
 Download:
Download:




-
Fractures are a prevalent injury among children, with one-third experiencing at least one fracture before reaching adulthood (1). This may be attributed to rapid bone growth, active bone mineral deposition, or their generally active lifestyles (2). Fractures not only cause intense physical pain but can also lead to serious complications, including infections, joint stiffness, functional limitations, and even disability. Such outcomes can severely hinder a child’s physical development and quality of life, placing significant burdens on families and society. In response, the Chinese government has incorporated bone health initiatives into broader policies such as Healthy China 2030 (3). To effectively prevent fractures in children, it is crucial to understand their epidemiological patterns. Thus, this study explores the prevalence and common sites of fractures among children and adolescents aged 6–17 years in China.
This study utilizes survey data from the National Nutrition and Health Systematic Survey for Children aged 0–17 in China (2019–2021). It employed a multi-stage stratified random cluster sampling approach to conduct a cross-sectional survey across 28 urban and rural locations in 14 provincial-level administrative divisions (PLADs) spread over seven Chinese regions: East, North, Central, South, Southwest, Northwest, and Northeast China. In each survey site, data were collected from 12 age groups (6 to 17 years old), totaling 196 individuals per age group. Overall, 65,856 participants were initially recruited. Following the exclusion of respondents with missing data across various questionnaires, the final sample comprised 60,930 individuals. The methods for study design and sampling have been detailed previously (4). Informed consent was obtained from the guardians of all participants. The study received ethical approval from the Ethical Review Committee of the National Institute for Nutrition and Health, Chinese Center for Disease Control and Prevention (No. 2019-009).
Questionnaires were employed to gather data from participants, including basic demographic details (gender, age, and residential address) and fracture-related information. Participants were initially queried about any hospital-diagnosed fractures in their history. If the response was affirmative, additional information was requested concerning the age at and location of the most recent fracture. Parents assisted children aged 6–9 years in completing the questionnaire, while those aged 10–17 years filled it out independently. Age, a continuous variable, was reported as means with standard deviations (SD), and categorical variables, such as fractures, were reported as n (%). Fracture prevalence was calculated by dividing the number of fracture cases by the population size, and differences in indices were compared using the chi-square test. Compound annual growth rates (CAGR) for fractures were determined by the twelfth root (n=12) of the total growth rate percentage between ages 6 to 17 years. The Cochran-Armitage trend test was employed to assess trends in fracture prevalence across age groups. All statistical analyses were conducted using SAS (version 9.4, SAS Institute Inc., Cary, USA). A two-sided P<0.05 was considered statistically significant.
The average age of the subjects was 11.57±3.43 years. Table 1 outlines the participants’ general characteristics and the fracture prevalence across various demographics. The survey indicated that out of 4,222 children aged 6–17 years, there was a fracture history, giving a prevalence rate of 6.93%, with a higher incidence in males (8.13%) compared to females (5.71%, P<0.001). Geographic variations were also noted, with rural areas showing a higher fracture prevalence of 7.22% compared to 6.62% in urban areas (P<0.001). Regionally, fracture rates varied significantly (P<0.001), peaking at 9.40% in North China and dropping to a low of 4.79% in South China.
Characteristics N (%) All fracture sites Upper limbs Lower limbs Trunk Head Prevalence
[% (95% CI)]P Prevalence
[% (95% CI)]P Prevalence
[% (95% CI)]P Prevalence
[% (95% CI)]P Prevalence
[% (95% CI)]P Gender <0.001 <0.001 0.018 0.271 0.006 Male 30,700 (50.4) 8.13 (7.82, 8.44) 5.21 (4.96, 5.46) 2.30 (2.13, 2.46) 0.28 (0.22, 0.34) 0.15 (0.10, 0.19) Female 30,230 (49.6) 5.71 (5.45, 5.97) 3.26 (3.06, 3.46) 2.02 (1.86, 2.18) 0.23 (0.18, 0.29) 0.07 (0.04, 0.10) Age group (years) <0.001 <0.001 <0.001 0.599 0.716 6–8 15,590 (25.6) 3.52 (3.23, 3.80) 2.09 (1.87, 2.32) 0.99 (0.84, 1.15) 0.21 (0.14, 0.28) 0.09 (0.04, 0.14) 9–11 14,010 (23.0) 5.81 (5.42, 6.20) 3.34 (3.04, 3.64) 1.98 (1.75, 2.21) 0.25 (0.17, 0.33) 0.10 (0.05, 0.15) 12–14 15,773 (25.9) 8.01 (7.59, 8.44) 4.98 (4.64, 5.32) 2.47 (2.22, 2.71) 0.26 (0.18, 0.34) 0.12 (0.07, 0.17) 15–17 15,557 (25.5) 10.26 (9.78, 10.74) 6.47 (6.08, 6.85) 3.18 ( 2.90, 3.45) 0.31 (0.22, 0.40) 0.13 (0.07, 0.18) Area 0.004 0.053 0.009 0.076 0.004 Urban 29,845 (49.0) 6.62 (6.34, 6.91) 4.08 (3.86, 4.31) 2.00 (1.84, 2.16) 0.29 (0.23, 0.36) 0.07 (0.04, 0.10) Rural 31,085 (51.0) 7.22 (6.93, 7.51) 4.40 (4.17, 4.63) 2.31 (2.14, 2.48) 0.22 (0.17, 0.27) 0.15 (0.11, 0.19) Seven Major Regions <0.001 <0.001 <0.001 0.002 0.282 North 9,060 (14.9) 9.40 (8.80, 10.01) 5.66 (5.19, 6.14) 3.05 (2.69, 3.40) 0.36 (0.24, 0.49) 0.17 (0.08, 0.25) Northeast 8,986 (14.7) 5.07 (4.62, 5.53) 3.14 (2.78, 3.50) 1.40 (1.16, 1.65) 0.34 (0.22, 0.47) 0.08 (0.02, 0.14) East 8,956 (14.7) 8.14 (7.57, 8.71) 4.76 (4.32, 5.20) 2.81 (2.47, 3.16) 0.29 (0.18, 0.40) 0.09 (0.03, 0.15) Central 8,815 (14.5) 5.74 (5.25, 6.23) 3.55 (3.16, 3.94) 1.83 (1.55, 2.11) 0.12 (0.05, 0.20) 0.10 (0.04, 0.17) South 7,606 (12.5) 4.79 (4.31, 5.27) 3.12 (2.73, 3.51) 1.37 (1.11, 1.63) 0.13 (0.05, 0.21) 0.05 (0.00, 0.10) Southwest 8,772 (14.4) 9.03 (8.43, 9.63) 5.88 (5.39, 6.37) 2.49 (2.16, 2.81) 0.33 (0.21, 0.45) 0.15 (0.07, 0.23) Northwest 8,735 (14.3) 5.99 (5.49, 6.48) 3.41 (3.03, 3.79) 2.04 (1.74, 2.33) 0.19 (0.10, 0.29) 0.13 (0.05, 0.20) Total 60,930 (100.0) 6.93 (6.73, 7.13) 4.24 (4.08, 4.40) 2.16 (2.04, 2.27) 0.26 (0.22, 0.30) 0.11 (0.08, 0.14) Abbreviation: CI=confidence interval. Table 1. Prevalence of fractures among children and adolescents aged 6–17 years — China, 2019–2021.
The prevalence of fractures varies with age and gender, ranging from 3.18% in males aged 6 years to 13.38% in those aged 17 years, and from 2.86% in females aged 6 years to 8.07% in females aged 17 years (Figure 1). The smallest difference in fracture prevalence between genders was observed in the 9-year-old group (3.77% in males versus 3.55% in females, χ2=0.105, P=0.746), while the largest difference was in the 17-year-old group (13.38% in males versus 8.07% in females, χ2=35.134, P<0.001). The CAGR of fracture prevalence from ages 6 to 17 was 12.72% for males and 9.04% for females, with a significant overall growth trend observed in both genders (P<0.001).
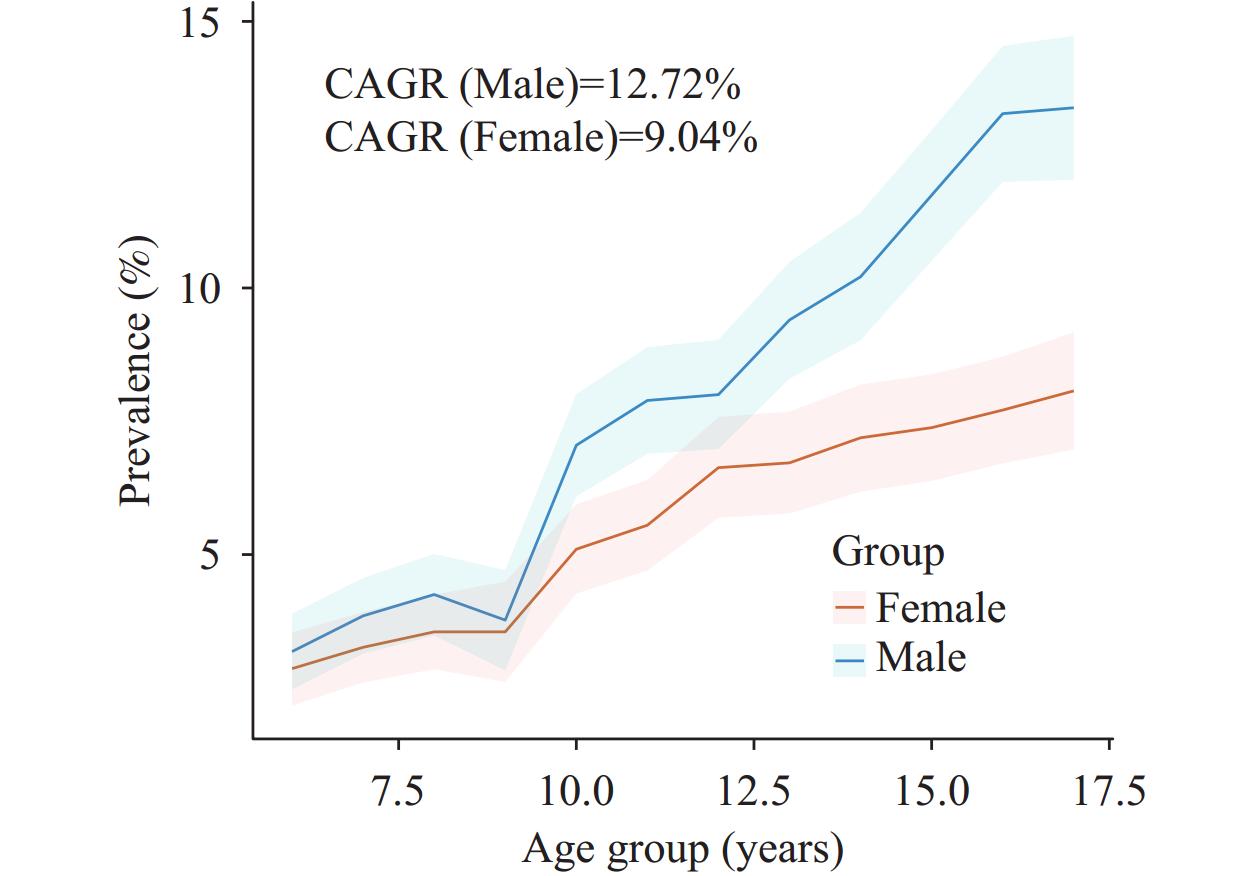 Figure 1.
Figure 1.Prevalence of fractures with 95% confidence intervals by age and gender among children and adolescents aged 6–17 years in China, 2019–2021.
Note: The compound annual growth rate (CAGR) was calculated as the twelfth root of the total fracture prevalence rate among 6–17 year olds. The Cochran-Armitage Trend Test yielded a P<0.001.Regarding different fracture sites, the prevalence rates for fractures in the upper limbs, lower limbs, trunk, and head were recorded at 4.24%, 2.16%, 0.26%, and 0.11%, respectively. The prevalence rates in males were higher than in females for upper limbs (5.21% vs. 3.26%, P<0.001), lower limbs (2.30% vs. 2.02%, P=0.018), and head (0.15% vs. 0.07%, P=0.006), but there was no significant difference in the prevalence of trunk fractures. There was a significant age-associated increase in prevalence for both upper and lower limb fractures (P<0.001). Geographically, the prevalence of fractures in the lower limbs and head was higher in rural areas compared to urban areas (2.31% vs. 2.00% and 0.15% vs. 0.07%, respectively, P<0.05). Additionally, there were regional differences in the prevalence rates of fractures in the upper limbs, lower limbs, and trunk across seven regions (P<0.001).
In a study of 4,222 children with a history of fractures, the majority involved the upper limbs, accounting for 65.9% of males and 58.9% of females (Figure 2). Fractures of the lower limbs were reported in 28.6% of males and 35.6% of females. Fractures involving the trunk and head were less common, comprising less than 5% of fractures in both genders. Similar distributions were observed across different gender and age subgroups, as detailed in
Supplementary Figure S1 . The incidence of fractures in both the upper and lower limbs initially increased with age, peaking at around 10 years old at 7.1% for upper limbs in males and 6.89% in females, and at 3.12% for lower limbs in males and 4.29% in females, before subsequently declining.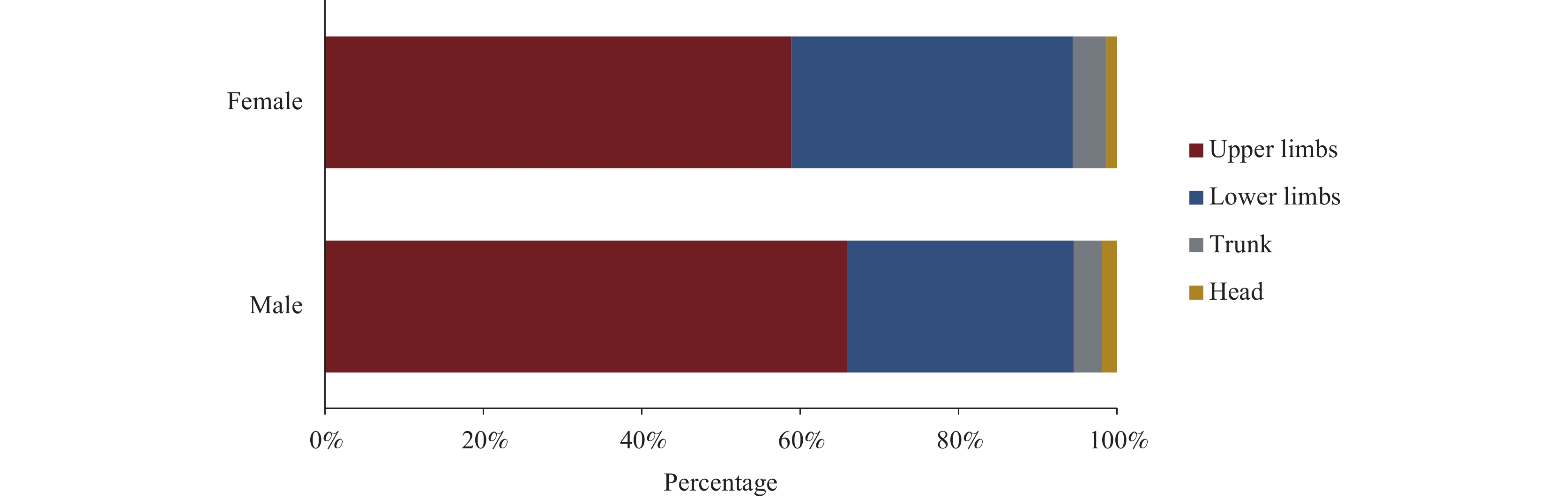 Figure 2.
Figure 2.Composition of the percentage of different fracture sites by gender in children and adolescents.
-
This cross-sectional study provides nationally and regionally representative data on the prevalence of fractures among Chinese children and adolescents aged 6–17 years. The observed prevalence of fractures in this demographic was 6.93%, which is significantly higher than the rate in Chinese adults aged 25–34 years (2.05 per 1,000 people) (5). This indicates that children and adolescents constitute a high-risk group for fractures, presenting substantial public health challenges. Furthermore, the prevalence of fractures among children varies by ethnicity. Over recent decades, numerous studies have investigated the epidemiology of childhood fractures in various regions, including Scandinavia and the United Kingdom (UK). In our study, the fracture rate was lower compared to white children in the UK (14%, N=10,856) and comparable to non-white children (8.1%, N=1,711) aged 0–14 years from a population-based household survey in the UK (6). Moreover, the China national fracture study in 2014 (N=512,187) reported a fracture incidence of 3.21 per 1,000 people across all ages, also lower than that observed among white populations (5). The ethnic disparities in fracture prevalence among children could be attributed to genetic factors, differences in bone mineral densities, or dietary variations. Additionally, lower engagement in high-risk activities among Chinese children may explain some of the ethnic differences (6).
Childhood fractures exhibit significant variations by gender and age. Males consistently experience a higher incidence of fractures across all age groups and regions, aligning with findings from prior research (5,7). Notably, this disparity widens beginning at the age of nine. This trend may be attributed to male children typically engaging in more vigorous and high-risk physical activities, thus increasing their susceptibility to fractures. Furthermore, our data indicate that fractures are most prevalent among males aged 10–13 and females aged 10–12. This pattern is supported by a comprehensive survey conducted in Beijing, which also identified the highest fracture incidence within the same age range for males (7). The differences in fracture rates among age groups likely reflect the stages of skeletal development, with fractures occurring most frequently during adolescence — a period characterized by rapid changes in bone mineral density, geometry, and microarchitecture (8). Additionally, the higher bone elasticity in younger children and greater bone strength in older children contribute to lower fracture prevalences in these age groups.
Childhood fractures demonstrate notable regional disparities in China, with a higher incidence in rural areas compared to urban areas (7.22% vs. 6.62%). In economically disadvantaged rural regions, the prevalence of such injuries can be attributed to children’s vulnerability to unbalanced diets or nutrient deficiencies that potentially compromise bone health (9). Additionally, a significant number of children in rural areas, often left unsupervised due to their parents’ absence, face an increased risk of accidental injuries or fractures (10). This study is the first to elucidate regional variations in childhood fractures across seven major regions. Further research is warranted to investigate the factors influencing childhood fractures in different regions.
The prevalence of childhood fractures varies significantly across different anatomical sites. Over half of all fractures occur in the upper limbs, with a notably higher incidence in males (66%). A cohort study in Beijing revealed that fractures of the upper limb comprise approximately 65.9%–73.3% of fractures among children aged 6–16 years (7). Accelerated remodeling of the metaphysis in the forearms of children can lead to a temporary reduction in bone mass, thereby increasing the risk of fractures. Additionally, the frequent use of upper limbs in sports activities and their critical role in self-protection during unintentional injuries contribute to the higher prevalence of fractures in upper limbs.
This study was subject to some limitations. First, the age at which fractures occurred was determined based on questionnaire responses, which may introduce recall bias. Second, the cross-sectional nature of this study precludes the calculation of fracture incidence; therefore, future cohort studies are advised.
In conclusion, childhood fractures represent a significant public health issue in China. Greater emphasis should be placed on children from rural areas and males in middle childhood. There is a need to enhance bone safety education for both children and their guardians to raise awareness about fracture prevention. Additional research is necessary to investigate potential factors influencing fractures among community children.
-
No conflicts of interest.
-
We extend our gratitude to the project teams at the China CDC, provincial CDCs, county/district CDCs, local school staff, and all participants.
HTML
| Citation: |

|