC Q1 (Reference) 0 0 0 0 Q2 −0.30 (−0.74, 0.13) 1.06 (0.12, 2.30)* 0.59 (−2.44, 3.62) 0.07 (−0.14, 0.27) Q3 0.08 (−0.50, 0.66) 1.13 (0.01, 2.25)* −1.46 (−2.61, −0.32)* 0.06 (−0.11, 0.23) Q4 −0.11 (−0.73, 0.52) 1.19 (0.09, 2.30)* −1.26 (−2.44, −0.08)* 0.13 (−0.10, 0.36) Per IQR −0.07 (−0.19, 0.05) 0.37 (−0.01, 0.75) −0.50 (−1.07, 0.08) 0.02 (−0.06, 0.10) Note: Q1=urinary Tl≤0.16 μg/L; Q2=0.16μg/L<urinary Tl≤0.28 μg/L; Q3=0.28 μg/L<urinary Tl≤0.46 μg/L; Q4=urinary Tl>0.46 μg/L.
Abbreviation: CI=confidence interval; Tl=thallium; CRP=C−reactive protein; WBC=white blood cell count; IQR=interquartile range; BMI=body mass index; UCr=urine creatinine; TC=total cholesterol.
Adjusted for age, sex, education, residence, marital status, household income, smoking status, drinking status, meat consumption, vegetable consumption, hypertension, diabetes, BMI, UCr, and TC.
* P<0.05.Table 2. Weighted regression coefficients (β) and 95% CI for the association of urinary Tl with inflammatory indicators among Chinese adults in 2017–2018.
Subgroup analyses stratified by gender and age group revealed a significant positive association between urinary Tl levels and CKD in women. Further examination by age indicated more pronounced positive effects in older adults (
Supplementary Table S5 ). Sensitivity analyses, utilizing eGFR calculated via the CKD Epidemiology Collaboration (CKD-EPI) equation, corroborated these findings, demonstrating a stable association between urinary Tl levels and reduced renal function (Supplementary Table S6 ). -
Our study found a significant positive association between higher urinary Tl exposure and increased prevalence of CKD, as well as a decrease in eGFR. Notably, the positive associations with CKD were more pronounced in older adults.
The association between Tl and renal function remains inconclusive based on previous epidemiological studies. Urinary Tl has not been linked to an increased prevalence of CKD in the Chinese community of older adults in both single exposure and mixed metal exposure analyses (8). Conversely, a positive association has been reported between Tl and higher SCr- and cystatin-C-based eGFR in occupational populations, with the association persisting after adjustments for cadmium (Cd) and antimony (Sb) (5). Our study supports the hypothesis that Tl is associated with decreased renal function, aligning with a study in China that found significant impairment in kidney function among six children exposed to Tl (6). Discrepancies in results could be due to differences in participant characteristics, such as age and exposure concentrations. In our study, we adjusted for CKD risk factors, including hypertension, diabetes, total cholesterol (TC), BMI, and urinary metals, enhancing the robustness of our findings. We observed a stronger association between Tl and CKD in women. Prior research has suggested that females may be more susceptible to kidney damage from heavy metals, possibly due to reduced estrogen production, which can diminish antioxidative capacity (9). A study in Taiwan, China, documented a decline in eGFR with age among subjects exposed to multiple metals (10). Our results are consistent with this finding, showing a higher risk of CKD in the 60–79 age group. The mechanism of Tl toxicity to the kidney remains incompletely understood. Animal studies have demonstrated nephrotoxic effects of Tl, with rat kidneys showing the highest accumulation of the metal (11). Previous research has indicated that high Tl exposure is associated with elevated CRP levels, suggesting that inflammation partly mediates effects of Tl on lung function (12). In this study, we identified an increased neutrophil ratio and a decreased lymphocyte ratio in individuals with high urinary Tl, indicating a positive association between Tl and inflammatory responses. Further in vivo and in vitro research is needed to explore the mechanisms underlying this relationship.
This cross-sectional study design limits our ability to determine the temporal relationship between exposure and outcome, introducing the risk of reverse causality. However, previous research using data from National Health and Nutrition Examination Survey (NHANES) has shown that as eGFR decreases, urinary Tl concentrations also decline, while urinary metal concentrations tend to rise with improved kidney function (13). These findings indicate that variations in renal function could affect urinary metal concentrations, potentially underestimating the true association between urinary metals and disease risk.
This study is subject to some limitations. First, urine microalbumin was not assessed, relying solely on eGFR for defining CKD, which could potentially underestimate the prevalence of CKD. Second, urinary Tl levels were measured using convenience samples rather than 24-hour urine collections, possibly introducing bias in estimating actual Tl exposure.
Tl exposure primarily occurs through the consumption of vegetables and potable water contaminated with Tl. Industrialization, along with the rapid development of mining and metal smelting, has exacerbated Tl contamination in surface water and soil. It is imperative to enhance monitoring of Tl levels in potable water, vegetables, and aquatic organisms, particularly in areas prone to Tl pollution such as those near Tl mining sites, thermal power plants, and metal smelting facilities. The current standards for Tl in surface and drinking water were established two decades ago and require urgent revision based on recent scientific findings. Moreover, existing toxicological data on both carcinogenic and non-carcinogenic effects of Tl are scarce, necessitating further research to better understand its potential health risks. Our study identified a significant link between Tl exposure and an increased risk of CKD and reduced eGFR, particularly among older adults. Given the critical issue of metal pollution, it is crucial to mitigate or eliminate renal toxic metal exposure to lessen the impact on renal function decline.
HTML
| Citation: |

|