
 Download:
Download:




-
Air pollution continues to be a significant risk factor for disability and is associated with approximately 6.67 million global deaths annually (1). According to the 2018 Guangdong Ecological Environment Report, ozone (O3) and fine particulate matter (PM2.5), accounting for 55.5% and 17.0% of primary pollutants, respectively, are the predominant contaminants in the Pearl River Delta region’s 9 cities (2). It has been established that PM2.5 and O3 are positively associated with the incidence and mortality rates of respiratory diseases, which may also have interaction effects between O3 and PM2.5 on population health (3).
In this study, we employed a generalized additive model (GAM) to analyze the associations between O3 and PM2.5 concentrations and mortality rates from respiratory diseases, chronic obstructive pulmonary disease (COPD), and lung cancer in Guangzhou. Additionally, we applied the quantile g-computation (QG-C) model to assess the combined effects of these pollutants on mortality related to respiratory conditions. Our findings contribute to a more comprehensive environmental health risk assessment and support the formulation of integrated prevention and control strategies.
Meteorological data, the daily maximum 8-hour average concentration of O3 and the 24-hour average concentration of PM2.5, during 2018–2021, were sourced from the Guangdong Multi-Trigger Smart Early Warning System. Respiratory diseases, COPD, and lung cancer, which are attributed to death, were classified using the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) codes with J00-J99, J40-J47, and C34, respectively.
R (version 4.2.2; R Core Team, Vienna, Austria) equipped with the “mgcv” and “dlnm” packages was utilized to develop GAMs to investigate the non-linear relationships between pollutant exposure and mortality from selected diseases. Both lagged concentrations and moving averages of pollutants were integrated into the models to consider delayed and cumulative effects. The QG-C method, utilizing the “qgcomp” package, estimated the joint effects of PM2.5 and O3 exposure, with the lowest quantile serving as the reference point (4). Subgroup analyses were performed based on age (less than 85 years and 85 years or older), sex, seasonal variations (April to September as warm and October to March as cold), and the coronavirus disease 2019 (COVID-19) pandemic periods (2018–2019 and 2020–2021).
The outcomes of the single-pollutant exposure analysis are presented as excess risk (ER) with a 95% confidence interval (CI) corresponding to every 10 μg/m3 increment in pollutant levels. For combined exposure effects, relative risks (RRs) and their 95% CIs are reported per quartile increase in pollutant concentration. Z tests were employed to assess differences between subgroups, with a P less than 0.05 denoting statistical significance.
During 2018 and 2021, Guangzhou recorded 29,258 deaths from respiratory diseases, 11,036 from COPD, and 16,901 from lung cancer (
Supplementary Table S1 ). The mortality rates for respiratory diseases and COPD declined in both genders, whereas lung cancer mortality rates varied throughout the period (Supplementary Table S2 ).The average daily concentrations were 29.34 μg/m3 for PM2.5 and 90.63 μg/m3 for O3. O3 levels exhibited a slight increase, whereas PM2.5 levels showed a significant decline (
Supplementary Figure S1A–B ). The monthly trends in O3 and PM2.5 concentrations in Guangzhou varied significantly. According to the meteorological data, the daily average temperature was 22.71 °C, and the average relative humidity was 79.14% in Guangzhou. (Supplementary Figure S1C–D ). PM2.5 levels showed a distinct seasonal pattern, peaking in winter and reaching the lowest levels in summer. Autocorrelation analysis revealed a non-stationary sequence, indicating a decrease in pollutant concentrations over time. Unlike PM2.5, O3 concentrations did not exhibit any annual variability; however, they still displayed a seasonal pattern, with the highest levels of pollution from April to September (Supplementary Figure S1E–F ).As demonstrated in Table 1 and
Supplementary Figure S2 , the highest and most statistically significant increased risk was observed on the first day (lag0) for both O3 and PM2.5 (P<0.05). As the lag time extended, the correlations between these pollutants and mortality rates gradually diminished and were no longer significant after three days (lag3), suggesting that O3 and PM2.5 primarily have acute impacts on respiratory diseases. Both PM2.5 and O3 exhibited cumulative effects on mortality from all selected diseases. The maximum cumulative effects of PM2.5 and O3 on all-cause mortality were seen at lag03, except that of O3 on respiratory disease occurred at lag04. However, when PM2.5 was set as a covariate, no significant association was observed between O3 exposure and lung cancer mortality (Supplementary Table S3 ).Lag time PM2.5, ER (95% CI) (%) O3, ER (95% CI) (%) Respiratory diseases COPD Lung cancer Respiratory diseases COPD Lung cancer Lag0 1.08 (0.62, 1.55)* 1.00 (0.26, 1.74)* 1.42 (0.81, 2.04)* 0.37 (0.19, 0.55)* 0.50 (0.20, 0.79)* 0.34 (0.12, 0.57)* Lag1 0.86 (0.49, 1.23)* 0.77 (0.18, 1.36)* 1.09 (0.61, 1.58)* 0.30 (0.16, 0.44)* 0.39 (0.16, 0.62)* 0.26 (0.08, 0.44)* Lag2 0.63 (0.35, 0.92)* 0.54 (0.09, 1.00)* 0.76 (0.38, 1.13)* 0.23 (0.12, 0.33)* 0.29 (0.11, 0.46)* 0.17 (0.04, 0.31)* Lag3 0.41 (0.18, 0.63)* 0.32 (−0.05, 0.68) 0.43 (0.13, 0.73)* 0.15 (0.07, 0.23)* 0.18 (0.04, 0.32)* 0.09 (−0.02, 0.19) Lag4 0.18 (−0.04, 0.40) 0.09 (−0.26, 0.44) 0.10 (−0.19, 0.38) 0.08 (−0.00, 0.16) 0.07 (−0.06, 0.20) 0.00 (−0.09, 0.10) Lag5 −0.04 (−0.30, 0.21) −0.14 (−0.54, 0.27) −0.23 (−0.57, 0.11) 0.00 (−0.09, 0.10) −0.03 (−0.19, 0.13) −0.08 (−0.20, 0.04) Lag01 2.65 (1.47, 3.82)* 2.51 (0.62, 4.39)* 3.65 (2.10, 5.20)* 0.77 (0.30, 1.23)* 1.14 (0.37, 1.91)* 0.72 (0.13, 1.31)* Lag02 3.06 (1.78, 4.34)* 2.61 (0.55, 4.67)* 3.83 (2.15, 5.52)* 1.03 (0.54, 1.52)* 1.40 (0.59, 2.22)* 0.79 (0.16, 1.41)* Lag03 3.28 (1.91, 4.66)* 2.72 (0.51, 4.93)* 3.90 (2.08, 5.71)* 1.12 (0.61, 1.64)* 1.46 (0.61, 2.32)* 0.85 (0.20, 1.51)* Lag04 3.15 (1.69, 4.62)* 2.70 (0.35, 5.04)* 3.42 (1.48, 5.35)* 1.14 (0.60, 1.68)* 1.41 (0.52, 2.31)* 0.77 (0.08, 1.46)* Lag05 2.77 (1.23, 4.31)* 2.32 (−0.15, 4.80) 2.92 (0.88, 4.96)* 1.07 (0.50, 1.63)* 1.23 (0.29, 2.17)* 0.64 (−0.08, 1.36)* Abbreviation: ER=excess risk; CI=confidence interval; COPD=chronic obstructive pulmonary disease; PM2.5=fine particulate matter; O3=ozone.
* P<0.05.Table 1. Excess risk associated with exposure to PM2.5 or O3 on respiratory disease mortality.
The results of the subgroup analysis assessing the impact of O3 and PM2.5 on mortality from selected diseases across various demographics and the COVID-19 pandemic period are presented (Figure 1, and
Supplementary Table S4 ). The analysis revealed minimal significant differences in the effects across age groups, sexes, and throughout the COVID-19 pandemic, suggesting that these factors may not significantly modify the association between O3/PM2.5 exposure and mortality risk from selected diseases. Notably, the warm season exhibited a higher ER for mortality from COPD associated with exposure to O3 or PM2.5 (Figure 1). Furthermore, PM2.5 exposure demonstrated a more pronounced effect on COPD mortality in males compared to females, whereas the reverse was observed for lung cancer. In terms of age, PM2.5 exposure had a stronger impact on individuals aged above 85 years, whereas O3 showed greater effects on those under 85 years.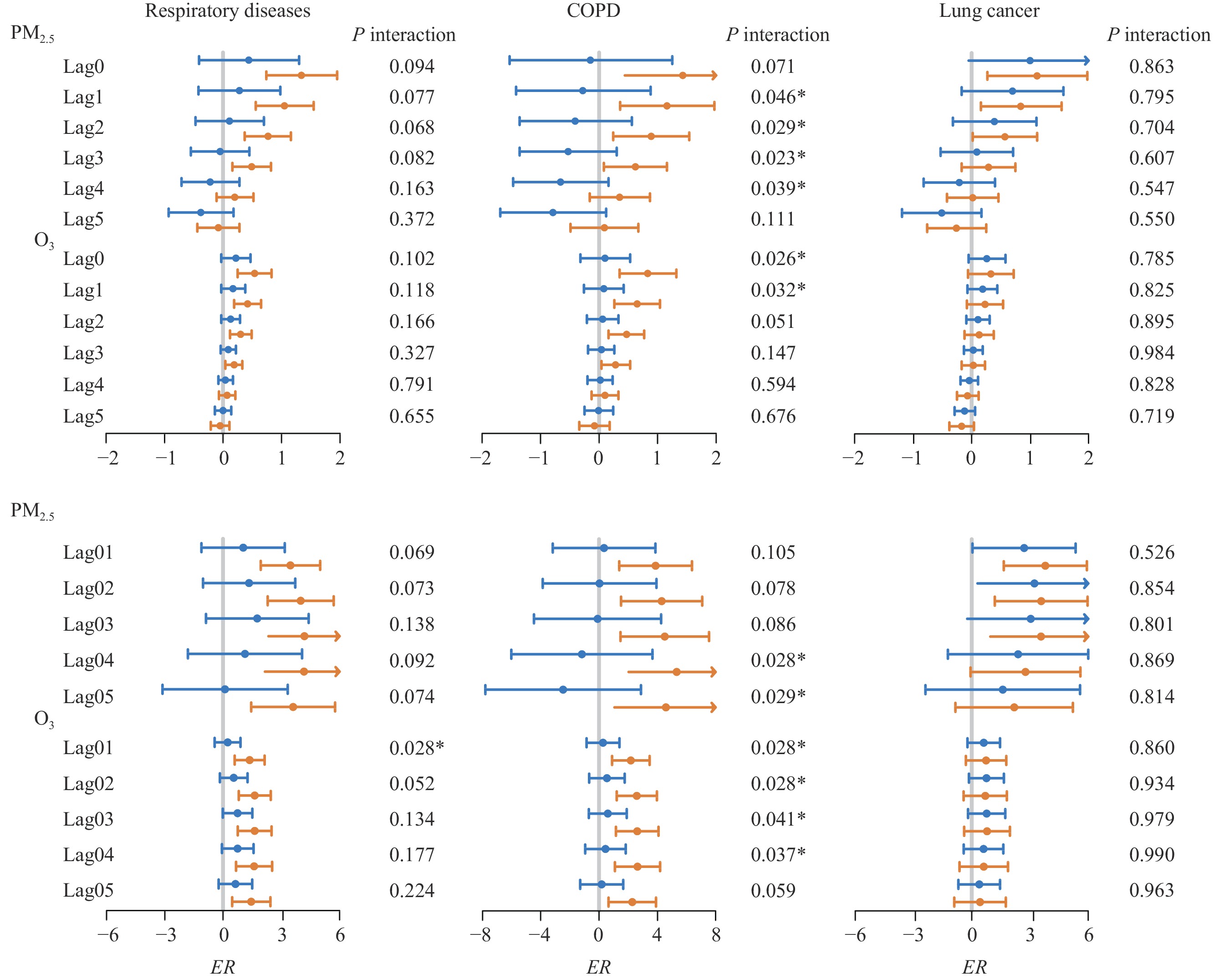 Figure 1.
Figure 1.Effects of changes in PM2.5 and O3 concentrations on mortality across cool and warm season subgroups under various lag conditions.
Note: Single lags lag0 to lag5 and cumulative lags lag01 to lag05. Blue represents the cold group; yellow represents the warm group.
Abbreviation: ER=excess risk; COPD=chronic obstructive pulmonary disease; PM2.5=fine particulate matter; O3=ozone.
* P<0.05.
Spearman correlation analysis revealed positive correlations between PM2.5 and O3, indicating potential interactions between these pollutants. In terms of meteorological factors, O3 showed a positive correlation with temperature and a negative correlation with relative humidity. Conversely, PM2.5 exhibited negative correlations with both temperature and relative humidity (
Supplementary Table S5 ).The QG-C model demonstrated that combined exposure to PM2.5 and O3 was significantly associated with increased mortality due to all selected diseases, of which the weights of two pollutants were presented in
Supplementary Figure S3 . For females and individuals aged below 85, this combined exposure was identified as a risk factor for mortality. Among males, concurrent exposure to PM2.5 and O3 was also linked to an increased risk of mortality from lung cancer. Furthermore, during the warm seasons, the correlation between combined exposure to PM2.5 and O3 and mortality from all examined diseases was evident, suggesting that higher temperatures may significantly influence respiratory-related diseases (Table 2).Group Died of respiratory diseases Died of COPD Died of lung cancer Total population 1.03 (1.01, 1.05)† 1.03 (1.00, 1.07)* 1.05(1.02, 1.08)† Age group (years) ≥85 1.03 (1.00, 1.06)* 1.03 (0.99, 1.08) 1.02 (0.95, 1.09) <85 1.04 (1.01, 1.06)† 1.04 (0.99, 1.08) 1.05 (1.03, 1.08)† Sex Male 1.01 (0.99, 1.04) 1.03 (0.99, 1.07) 1.05 (1.02, 1.08)† Female 1.06 (1.03, 1.1)†,§ 1.04 (0.98, 1.10) 1.06 (1.01, 1.11)* Season Cold 1.00 (0.97, 1.03) 0.99 (0.95, 1.04) 1.02 (0.99, 1.06) Warm 1.04 (1.02, 1.07)†,§ 1.04 (1.00, 1.08)* 1.04 (1.00, 1.07)* Time COVID-19 1.02 (0.99, 1.05) 1.03 (0.99, 1.07) 1.02 (0.99, 1.05) non-COVID-19 1.01 (0.99, 1.04) 1.02 (0.98, 1.06) 1.06 (1.02, 1.09)† Abbreviation: COPD=chronic obstructive pulmonary disease; COVID-19=coronavirus disease 2019.
* P<0.05;
† P<0.01;
§ statistically significant compared to males or cold group.Table 2. Association of combined PM2.5 and O3 exposure with mortality risk according to the QG-C model.
-
In recent years, public concern over air pollution in China, specifically regarding PM2.5 and O3 exposure, has escalated. Standards set by the Chinese Ambient Air Quality Standards (AAQSs) reveal that from 2018 to 2021, only 68.99% of days met the PM2.5 criteria. Furthermore, the compliance for O3 was even lower, with just 35.25% of days meeting the AAQSs. This data underscores the persistent air pollution threat facing residents of Guangzhou and highlights the urgent need for enhanced pollution control measures.
It has been found that higher concentrations of PM2.5 and O3 were positively correlated with an increased risk of death from respiratory diseases in this study by using a time-series design. Many epidemiological studies have consistently demonstrated significant correlations between PM2.5 and O3 exposure and both the incidence and mortality of respiratory conditions, particularly lung-related diseases (5). The associations found in this study seem to be stronger than those reported elsewhere. This discrepancy could be attributed to Guangzhou’s unique geographical characteristics (6), such as its extended warm seasons and elevated temperatures, which may enhance respiratory rates and lung ventilation, thereby heightening vulnerability to air pollutants.
Our findings indicate a positive association between combined exposure to PM2.5 and O3, and increased mortality from all selected diseases. This association may be mechanistically supported by the ability of particulate matter to reduce ultraviolet radiation penetration, thus interfering with O3 photochemical reactions. Additionally, exposure to both PM2.5 and O3 can stimulate oxidative stress in lung tissues, suggesting there are biological interactions and combined effects between these pollutants (7).
This study also presents several limitations. First, it assumes that air pollutant concentrations from monitoring stations reflect the population exposures. Second, the dataset only includes Guangzhou, which limits the generalizability of the findings. Lastly, the study’s time-series analysis design is unable to assess the long-term risks associated with air pollution.
Exposure to PM2.5 and O3 in the atmosphere is linked to an increased risk of respiratory diseases, COPD, and lung cancer mortality. The combined effects of PM2.5 and O3 further exacerbate mortality rates associated with these conditions. Given that the current levels of PM2.5 and O3 continue to pose health risks, it is crucial to enhance health protection and disease control strategies for the population in Guangzhou.
HTML
| Citation: |

|