
 Download:
Download:




-
Hearing loss (HL) and cognitive impairment are both highly prevalent neurological complications for older adults, affecting approximately 59% and 22% of older adults, respectively (1-2). A systematic review and meta-analysis showed that age-related HL was a possible biomarker and modifiable risk factor for cognitive impairment (3). However, to our knowledge, only one study has explored this association among Chinese older adults (4). Therefore, this study aimed to explore the association between HL and cognitive impairment using a large sample, community-based investigation among elderly people. This study utilized data from the second round of the Prevention and Intervention on Neurodegenerative Disease for Elderly in China (PINDEC) project, which was conducted in Liaoning, Henan, and Guangdong provinces in 2019–2020. A total of 10,347 community-dwelling older adults aged 60 years and above were recruited using a stratified, multi-stage cluster sampling method. After adjusting for confounding factors, the multivariate logistic regression analysis showed that, compared with the no HL group, the odds ratios (ORs) for cognitive impairment were 1.23 [95% confidence interval (CI): 1.08, 1.40] for mild HL, 1.55 (95% CI: 1.32, 1.82) for moderate HL, and 1.87 (95% CI: 1.47, 2.39) for severe or profound HL. The association between HL and cognitive impairment highlights the need to integrate the early identification of these problems into primary care, as both are risk factors for healthy aging and potentially preventable and/or treatable conditions.
The PINDEC project was initiated in 2015 to explore the epidemiology of neurodegenerative diseases and other common health problems, and their risk factors, among adults aged 60 years and older in China. The second round of field surveys was conducted from 2019 to 2020 in 12 districts/counties across Liaoning, Henan, and Guangdong provinces. These provinces were selected by considering their geographic location, level of economic development, and degree of aging. A stratified multi-stage cluster sampling method was used to select adults aged 60 years or older who had lived at their residence for more than 6 months in the past year. First, two or three cities in each province were selected by simple random sampling. Second, one county and one district were randomly selected in each city. Third, one township or one street was sampled at each county/district using the proportional to population size (PPS) sampling method. Fourth, cluster sampling was used to select several administrative villages or neighborhood committees in the selected townships/streets, until the survey sample size (1,000 respondents) was met. Trained local health staff conducted interviews and physical examinations with all participants to collect information on demographics, lifestyle, activities of daily living, cognitive function screening, sleep quality, hearing function, and olfactory function.
HL was measured by pure-tone audiometry. Pure-tone audiometry was performed for all individuals in a quiet room in which ambient noise did not exceed 50 dB as measured by a sound level meter. Levels of ambient noise were recorded for each subject in a questionnaire. Each ear was tested separately at 0.5, 1, 2, and 4 kHz to obtain the hearing threshold at each frequency. The average of the hearing thresholds at these four frequencies in the better ear was taken as the pure-tone average (PTA). According to the World Health Organization (WHO) 1997 hearing classification criteria (5), a PTA ≤25 dB was considered normal hearing, 26–40 dB was mild HL, 41–60 dB was moderate HL, and ≥61 dB was severe or profound HL. A uniform type of audiometer in accordance with the national standard GB/T 7341.1-2010 was used for all tests and was calibrated prior to testing. The detailed investigation workflow is shown in
Supplementary Figure S1 .Cognitive function was assessed using a Chinese version of the Mini-Mental State Examination (MMSE). Cognitive impairment was defined as an MMSE score of ≤17 for illiterate participants (0 years of education), ≤20 for those with a primary school education (1–6 years of education), and ≤24 for those with a junior high school education and above (≥7 years of education) (6).
Ethical approval was granted by the Ethnics Commitee of the National Center for Chronic and Noncommunicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention (approval number 201902). All the participants provided written informed consent prior to the survey.
A total of 12,369 participants were selected, and 12,223 completed the survey, yielding a response rate of 98.8%. After data cleaning, 1,876 participants were excluded due to incomplete sociodemographic data or lacking responses to the hearing function test or cognitive function screening questions. Finally, a total of 10,347 participants were included in this study. Demographic characteristics of the categorical variables were described as percentages in the overall population and subgroups. The chi-square test was used to analyze differences between subgroups, with a P of <0.05 considered statistically significant. Multivariable logistic regression was used to examine the association of HL with cognitive impairment. All statistical analyses were performed using SAS software (version 9.4; SAS Institute Inc., Cary, USA).
Of the 10,347 participants in the study sample, 57.2% were female, and 58.6% resided in rural areas (Table 1). The average age was 69.1±6.6 years. In 2019–2020, among older adults aged 60 years and above, the prevalence rates of mild HL, moderate HL, and severe or profound HL were 47.2% (95% CI: 46.3%, 48.2%), 18.0% (95% CI: 17.3%, 18.8%), and 4.5% (95% CI: 4.1%, 4.9%), respectively. The prevalence of moderate or higher grades of HL increased with age, from 12.8% at 60–64 years to 52.4% at 80 years and above. Across subgroups, the study found that the prevalence rates of moderate HL and severe or profound HL were likely higher among those residing in rural areas, those of older age, those with fewer years of education, and those who were widowed. There was no statistically significant difference in the prevalence of mild HL between males and females; however, the prevalence rates of moderate HL and severe or profound HL were higher in males than in females (Table 1). The prevalence of cognitive impairment was 19.1% (95% CI: 18.3%, 19.8%) overall and increased gradually with the severity of HL in both males and females (P<0.001) (Figure 1). The prevalence of cognitive impairment was 14.3% (95% CI: 13.1%, 15.5%) for those with normal hearing function, 18.4% (95% CI: 17.3%, 19.5%) for those with mild HL, 25.4% (95% CI: 23.4%, 27.4%) for those with moderate HL, and 32.3% (95% CI: 28.0%, 36.5%) for those with severe or profound HL. Among those with HL, the prevalence of cognitive impairment was higher in females than in males (Figure 1). After adjusting for confounding factors, multivariate logistic regression analysis showed that, compared with the no HL group, the ORs for cognitive impairment were 1.23 (95% CI: 1.08, 1.40) for mild HL, 1.55 (95% CI: 1.32, 1.82) for moderate HL, and 1.87 (95% CI: 1.47, 2.39) for severe or profound HL (Table 2).
Characteristics n (%) Grades of hearing loss, % (95% CI) Mild Moderate Severe or profound P Total 10,347 (100.0) 47.2 (46.3, 48.2) 18.0 (17.3, 18.8) 4.5 (4.1, 4.9) Sex <0.001 Male 4,433 (42.8) 48.0 (46.6, 49.5) 21.1 (19.9, 22.3) 5.4 (4.7, 6.0) Female 5,914 (57.2) 46.7 (45.4, 47.9) 15.8 (14.8, 16.7) 3.9 (3.4, 4.4) P for difference 0.166 <0.001 <0.001 Age (years old) <0.001 60–64 3,031 (29.3) 44.4 (42.6, 46.2) 11.0 (9.9, 12.1) 1.8 (1.3, 2.3) 65–69 3,135 (30.3) 49.8 (48.0, 51.5) 13.6 (12.4, 14.8) 2.6 (2.0, 3.1) 70–74 2,101 (20.3) 51.2 (49.1, 53.4) 20.5 (18.7, 22.2) 4.4 (3.5, 5.3) 75–79 1,171 (11.3) 46.5 (43.7, 49.4) 28.9 (26.3, 31.5) 9.0 (7.3, 10.6) 80 and above 909 (8.8) 39.7 (36.5, 42.9) 37.3 (34.1, 40.4) 15.1 (12.7, 17.4) P for trend <0.001 <0.001 <0.001 Location <0.001 Urban 4,287 (41.4) 49.4 (47.9, 50.9) 12.9 (11.9, 13.9) 2.9 (2.4, 3.4) Rural 6,060 (58.6) 45.7 (44.4, 46.9) 21.7 (20.6, 22.7) 5.7 (5.1, 6.3) P for difference <0.001 <0.001 <0.001 Education (years) <0.001 0 2,707 (26.2) 46 (44.1, 47.8) 22.4 (20.8, 24) 7.3 (6.3, 8.3) 1–6 3,933 (38.0) 48.9 (47.3, 50.4) 18.2 (17, 19.4) 4.5 (3.9, 5.1) 7–9 2,558 (24.7) 45.9 (44, 47.8) 15.3 (13.9, 16.7) 2.7 (2.1, 3.3) 10 and above 1,149 (11.1) 47.7 (44.8, 50.6) 13.3 (11.3, 15.3) 2.1 (1.3, 2.9) P for trend 0.048 <0.001 <0.001 Marital status <0.001 Non-widowed 8,249 (79.7) 47.4 (46.3, 48.5) 16.8 (16, 17.6) 4.1 (3.7, 4.5) Widowed 2,098 (20.3) 46.6 (44.5, 48.8) 23.1 (21.3, 24.9) 6.2 (5.2, 7.3) P for difference 0.521 <0.001 <0.001 Occupation <0.001 Farmer 6,308 (61.0) 48.3 (47.1, 49.5) 19.2 (18.2, 20.2) 5.4 (4.8, 5.9) Worker 2,202 (21.3) 46.0 (43.9, 48.1) 16.9 (15.4, 18.5) 3.3 (2.6, 4.1) Non-manual 1,837 (17.8) 45.1 (42.9, 47.4) 15.4 (13.8, 17.1) 3.0 (2.2, 3.8) P for difference 0.025 <0.001 <0.001 Note: Non-manual worker includes teachers, researchers, doctors, office workers, and other occupations apart from farmer and worker.
Abbreviation: CI=confidence interval.Table 1. Prevalence of hearing loss among community-dwelling elderly by different characteristics in Liaoning, Henan, and Guangdong provinces in China, 2019–2020.
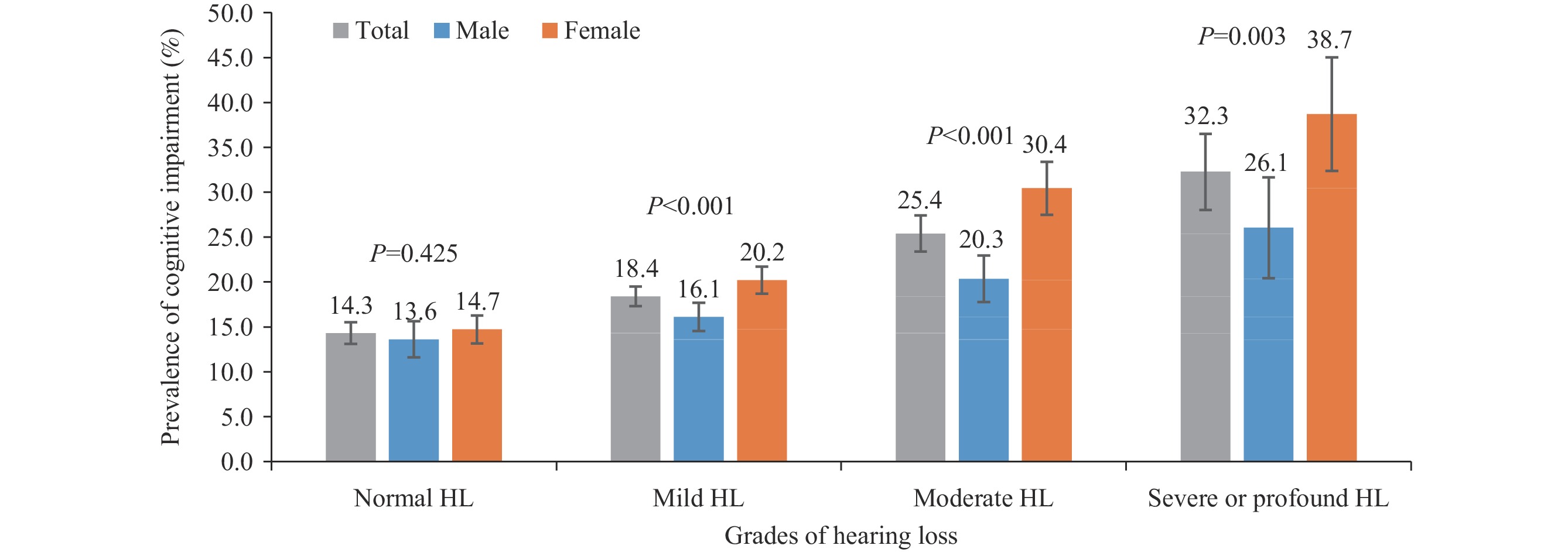 Figure 1.
Figure 1.Prevalence of cognitive impairment among elderly with different grade of HL by genders in Liaoning, Henan, and Guangdong provinces in China, 2019–2020.
Note: P denotes the prevalence difference of cognitive impairment between males and females in each grade of HL among older adults.
Abbreviation: HL=hearing loss.
Subgroups OR 95% CI P Normal HL 1.00 Mild HL 1.23 1.08–1.40 0.002 Moderate HL 1.55 1.32–1.82 <0.001 Severe or profound HL 1.87 1.47–2.39 <0.001 Note: The multivariable logistic regression had adjusted demographic variables including age, sex, urban-rural status, educational level, occupation and marital status; behavioral variables such as smoking, alcohol drinking, regular tea drinking, regular exercise, living with family, and reading; cardiovascular risk factors such as BMI, hypertension, diabetes, dyslipidemia, heart disease, and cerebrovascular disease.
Abbreviation: HL=hearing loss; CI=confidence interval; OR=odds ratio; BMI=body mass index.Table 2. Multivariable logistic regression analysis for cognitive impairment among community-dwelling elderly in Liaoning, Henan, and Guangdong provinces in China, 2019–2020.
-
With a large sample of 10,347 community-dwelling older adults in three provinces, this study identified that the prevalence rates of mild HL, moderate HL, and severe or profound HL were 47.2% (95% CI: 46.3%, 48.2%), 18.0% (95% CI: 17.3%, 18.8%), and 4.5% (95% CI: 4.1%, 4.9%), respectively. The prevalence of cognitive impairment was 19.1% (95% CI: 18.3%, 19.8%) overall and increased gradually with the severity of HL. Using normal hearing function as the reference group, the ORs for having cognitive impairment increased gradually with the severity of HL: 1.23 (1.08–1.40) for mild HL, 1.55 (1.32–1.82) for moderate HL, and 1.87 (1.47–2.39) for severe or profound HL. Hearing-related social isolation has been proposed to contribute to the association between HL and poorer cognitive function. The association between HL and cognitive impairment highlights the need to enhance public awareness of hearing protection, and it is crucial to minimize the adverse impact of HL on language and cognitive development.
This study shows that the prevalence of mild HL (47.2%) was higher than that reported in a 2014–2015 survey (34.8%), while the prevalence of moderate or higher grades of HL was 22.5%, slightly lower than that survey (24.1%) (1). This study found that the prevalence of moderate or higher grades of HL increased with age, rising from 12.8% at the age of 60–64 years to 52.4% at 80 years and above, consistent with global trends (7). Individuals with lower socioeconomic status, such as those living in rural areas, with fewer years of education, or who were widowed, were more likely to have moderate or severe HL. This disparity may reflect limited access to ear and hearing care resources and services among these populations (7). Consistent with other studies, we found that HL was associated with cognitive impairment (3). More specifically, this study found that any grade of HL was related to cognitive impairment, a finding somewhat different from a previous study that found only individuals with moderate or severe HL performed worse in cognitive assessments (8). This discrepancy may be due to differing criteria for HL grades and different cognitive function assessment scales. The association between HL and cognitive impairment remains unclear (3). HL may contribute to cognitive decline through impaired speech perception or a broader physiological decline, including vascular decline.
A cohort study suggested that hearing aids might prevent or delay dementia onset and progression (9). The WHO recommends hearing screening followed by prompt hearing aid provision for older adults, as this is associated with significant improvements in hearing-related health outcomes. Hearing function should be protected throughout the life course, as many causes of HL can be prevented through public health strategies and clinical interventions (7).
This study was subject to some limitations. First, the cross-sectional design precludes inferences about temporal associations between HL and cognitive impairment. Second, data from the three provinces are not nationally representative. Third, the time course of HL could not be determined for inclusion in the regression models, which may be associated with cognitive decline in older adults.
In conclusion, this study found that HL was prevalent among community-dwelling older adults and a possible modifiable risk factor for cognitive impairment. These findings suggest that enhancing public awareness of hearing protection is important for preventing cognitive impairment. Moreover, promoting HL screening and cognitive function assessment during elderly health examinations or primary care management is crucial for healthy aging.
-
No conflicts of interest.
-
All participants who took part in the project and doctors from collaborative hospitals, on-site work organization of primary medical and public health institution, supervision and guidance by all experts during the project implementation process.
HTML
| Citation: |

|