
 Download:
Download:




-
Infectious disease outbreaks, particularly emerging infectious diseases (EID), have significantly impacted global health over the last several decades. Notably, the 2003 severe acute respiratory syndrome (SARS/SARS-CoV-1) epidemic impacted 26 countries, resulting in over 8,000 cases and approximately 774 deaths, reflecting a case fatality rate of around 9.6% (1). The 2009 pandemic influenza A H1N1 affected more than 214 countries, with over 18,449 recorded fatalities worldwide (2). More recently, the coronavirus disease 2019 (COVID-19) pandemic has caused approximately seven million deaths globally (3) and has had extensive social, economic, and political ramifications, continuing to affect nearly every facet of life worldwide (4). In response to the ever-changing infectious disease landscape, there is a critical need to enhance our surveillance and early warning approaches. Current early warning systems (EWS) for EID often depend on a limited range of data sources, primarily healthcare facilities, and are hindered by delays in disease detection due to the reliance on clinical diagnosis data, which may be inadequate for timely infectious disease surveillance.
Over the past two decades, China has confronted several outbreaks of EID, such as SARS-CoV-1 (5), highly pathogenic avian influenza A(H5N1) (6), A(H5N6) (7), A(H7N9) (8), a human Streptococcus suis outbreak in Sichuan Province (9), and COVID-19 (10). In response, China has bolstered its capacity for early detection and response through an integrated approach, which includes enhancements in systems like the Infectious Disease Automated-Alert and Response System (CIDARS) (11). Furthermore, the establishment of the Public Health Emergency Response Information System (PHERIS) (12) and syndromic surveillance mechanisms has strengthened its EWS infrastructure. In contrast, Australia utilizes the National Notifiable Disease Surveillance System (NNDSS) and augments it with hospital-based syndromic surveillance, which monitors notifiable pathogens and lays the groundwork for more advanced national surveillance and EWS. Recognizing the critical importance of rapid response and preparedness for infectious disease outbreaks, both China and Australia, as prominent players in public health within the Asia-Pacific region, have acknowledged the need for a cooperative infectious disease EWS network. The geographical positioning of China in the Northern Hemisphere and Australia in the Southern Hemisphere offers a unique opportunity to establish an inter-hemispheric EWS focused on seasonal influenza. The Research Network of EWS for Infectious Diseases between China and Australia (NetEWAC) was inaugurated in August 2023, supported by a grant from the Australian Department of Foreign Affairs and Trade (DFAT). This collaborative effort is designed to enhance early outbreak detection, facilitate data sharing, and strengthen regional health security.
This article offers a detailed overview of the current state of EWS and introduces a concept for developing an integrated NetEWAC. As key players in the Asia-Pacific region, the establishment of this collaborative network is projected to be mutually beneficial, enhancing not only national but also regional and global health security. Through such bilateral partnerships, there is potential for expansion and to serve as models for broader regional collaboration, thus strengthening collective responses to health emergencies.
-
EWS are essential for the early detection of infectious diseases that exceed predefined thresholds, providing alerts to health authorities before a significant increase in cases. EWS incorporate various surveillance approaches that differ depending on the specific diseases or symptoms monitored and the effectiveness of the systems or indicators, enabling rapid detection of small case clusters before they escalate and burden healthcare systems (13). In several high- or middle-income countries, EWS have been implemented based on national notifiable infectious disease surveillance systems, including China’s CIDARS (11), Norway’s national web-based outbreak rapid alert system (Vesuv) (14), and Sweden’s Computer Supported Outbreak Detection System (CASE) (15). In contrast, syndromic surveillance-based EWS focuses on identifying non-specific symptoms at the initial stages of illness, which allows for the identification of illness clusters before formal diagnoses are confirmed and reported to public health authorities (16). Such systems are not only crucial but also extensively utilized in various nations. Prominent examples include the USA’s Early Aberration Reporting System (EARS) (17) and the Electronic Surveillance System for the Early Notification of Community-Based Epidemics (ESSENCE) (18-19); the United Kingdom’s Emergency Department Sentinel Syndromic Surveillance System (EDSSS) (20) and the National Health Service (NHS) Direct Syndromic Surveillance (21); and Australia’s Public Health Real-Time Emergency Department Surveillance System (PHREDSS) (22). Additionally, other EWS configurations compile real-time data from diverse sources, such as laboratory tests, over-the-counter (OTC) drug sales, emergency call volumes, ambulance dispatches, and patient attendance records at primary care facilities (13).
To address the escalating risk of infectious disease epidemics worldwide, the World Health Organization (WHO) initiated the Global Outbreak Alert and Response Network (GOARN) in 2000. This collaborative network comprises institutions and international organizations concerted in providing a swift and effective response to outbreaks wherever they occur. Since its establishment, GOARN has played a pivotal role in managing major outbreaks such as SARS, Ebola, H5N1, and the 2009 H1N1 pandemic (23). Additionally, in 2004, WHO launched the Early Warning Alert and Response Network (EWARN) to aid low-income countries in promptly identifying and managing infectious disease outbreaks during humanitarian emergencies. EWARN has been deployed in countries including South Sudan, Haiti, Somalia, Congo, Mozambique, Syria, Iraq, and the Philippines (24). It notably detected the reemergence of wild poliovirus in Somalia in 2013 (25). However, EWARN serves as a temporary measure during crises, not as a replacement for permanent national surveillance systems. Once the humanitarian crisis concludes, the notification activities revert to routine surveillance, limiting outbreak detection capabilities outside of emergencies where robust surveillance systems might be absent (24). Furthermore, the WHO Global Influenza Surveillance and Response System (GISRS) gathers global data to enhance data sharing and integration, crucial for early detection and preparedness against influenza outbreaks (26). Nonetheless, disparities exist in the early warning capabilities and coverage across GISRS-participating countries, indicating that regional networks like NetEWAC could enhance global surveillance efforts by bolstering local capacities and fostering regional cooperation in infectious disease early warning.
In the domain of digital surveillance, platforms such as Google Flu Trends (GFT) (27) initially emerged as pioneering, web-based systems for the real-time tracking of influenza-like illnesses (ILI). Though GFT highlighted the potential of utilizing search engine data for disease surveillance, it was ultimately phased out due to issues related to its accuracy and reliability. This highlights the critical need for ongoing evaluation of the effectiveness and limitations of such digital tools in public health surveillance (28). Complementary to these platforms, HealthMap distinguishes itself as an impactful digital instrument within global health monitoring. By consolidating data from varied sources including news reports, eyewitness accounts, and official records, HealthMap delivers real-time insights on a broad spectrum of health threats, including infectious diseases and drug resistance. This system has been instrumental in the real-time tracking of disease dissemination, enhancing early detection and intervention during health crises (29). The integration of HealthMap into the global health surveillance framework enhances the capabilities of conventional systems such as GOARN, EWARN, and GISRS, thereby improving overall early warning and response mechanisms for infectious disease threats. For a detailed review of EWS established in various countries and by international organizations, refer to Table 1.
EWS name Geographical scope Data source Disease or syndromes Strengths Limitations CIDARS (11) China NIDRIS 28 infectious diseases notifiable to NIDRIS CIDARS uses real-time reporting information via the Internet, enhancing the timeliness and completeness of data reporting; it employs three aberration detection methods to detect unusual occurrences of 28 notifiable infectious diseases; nationwide implementation, involving all levels of CDCs in China, facilitates early outbreak detection and prompt reporting across the country CIDARS relies on notifiable infectious disease surveillance data, which may be less timely and sensitive compared to other outbreak detection systems using pre-diagnosis data or media reports; generation of negative signals, causing unnecessary signal response work for local staff; maintaining normal operations of the system and managing over 6,000 users pose significant challenges. PHREDSS (30) Australia/NSW ED Notifiable infectious diseases Real-time data analysis, early warning system, enhance the overall surveillance capabilities Limited to ED visits, integration and data sharing with other health surveillance systems can be challenging FluTracking (31) Australia Community-Based Surveillance ILI Community reporting; real-time data on ILI trends; cost-effective compared to traditional surveillance methods; wide geographical coverage and public engagement Reliance on self-reported data, lack of detailed clinical information; potential participant bias; dependent on internet access ESSENCE (19) USA MTFs from over 300 military installations worldwide Communicable diseases ESSENCE demonstrates high accuracy in data representation, particularly in gastrointestinal diseases, which have the highest overall sensitivity (89%) and specificity (96%); the military system provides near-complete data coverage of outpatient visits, which is advantageous for public health surveillance The sensitivity for respiratory diseases was lower (65.7%) compared to gastrointestinal diseases; the quality of data depends on the accuracy of ICD-9 coding EARS (17) USA Public health surveillance data Deliberately emerging infectious diseases EARS includes various aberration detection methods, providing flexibility and options for different surveillance needs; it allows local and state health departments to modify sensitivity and specificity thresholds according to their public health importance; and providing flexibility and options for different surveillance needs in various data sources, enhancing its applicability The effectiveness of EARS depends on the quality and reliability of the input data; challenges in differentiating false alarms, leading to potential over-investigation; complexity in operation and cost and resource-intensive requirements ARTSSN (32) Canada/Alberta Province Electronic Health Record (e.g., Health Link calls, ED visits, school absenteeism, laboratory tests) Communicable and non-communicable diseases ARTSSN analyses multiple electronic data sources concurrently in real-time, delivers timely, comprehensive, and automated surveillance; capable of monitoring a wide range of health conditions, including infectious and chronic diseases, injuries, and environmental hazards Dependence on data source stability, interpreting signals from multiple data streams and understanding free-text medical records remain complex tasks EDSSS (20) UK ED Pre-defined Syndromic indicators Timely detection of public health threats, comprehensive data collection, real-time surveillance, and can be adapted to focus on specific health conditions or syndromes. Dependence on data quality, integration with other health surveillance systems, and limited to ED data. NHS Direct (21) UK National Telephone Health Advice Helpline 10 common syndromes Unique data sources outside of traditional clinical settings, capturing health concerns that might not result in hospital or GP visits; accessible to a large proportion of the population. The reliance on self-reported symptoms could lead to variability in data quality and challenges in interpretation; limited clinical validation, and integration with other health surveillance systems. SARI-surveillance (33) Germany Private hospital network SARI Provides prompt and reliable information on SARI in patients in Germany; explores different diagnosis groups and classes (admission or discharge; primary or secondary); high sensitivity with Sensitive Case Definition (SCD), which includes not only patients with primary discharge from J09 -J22 but also cases with any secondary discharge diagnosis from J09-J22 Lack of complementary virological information; discharge data lagged the information from primary care sentinel surveillance, leading to delayed availability of data SurSaUD (34) France All-cause mortality data Mortality variations The system records 77.5% of the total number of deaths, the extensive coverage ensures effective monitoring of expected and unusual mortality outbreaks; high sensitivity and specificity Lack of medical causes of death limits the ability to target recommendations and determine the specific contributions of events like influenza epidemics and heatwaves to overall mortality Vesuv (14) Norway MSIS Infectious diseases notifiable to MSIS Vesuv allows information included in each notification to be modified and updated as the outbreak investigation progresses, which is practical for users conducting outbreak investigations; Vesuv is an event-based reporting system Awareness and training needs; cannot quantitatively assess its timeliness, as the date of identification of the outbreak is missing. CASE (15) Sweden SmiNet (national notifiable disease database) Communicable diseases CASE is adaptable to different contexts, enhancing its usefulness in various settings; CASE uses emails for notifications, presenting information in a familiar format without requiring users to learn a new interface, simplifying the communication process; allowing users to select statistical methods best suited to the characteristics of a specific disease; this flexibility enables more accurate detection and analysis of disease outbreaks The effectiveness of the system is highly dependent on the quality and completeness of the data from SmiNet. ICARES (35) Netherlands GP, and hospital records Clusters of infectious diseases ICARES can detect differences in the incidence of various disease groups in real-time, within a 24-window; capable of making historical comparisons specific to each healthcare provider and adjusting baseline values for seasonal variations in disease incidence ICARES faces challenges in measuring sensitivity due to imperfections in coding for non-specific syndromes and a limited number of participating healthcare facilities, resulting in both false positive and false negative alerts GPSURV (36) New Zealand GP electronic clinical records Three acute infectious disease syndromes Effectively monitors acute infectious disease syndromes like gastroenteritis, influenza-like illness, and skin infections; adaptive denominator definition ensures a more accurate representation of the patient population Complexity in denominator population definition; GPSURV’s focus on record completion and data capture, rather than diagnostic reliability, raised questions about the system’s data quality ProMed-mail (37) Global Media reports, official reports, online summaries, local observers, and others Emerging infectious diseases and toxins Global reach: ProMED-mail disseminates information to over 30,000 people in more than 180 countries, indicating its wide reach and influence and diverse information sources, including media reports, official reports, online summaries, and observations The postings on ProMED-mail are often drawn from general media sources and lack scientific language, which can affect their credibility among professionals; a large volume of postings originate from doubtful sources, dependence on confirmation from other sources Google Flu Trends (27)* Global Web search queries related to flu Influenza Wide reach, it gathers and analyzes healthcare-seeking behavior in the form of online search queries, reflecting a global user base; usefulness in developed countries; correlation with traditional data Data inaccuracies and sampling issues; the lack of standardized search criteria means different users may enter symptoms differently, affecting the accuracy and consistency of data GOARN (23) Global Member States, EIOS, EBS, disease-specific networks, network of collaborating institutions, direct reports from the field, and other International organizations (e.g., FAO, and OIE) Infectious disease and emerging infections Global collaboration, rapid response capability, expertise and experience, information sharing, capacity building, and research and development Resource limitations, political and bureaucratic challenges, variability in health systems, data quality, and sharing issues. GISRS (38) Global Influenza surveillance data from NICs, WHO H5 Reference laboratories, ERLs and WHO regional databases Respiratory viruses, including Influenza Existing global and regional networks for surveillance of circulating and emerging strains of respiratory viruses, including influenza; robust laboratory network Varying capacities of NICs; limited geographical coverage; inadequate human and veterinary surveillance; workforce constraints; poor intersectoral coordination; and funding constraints HealthMap (29) Global News reports, eyewitness accounts, and official records a wide range of health threats, such as infectious diseases and drug resistance Multistream real-time surveillance; extensive data collection; global reach and language expansion; automated system for data organization; wide usage by government agencies Dealing with unstructured and unorganized internet data; difficulty in differentiating between distinct types of reports; focus on conspicuous but low-impact events; time-consuming for users FluNet (39) Global Influenza virological surveillance data (NICs of the GISRS) Influenza Facilitating the collection and sharing influenza surveillance data from NICs of the GISRS and other national influenza reference laboratories collaborating actively with GISRS across the globe; providing near real-time data on influenza virus strains circulating worldwide; allowing for the analysis of global and regional trends in influenza activities Quality and timeliness of data depend on the participating countries’ surveillance capacities; underrepresentation of some regions in developing countries; not covering other respiratory viruses or emerging pathogens EPIWATCH (40) Global Open-source data Infectious disease and emerging infections Real-time or near-real-time monitoring; data integration from various sources; early warning capability; customizable alerts based on specific diseases or geographical areas of interest Effectiveness depends on the quality and reliability of the data fed into it; a limited scope, focusing on specific diseases or regions; potential false alarms or overreport, leading to unnecessary responses Abbreviation: CIDARS=China infectious disease automated-alert and response system; NIDRIS=national notifiable infectious diseases reporting information system; PHREDSS=the NSW public health real-time emergency department surveillance system; NSW=New South Wales; ED=emergency departments; ILI=influenza-like illness; ESSNCE=electronic surveillance system for theearly notification of communicable-based epidemics; USA=United States of America; MTFs=military treatment facilities; EARS=early aberration reporting system; ARTSSN=the alberta real time syndromic surveillance; EDSSS=emergency department sentinel syndromic surveillance system; UK=United Kingdom; NHS=national health service; SARI=severe acute respiratory infections surveillance system; SurSaUD=reactive mortality surveillance system-syndromic surveillance system; Vesuv=national web-based outbreak rapid alert system; MSIS=norwegian surveillance system for communicable diseases; CASE=computer supported outbreak detection system; SmiNet=internet-based surveillance system for communicable diseases; ICARES=integrated crisis alert and response system; GP=general practitioner; GPSURV=electronic general-practitioner-based syndromic surveillance system; SID-SSS=school-based syndromic surveillance system; GOARN=global outbreak alert and response network; EIOS=epidemic intelligence from open sources; EBS=event-based surveillance; FAO=food and agriculture organization; OIE=world organization for animal health; GISRS=WHO global influenza surveillance and response system; NICs=national influenza centers; ERLs=WHO essential regulatory laboratories.
* Google Flu Trends stopped publishing current estimates on August 9, 2015.Table 1. Overview of early warning systems for infectious disease outbreaks.
-
Following the 2003 SARS epidemic, the Chinese government initiated a series of enhancements to the National Notifiable Infectious Diseases Reporting Information System (NIDRIS) (41) to bolster infectious disease surveillance capabilities. Although NIDRIS significantly improved the reporting timeliness for notifiable infectious diseases, its capacity for early outbreak detection remained limited. In response, in 2004, China launched the PHERIS, a web-based, event-based system designed to gather data on a variety of public health events, including infectious disease outbreaks, 57 clusters of diseases of unknown cause, extensive food or occupational poisonings, and other significant public health events (12). This system expanded the surveillance scope beyond that provided by NIDRIS. In 2008, China introduced the CIDARS (42), an EWS operating nationally that builds on the existing NIDRIS data concerning 28 notifiable diseases prone to outbreaks, thus enhancing early detection capabilities. CIDARS performs real-time and daily data analysis based on four key elements: aberration detection, signal creation, signal distribution, and feedback on signal responses (Figure 1). It automatically identifies data anomalies reported through NIDRIS and swiftly issues alert to the corresponding county-level CDC via Short Message Service (SMS). Moreover, CDCs at national, provincial, and prefecture levels coordinate the response to each signal, providing expertise and facilitative support to ensure efficient information exchange and coordinated response efforts to prevent disease spread (11). Evaluations of the system have demonstrated CIDARS’s effectiveness in generating timely and specific warning signals, with evidence from 2009 to 2012 showing successful detection of all 30 dengue fever outbreaks during the period (43). Its efficacy in identifying hand, foot, and mouth disease outbreaks in China has also been validated (44). However, CIDARS’s dependence on the data from diagnosed and reported cases within NIDRIS can impede its ability to detect outbreaks before these cases are clinically identified. Challenges such as reporting delays and underreporting may result in delayed or missed warnings, particularly with EID (11).
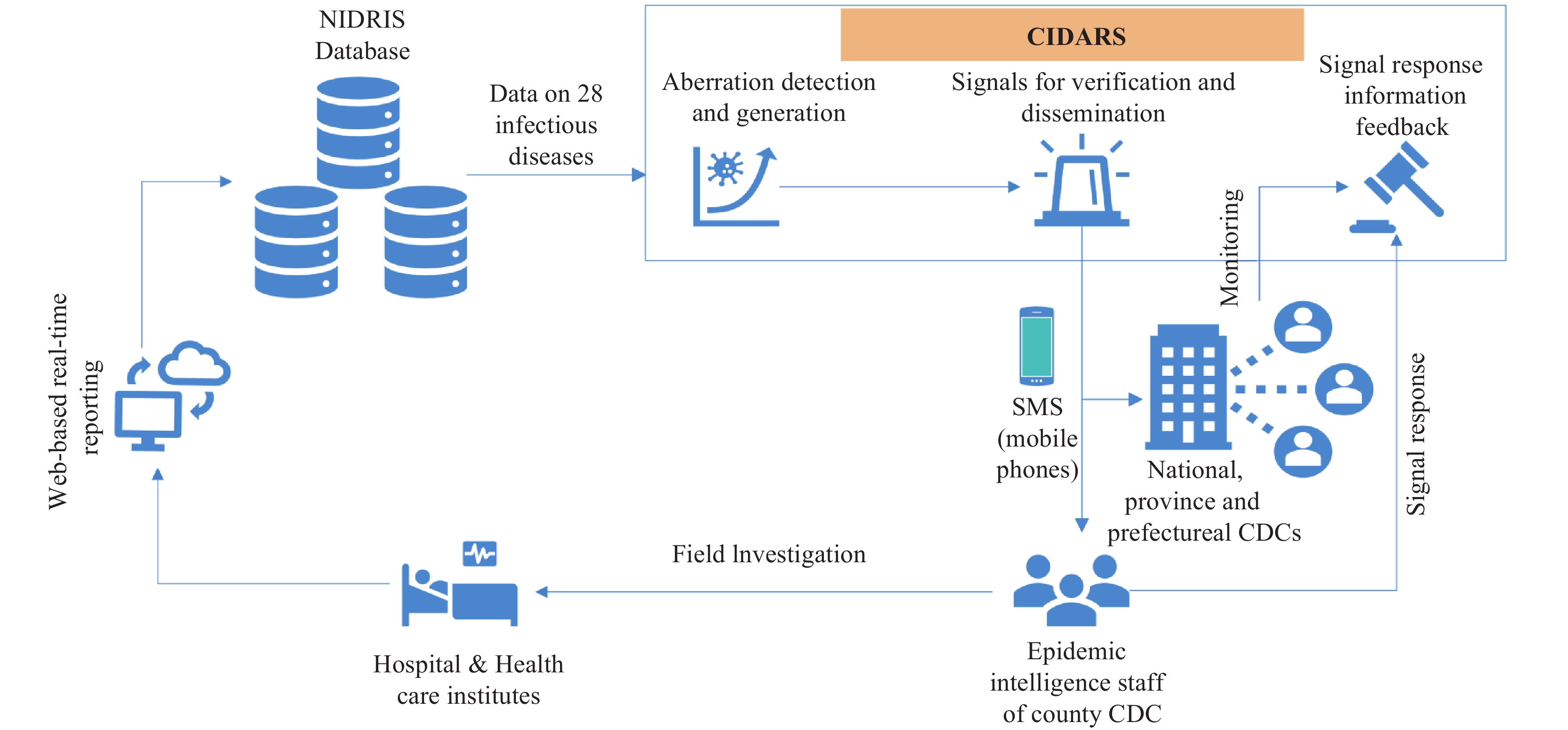 Figure 1.
Figure 1.Flow diagram of the CIDARS.
Abbreviation: CIDARS=China infectious diseases automated alert and response system; SMS=short message service; NIDRIS=national notifiable infectious diseases reporting system.Syndromic surveillance-based EWS in China are primarily employed for monitoring influenza epidemics (45). Within this EWS framework, the pneumonia of unknown etiology (PUE) surveillance system, established after the SARS outbreak in 2004, is integral for tracking novel respiratory pathogens, including avian influenza and SARS (46). From 2005 to 2013, the PUE system was instrumental in detecting 23 of the 43 cases of avian influenza A (H5N1) in Chinese mainland (46). Notably, as part of the comprehensive EWS, the PUE system also identified the first four cases of novel coronavirus (2019-nCoV)-infected pneumonia (NCIP) in Wuhan on December 29, 2019 (47). However, the PUE system encounters challenges such as significant underreporting, which impairs its overall effectiveness (48). After the 2008 Sichuan earthquake, mobile phones equipped with infectious disease reporting software were distributed to local healthcare providers, enhancing early detection and response capabilities for infectious disease outbreaks (49). Additionally, China CDC has implemented media surveillance to identify infectious disease outbreaks. This system gathers information from three key sources: searches for public health-related keywords using Baidu’s search engine (50), global health platforms including WHO GOARN, GPHIN, ProMED, and CIDRAP, and reports from domestic public health institutes. An automated monitoring system screens this information daily, compiling a list of relevant public health events. These events are then assessed by a specialized team who initiates a comprehensive procedure of in-depth follow-up, verification, and tailored response for each identified health concern (51).
Several early warning and detection methods, including the Pudong Syndromic Surveillance and Early Warning System (PD-SEWS) (52), “Xiao Lian Xing” (XLX), an app-based sentinel syndromic surveillance system (SSS) utilizing school absenteeism data (53), OTC drug sales, hospital and school-based ILI data, Baidu search queries (54), and the Integrated Surveillance System for infectious diseases in rural China project (ISSC) (55), have proven to be effective in the early detection of outbreaks (13). These methods are crucial components of an integrated infectious disease surveillance and EWS. In China, efforts are increasing to enhance the integration and connectivity of various infectious disease surveillance systems. Such initiatives aim to develop a comprehensive platform that combines multi-channel surveillance data, including mandatory case reporting, syndromic surveillance, causes of deaths, and laboratory reports, with multi-point triggers such as OTC drug sales, internet search queries, school absenteeism, social media, and news reports. The objective is to build a robust, interconnected surveillance network and EWS for infectious diseases. While this approach is promising, it requires significant ongoing development (56).
In contrast, Australia’s NNDSS, established in 1991, mandates that healthcare providers and laboratories report case data to state or territory health authorities. These authorities, in turn, transmit de-identified data to a national database (57). Although the NNDSS is a highly valued resource for infectious disease control and prevention in Australia (58), the recent global spread of infectious diseases, particularly highlighted by the COVID-19 pandemic, has emphasized the necessity for more effective and precise surveillance systems (59). While Australia has not adopted a comprehensive national surveillance and EWS for infectious diseases akin to CIDARS (11), it has developed sophisticated syndromic surveillance systems. These systems have evolved over the years to incorporate data from varied sources such as hospitals, emergency departments, general practitioners, laboratories, and communities. By monitoring symptoms and health-related data across these platforms, the system plays a pivotal role in the early detection of outbreaks prior to laboratory confirmation, thereby enabling swift responses. Notably, during the 2009 H1N1 influenza pandemic, this system was instrumental in tracking viral spread, assessing case severity, and informing vaccination strategies (60). This approach could serve as a blueprint for surveillance of emerging infections and EWS development within the country.
-
The primary goal of the NetEWAC initiative is to improve seasonal influenza surveillance and EWS. By capitalizing on the unique seasonality of influenza in different countries with asynchronous influenza seasons, the program aims to enhance the accuracy of predictive models and the effectiveness of intervention strategies. The network will concentrate on analyzing influenza trends, peak activities, and potential inter-hemispheric transmission patterns, with customizations to specifically tackle the challenges associated with seasonal influenza. This strategy could potentially be adapted for the surveillance, prediction, and management of other infectious diseases.
In China, the seasonality of influenza varies significantly due to its extensive geographical size, diverse climate zones, and population distribution. In the northern regions, similar to other temperate zones, influenza typically peaks during the winter months, with epidemics occurring from December to February. Conversely, southern China, which features a subtropical to tropical climate, experiences two influenza peaks: a primary peak in winter and a secondary, smaller peak in summer. Additionally, influenza may circulate year-round in these southern regions (61). Factors such as absolute humidity, minimum temperature, rainfall, and ultraviolet light contribute to the seasonality of influenza (61–62). Moreover, urban areas, which have denser populations and more frequent person-to-person interactions, often exhibit distinct influenza trends compared to rural settings (63).
In Australia, the influenza season generally commences in May or June, reaching its peak during the winter months. However, in tropical and subtropical areas, influenza cases may be present throughout the year, typically increasing during the cooler or rainier months. The timing and severity of influenza seasons vary annually, influenced by factors such as the strains of circulating viruses, population immunity levels, and travel patterns. Notably, due to the COVID-19 pandemic and resultant travel restrictions, there was a significant reduction in influenza activity from March 2020 to October 2021. Influenza activity resumed in Victoria, Australia (64), in November 2021, with an escalation leading to a major outbreak by May 2022 (65). Additionally, non-seasonal spikes can emerge, particularly during pandemics, such as during the 2009 H1N1 pandemic (66-67). The influenza seasonality in Australia generally occurs about five to six months behind China’s primary influenza season, owing to the opposing seasons in the Northern and Southern Hemispheres (Figure 2).
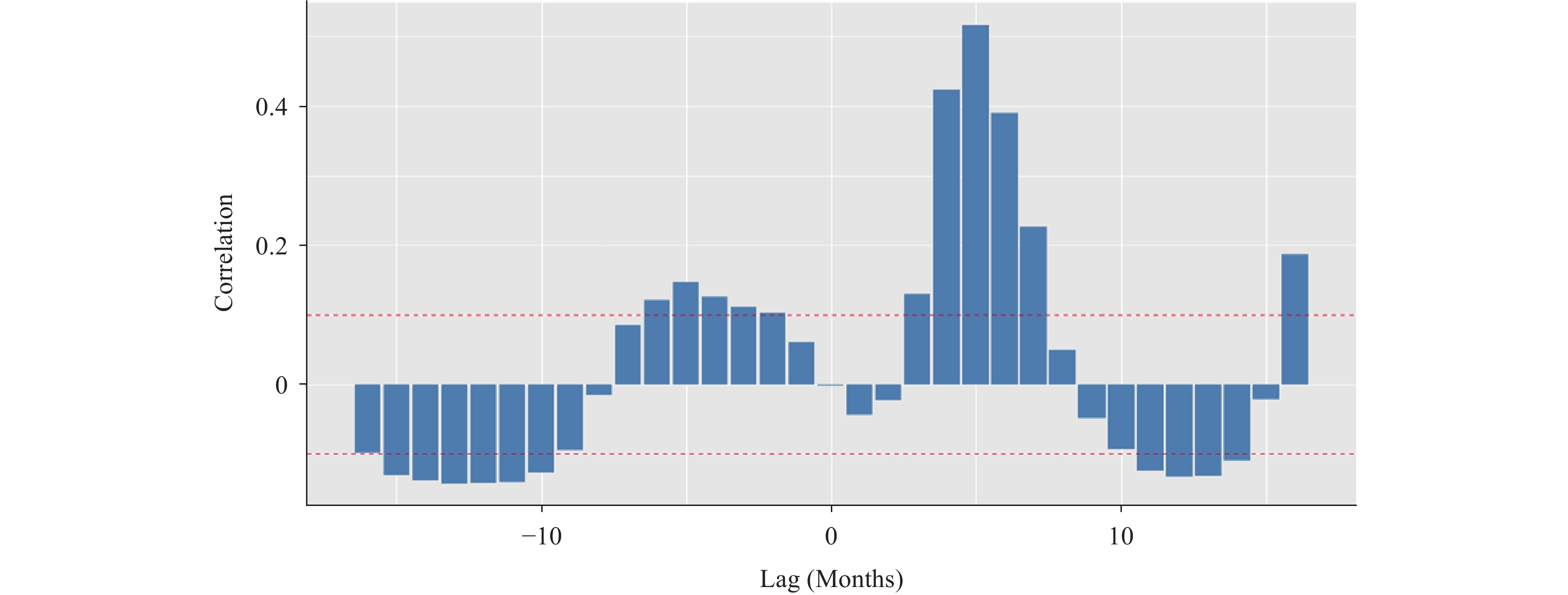 Figure 2.
Figure 2.Cross-correlation of influenza epidemics between China and Australia.
Note: This figure illustrates the correlation between influenza incidence rates in China and Australia over time. Negative lag values indicate that China’s influenza season precedes that of Australia, while positive lag values suggest the opposite. The bars represent correlation coefficients for various time lags, and the horizontal red lines indicate the confidence interval range of [−0.1, 0.1]. Bars crossing these lines denote a significant correlation. The strongest correlation occurs when Australia’s influenza season lags 4 to 5 months behind China’s, indicating a pattern where China’s influenza season can help predict the subsequent season in Australia.Influenza surveillance is critical for tracking and addressing seasonal epidemics and emergent strains. Both China and Australia have robust influenza surveillance systems, though they vary in size, coverage, and methodologies for data gathering. In China, surveillance relies on a network of healthcare facilities with mandatory reporting for both clinically diagnosed and laboratory-confirmed cases through the China National Influenza Surveillance Network (NISN). The NISN, which includes 554 sentinel hospitals and 410 laboratories, collects data pertaining to ILI and severe acute respiratory infections (SARI). This surveillance network plays a pivotal role in identifying novel influenza strains and detecting the onset of epidemics (68) (Figure 3).
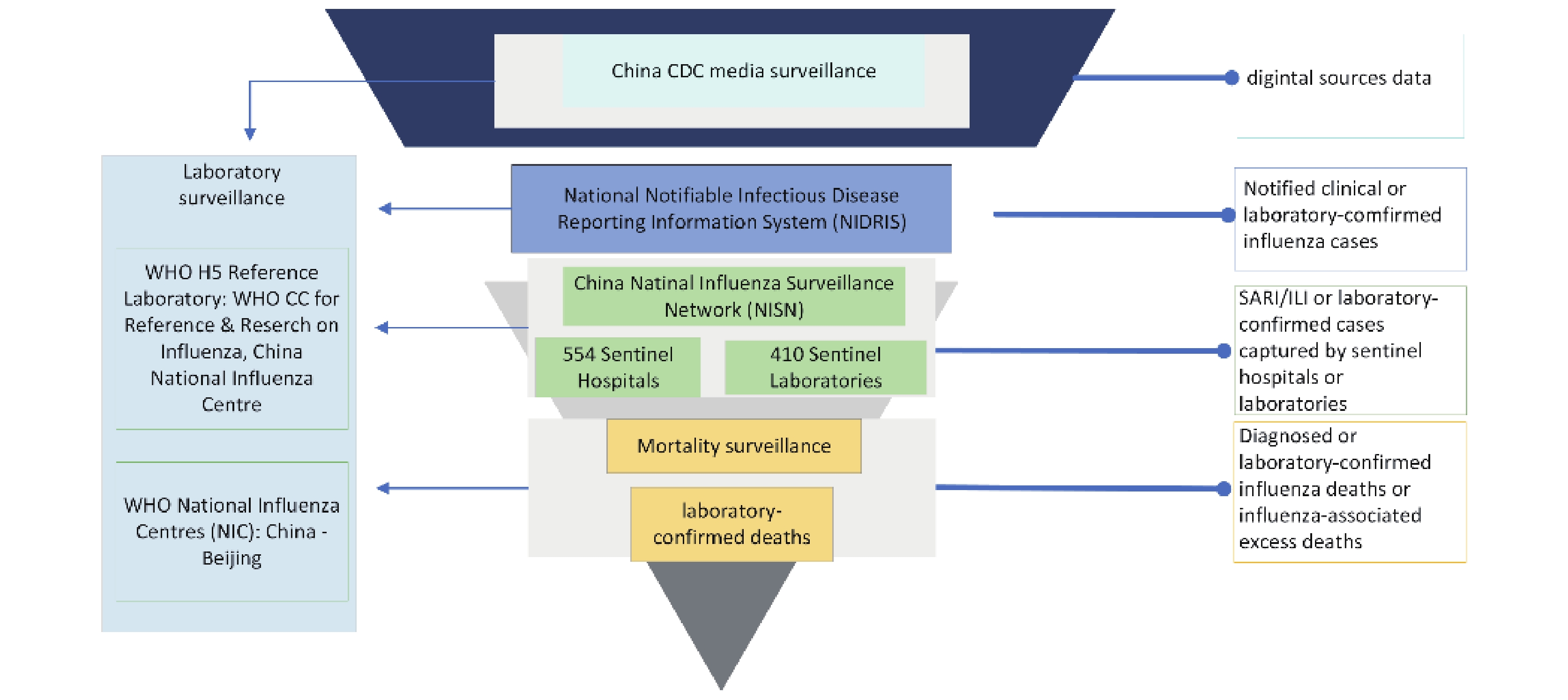 Figure 3.
Figure 3.Influenza surveillance system in China.
Abbreviation: SARI=severe acute respiratory infections; ILI=influenza-like illness; WHO CC=World Health Organization collaboration centers.Australia’s National Influenza Surveillance Scheme, established in 1994, collects both syndromic and laboratory-confirmed influenza cases via multiple channels including hospitals, general practitioners, community reporting, and mortality records (69). This scheme integrates data from various surveillance systems into the Australian Influenza Surveillance Report (AISR) during the flu season (65). In addition to mandatory reporting of laboratory-verified cases through the NNDSS, the initiative employs numerous data sources for comprehensive influenza surveillance data collection. Sentinel surveillance systems such as general practice (GP)-based ILI sentinel surveillance [e.g., the Australian Sentinel Practices Research Network (ASPREN)], emergency department (ED) surveillance systems for influenza, and hospital-based systems [e.g., the Influenza Complications Alert Network (FluCAN) and the Australian Pediatric Surveillance Unit (APSU)] are utilized. Together with a network of sentinel laboratories, they provide robust, near real-time medically attended data on ILI and virology, thus offering an in-depth view of influenza activity (70). Additionally, non-medically attended community-reported SARI or ILI cases as well as healthcare-seeking behaviors are directly captured from the public via web-based platforms such as FluTracking (31) and Healthdirect. Surveillance of influenza-related mortality further illuminates the severity of each season (71) (Figure 4).
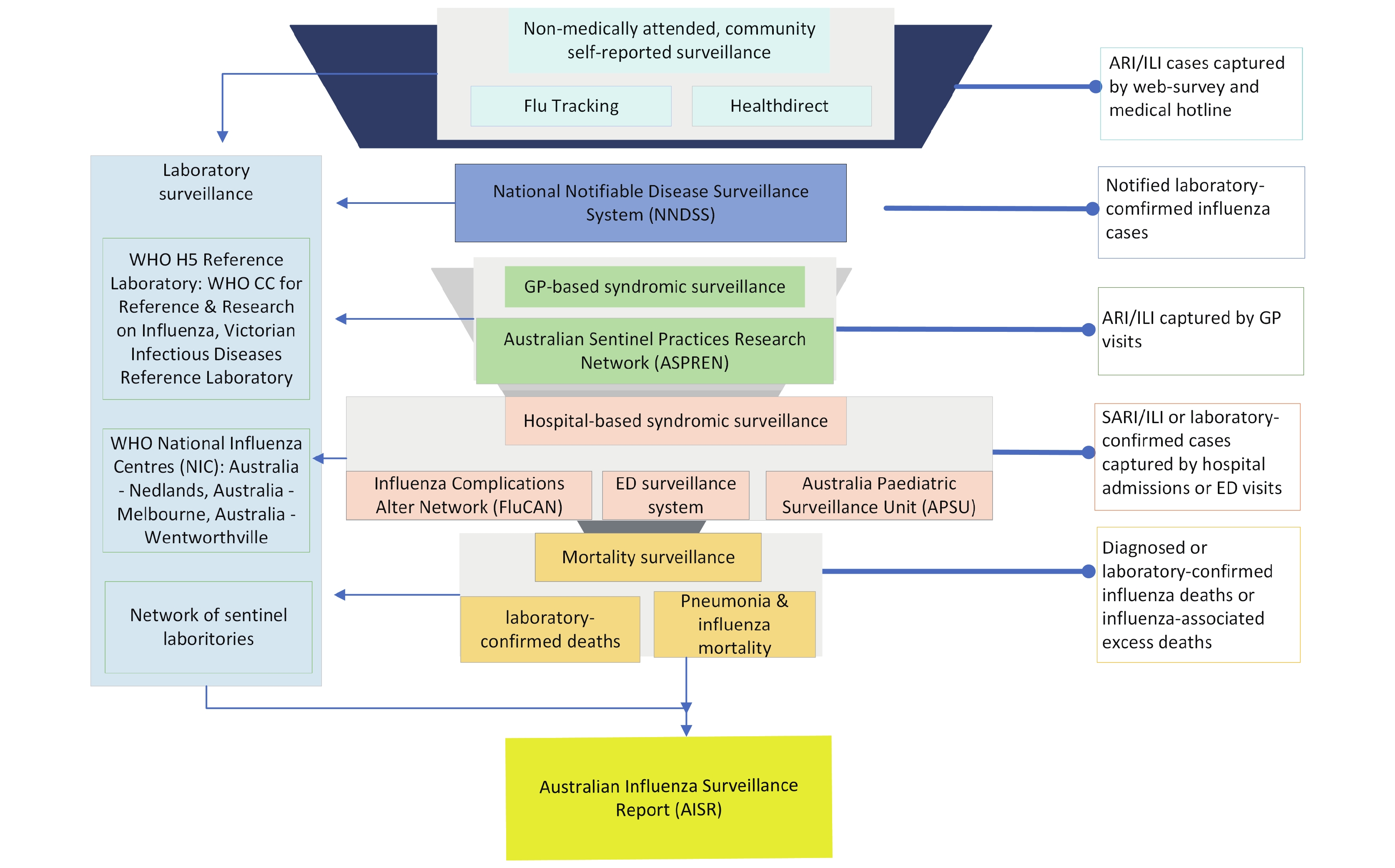 Figure 4.
Figure 4.Influenza surveillance system in Australia.
Abbreviation: ARI=acute respiratory illness; ILI=influenza-like illness; GP=general practitioner; GP-based=general practice-based; WHO CC=World Health Organization collaboration centers; ED=emergency department.While China and Australia employ divergent influenza surveillance strategies, cooperation between the two countries is possible due to their different geographical positions and climatic conditions, which lead to asynchronous influenza seasons. Analysis of data from each hemisphere demonstrates distinct seasonal patterns and varied peak periods. Concurrent outbreaks indicate potential cross-hemispheric transmission. By integrating cross-hemispheric data, this collaboration can enhance comparative analyses, thereby improving predictive models and intervention strategies.
-
China and Australia, located in the northern and southern hemispheres, respectively, experience distinct climatic conditions and population dynamics, leading to asynchronous influenza seasons and differing virus transmission patterns. Analyzing data from each hemisphere separately uncovers unique infection trends and variable influenza season peaks. Although typically these hemispheres suffer influenza outbreaks at different times, the occurrence of simultaneous epidemics implies the possibility of cross-hemispheric transmission. Integrating data from both hemispheres allows for comprehensive comparative analyses, which can elucidate trends, seasonal peaks, and inter-hemispheric transmission mechanisms (72-73). Previous research has demonstrated significant correlations between seasonal influenza outbreaks in countries such as the United States, Australia, and Chile (74); Argentina and South Korea (75). This facilitates more timely and accurate predictions of seasonal trends and the formulation of effective preventive measures (74-75). Furthermore, utilizing complementary influenza patterns from both hemispheres enhances the robustness of predictive models by incorporating broader seasonal dynamics. One study showed that combining data from both hemispheres markedly increased the accuracy of models, especially in predicting the timing of influenza outbreaks (73). Additionally, incorporating environmental factors like climate from both hemispheres has been shown to improve these models further (76). These findings underscore the importance of cross-hemispheric data integration in refining influenza prediction and highlight its implications for both national and global influenza surveillance and preparedness. By examining inter-hemispheric transmission patterns, NetEWAC can leverage the asynchronous influenza seasons between China and Australia to develop more accurate predictive models and devise effective intervention strategies.
Based on the components of the ongoing research network for an EWS between China and Australia, we recommend the following actions. 1) Establish data-sharing agreements: develop agreements with relevant institutions to access specific datasets from both countries. These agreements should define the terms of data use to ensure compliance with the legal frameworks of both nations. 2) Develop standardized data formats and terminologies: Create standardized formats and terminology to facilitate the integration and analysis of cross-national datasets. 3) Protect sensitive information: emphasizing aggregated and de-identified information data to protect sensitive information while enhancing early warning and surveillance. 4) Enhance surveillance capabilities: improve surveillance system in both nations to gather real-time, multi-source (77), historical, and cross-hemispheric surveillance data, along with other pertinent socio-environmental factors. 5) Develop robust spatiotemporal predictive models: Create predictive models to forecast influenza epidemics using socio-environmental factors, historical and ongoing surveillance data. 6) Translate findings into policy: Ensure that research findings are translated into actionable policy recommendations to support effective early warning and response strategies.
The creation of the collaborative NetEWAC network has substantial implications for global cooperation in the surveillance of EIDs. This initiative provides a blueprint for effective partnership among countries with varying healthcare systems, resources, and levels of experience. Successful regional collaborations naturally lead to an expansion of the network, bringing more countries in the Western Pacific Region into the fold. Such expansion not only broadens the network’s geographic reach but also amplifies its surveillance capabilities. Moreover, these regional partnerships lay the groundwork for wider international collaborations and networks.
The effectiveness of NetEWAC depends on its specialized strategy for monitoring seasonal influenza. The advantages of this collaboration are a better comprehension of influenza patterns across hemispheres, improved accuracy in predicting the timing of outbreaks, and the facilitation of more efficient public health interventions. Nevertheless, obstacles like data standardization, privacy issues, and the harmonization of various surveillance approaches need to be overcome. The network’ goal is to create a strong framework for data exchange and analysis, concentrating on the specific dynamics of seasonal influenza in both China and Australia.
-
In conclusion, the creation of NetEWAC marks a substantial advancement in targeted seasonal influenza surveillance and EWS. This collaborative effort between China and Australia concentrates on influenza and promises to significantly improve the understanding and management of this consequential disease. Given their status as major players in the WHO Western Pacific region, the knowledge derived from this collaborative effort could establish a model for similar initiatives, which might expand to include more comprehensive regional cooperation in infectious disease surveillance. While the primary emphasis is on influenza, the techniques and insights obtained from NetEWAC may also enhance approaches to other infectious diseases, thereby bolstering regional and global health security.
-
No conflicts of interest.
HTML
A Review of Existing EWS
Infectious Diseases Surveillance in China and Australia
Feasibility, Benefits, and Challenges of NetEWAC
| Citation: |

|