
 Download:
Download:




-
Hepatitis B, an infectious disease caused by the hepatitis B virus (HBV), is preventable through vaccination. In 1992, the recombinant hepatitis B vaccine (HepB) was recommended for routine immunization of infants, starting at birth. HepB was incorporated into the Expanded Program on Immunization (EPI) in 2002, and patient copayments for its administration were removed in 2005, enhancing its accessibility and affordability (1). By 2021, the prevalence of HBV infection had significantly declined due to comprehensive prevention and control measures centered around HepB vaccination (2). According to the World Health Organization (WHO) criteria, China has transitioned from high to intermediate endemicity since 2006 (3). Nonetheless, HBV prevalence remains regionally variable within China, exhibiting areas of high, intermediate, and low endemicity. Although previous studies in China have documented the epidemiological characteristics and trends of acute hepatitis B (AHB) (4), analyses of long-term trends and age-period-cohort effects are lacking. This study aims to provide an updated and comprehensive overview of AHB epidemiology in China, evaluate the effects of age, period, and cohort on AHB incidence, and offer evidence to inform strategies for achieving China’s hepatitis elimination goals.
-
This study obtained AHB reports from the National Notifiable Disease Reporting System (NNDRS) in China spanning 2005 to 2021. Based on HBsAg prevalence among individuals aged 1–59 years from a 1992 viral hepatitis seroepidemiological survey, this study’s researchers classified the 31 provincial-level administrative divisions (PLADs) in China into low (<7%), intermediate (7%–11%), and high (>11%) endemic areas. The low endemic areas include Beijing, Hebei, Guizhou, Tianjin, Inner Mongolia, Shanxi, Jiangsu, Yunnan, and Xinjiang PLADs. The intermediate endemic areas are Shanghai, Shandong, Hunan, Anhui, Gansu, Qinghai, Jilin, Shaanxi, Sichuan, Chongqing, Heilongjiang, and Zhejiang PLADs, while the high endemic areas encompass Hubei, Henan, Ningxia, Liaoning, Guangxi, Jiangxi, Fujian, Xizang, Hainan, and Guangdong PLADs. AHB cases were categorized into 18 age groups: 0–4, 5–9, 10–14, 15–19, ..., 80–84, and ≥85 years old. The study period was segmented into three distinct phases: 2005–2010 (post-full HepB introduction into EPI), 2011–2015 (post-nationwide childhood HepB catch-up campaign), and 2016–2021 (post-nationwide expansion of the iPMTCT program). With consideration of age group and period (Cohort=Period−Age), we calculated 20 corresponding 5-year birth cohorts (1921–2915, 1926–1930, 1931–1935, …, 2016–2020). Male-to-female ratios for subgroups were determined using population data from the 2000, 2010, and 2020 China Population Census Yearbooks.
-
Joinpoint regression was utilized to analyze trend data, with the Monte Carlo permutation test identifying the number, location, and P values of joinpoints. Annual percentage change (APC) and average APC (AAPC) were calculated based on endemic area, gender, and age subgroup. Age, period, and cohort effects, as well as rate ratios, were estimated using an age-period-cohort model. Statistical analyses were conducted using Joinpoint software (version 5.0.2, Statistical Research and Applications Branch, National Cancer Institute, Bethesda, USA) and age-period-cohort analysis web tool (National Cancer Institute, Bethesd USA).
-
Table 1 presents the incidences of AHB and their percentage changes by endemicity area, age group, and time period. From 2005 to 2010: In the 0–14 age group, the annual average reported AHB incidences per 100,000 population were 1.65, 2.33, and 2.56 in low, intermediate, and high endemic areas, respectively. In the ≥15 age group, the incidences were 6.26, 7.68, and 11.73, respectively. From 2011 to 2015: In the 0–14 age group, incidences were 0.62, 0.72, and 0.94, reflecting decreases of 62.42%, 69.10%, and 63.28% from the previous period in low, intermediate, and high endemic areas, respectively. In the ≥15 age group, incidences were 4.04, 5.36, and 9.45, with decreases of 35.46%, 30.21%, and 19.44%. From 2016 to 2021: In the 0–14 age group, average incidences were 0.56, 0.58, and 0.48, showing decreases of 66.06%, 75.11%, and 81.25% compared to 2005–2010 in low, intermediate, and high endemic areas, respectively. In the ≥15 age group, incidences were 3.61, 3.86, and 5.49, representing decreases of 42.33%, 49.74%, and 53.20%. AHB incidence was highest in high endemic areas and lowest in low endemic areas, but the annual average incidences varied by endemic area, gender, and age group. The corresponding results are provided in
Supplementary Table S1 .Categories Low endemicity Intermediate endemicity High endemicity Incidence rate (95% CI)
(1/100,000)Percent
change (%)Incidence rate (95% CI)
(1/100,000)Percent
change (%)Incidence rate (95% CI)
(1/100,000)Percent
change (%)0–14 age group 2005–2010 1.65 (1.61, 1.69) Reference 2.33 (2.29, 2.37) Reference 2.56 (2.52, 2.60) Reference 2011–2015 0.62 (0.59, 0.65) −62.42 0.72 (0.69, 0.75) −69.10 0.94 (0.91, 0.97) −63.28 2016–2021 0.56 (0.54, 0.58) −66.06 0.58 (0.56, 0.60) −75.11 0.48 (0.46, 0.50) −81.25 ≥15 age group 2005–2010 6.26 (6.22, 6.30) Reference 7.68 (7.65, 7.71) Reference 11.73 (11.68, 11.78) Reference 2011–2015 4.04 (4.01, 4.07) −35.46 5.36 (5.33, 5.39) −30.21 9.45 (9.41, 9.49) −19.44 2016–2021 3.61 (3.58, 3.64) −42.33 3.86 (3.84, 3.88) −49.74 5.49 (5.46, 5.52) −53.20 Total 2005–2010 5.37 (5.34, 5.40) Reference 6.72 (6.69, 6.75) Reference 9.87 (9.83, 9.91) Reference 2011–2015 3.47 (3.44, 3.50) −35.38 4.64 (4.61, 4.67) −30.95 7.93 (7.89, 7.97) −19.66 2016–2021 3.09 (3.07, 3.11) −42.46 3.34 (3.32, 3.36) −50.30 4.58 (4.55, 4.61) −53.60 Note: 2005–2010: after full HepB introduction into EPI; 2011–2015: after the nationwide childhood HepB catch-up campaign; 2016–2021: after integrated prevention of mother-to-child transmission of HIV, syphilis, and hepatitis B (iPMTCT) program expanded nationwide.
Abbreviation: AHB=acute hepatitis B; CI=confidence interval; EPI=Expanded Program on Immunization; HepB=hepatitis B vaccine; HIV= human immunodeficiency virus.Table 1. Annual average reported incidence of AHB and changes by endemic area and age group, 2005–2021, China.
-
The 15–39-year age group in high endemic areas exhibited the most significant decline in incidence, dropping from 23.14 per 100,000 in 2005 to 4.59 per 100,000 in 2021 among males, and from 10.62 per 100,000 to 3.21 per 100,000 among females (Table 2). The incidence of reported AHB among males aged 15–39 in low endemic areas decreased significantly between 2005 and 2012 (APC=−13.45%, P<0.05). However, the decrease was less pronounced between 2012 and 2021 (APC=−2.64%, P>0.05). In intermediate endemic areas from 2005 to 2021, consistent decreases were observed among both males (APC=−9.74%, P<0.05) and females (APC=−7.76%, P<0.05). In high endemic areas, a slight decrease was noted among males between 2005 and 2012 (APC=−5.57%, P<0.05) and among females between 2005 and 2014 (APC=−3.45%, P<0.05). This was followed by a marked decrease among males from 2012 to 2021 (APC=−13.30%, P<0.05) and among females between 2005 and 2014 (APC=−12.80%, P<0.05). Trends varied by age group and endemic area (Table 2, Figure 1).
Age (years) Gender Incidence rate (1/100,000) Total study period Trend 1 Trend 2 Trend 3 Trend 4 2005 2021 AAPC (%) 95% CI Years APC (%) Years APC (%) Years APC (%) Years APC (%) Low endemicity Total 5.96 3.07 −4.78* (−6.38, −3.02) 2005–2012 −9.86* 2012–2021 −0.63 0−14 Male 2.53 0.43 −12.58* (−15.66, −9.50) 2005–2012 −20.56* 2012–2018 2.90 2018–2021 −21.11* Female 1.35 0.36 −9.31* (−12.24, −6.36) 2005–2013 −17.56 2013–2016 18.38 2016–2021 −9.97 15−39 Male 11.88 4.23 −7.53* (−8.96, −5.94) 2005–2012 −13.45* 2012–2021 −2.64 Female 6.16 3.26 −4.97* (−7.35, −2.43) 2005–2021 −4.97* ≥40 Male 6.56 4.62 −2.49* (−3.94, −0.85) 2005–2012 −6.79* 2012–2021 0.99 Female 2.43 2.58 −0.35 (−2.47, 1.90) 2005–2021 −0.35 Intermediate endemicity Total 8.04 2.55 −6.30* (−7.60, −4.93) 2005–2021 −6.30* 0−14 Male 4.67 0.50 −12.95* (−15.16, −10.25) 2005–2011 −24.83* 2011–2021 −4.94 Female 2.63 0.38 −11.01* (−12.59, −9.24) 2005–2011 −23.67* 2011–2021 −2.43 15−39 Male 15.82 3.25 −9.74* (−10.81, −8.62) 2005–2021 −9.74* Female 7.94 2.08 −7.76* (−8.94, −6.52) 2005–2021 −7.76* ≥40 Male 8.07 4.01 −4.33* (−5.38, −3.37) 2005–2018 −1.91* 2018–2021 −14.16* Female 3.37 2.28 −2.49* (−4.05, −1.10) 2005–2018 0.09 2018–2021 −12.92* High endemicity Total 10.42 3.23 −7.45* (−8.12, −6.79) 2005–2015 −4.36* 2015–2021 −12.38* 0−14 Male 4.63 0.29 −16.82* (−18.13, −15.65) 2005–2011 −19.12* 2011–2019 −11.62* 2019–2021 −29.00* Female 2.25 0.22 −13.43* (−14.40, −12.48) 2005–2007 −8.34 2007–2011 −21.07* 2011–2016 −3.63 2016–2021 −18.16* 15−39 Male 23.14 4.59 −10.00* (−10.56, −9.39) 2005–2012 −5.57* 2012–2021 −13.30* Female 10.62 3.21 −7.66* (−8.48, −6.82) 2005–2014 −3.45* 2014–2021 −12.80* ≥40 Male 9.98 5.27 −4.04* (−4.91, −3.19) 2005–2015 0.08 2015–2021 −10.53* Female 3.53 2.67 −1.88* (−2.69, −1.05) 2005–2015 2.75* 2015–2021 −9.14* Abbreviation: AHB=acute hepatitis B; APC=annual percent change; AAPC=average annual percent change; CI=confidence interval.
* P<0.05.Table 2. Trends in AHB incidence across various time segments identified through joinpoint analysis by endemic areas, age groups, and gender, 2005–2021, China.
 Figure 1.
Figure 1.Joinpoint analysis of AHB incidence in low, intermediate, and high endemic areas of China from 2005 to 2021. (A) Trends of AHB incidence in low endemic areas. (B) Trends of AHB incidence in intermediate endemic areas. (C) Trends of AHB incidence in high endemic areas.
Abbreviation: HepB=hepatitis B vaccine; AHB=acute hepatitis B; iPMTCT=integrated prevention of mother-to-child transmission of HIV, syphilis, and hepatitis B; HIV=human immunodeficiency virus. -
The impact of age on AHB incidence was consistent across low, intermediate, and high endemic areas. Incidence rates significantly decreased from the 0–4 age group to the 10–14 age group, peaked in the 15–19 age group, and then declined in the older age groups (Figure 2).
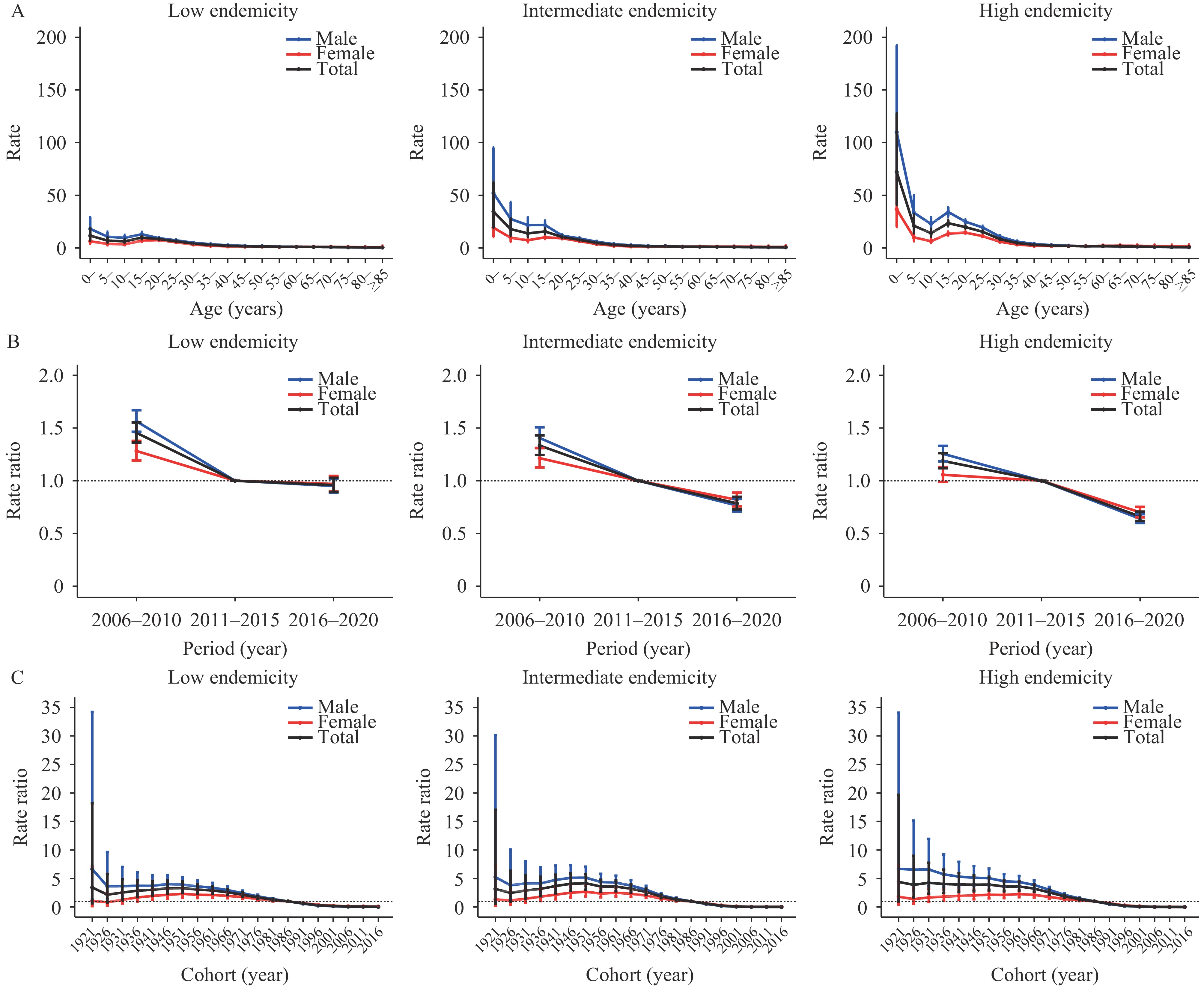 Figure 2.
Figure 2.Age, period, and cohort effects on AHB incidence in low, intermediate, and high endemic areas of China from 2006 to 2020. (A) Age effects on AHB incidence in low, intermediate, and high endemic areas. (B) Period effects on AHB incidence in low, intermediate, and high endemic areas. (C) Cohort effects on AHB incidence in low, intermediate, and high endemic areas.
Abbreviation: AHB=acute hepatitis B.Period effects demonstrated declines in AHB risk for both males and females across all endemic areas from 2006 to 2020. The highest risk was observed during the period 2006–2010. Using 2011–2015 as the reference period, the overall relative risk (RR) in low, intermediate, and high endemic areas was 1.45 (95% CI: 1.36, 1.55), 1.33 (95% CI: 1.24, 1.43), and 1.19 (95% CI: 1.12, 1.26), respectively. The period 2016–2020 exhibited the lowest risk, with RR values of 0.95 (95% CI: 0.89, 1.03), 0.79 (95% CI: 0.73, 0.85), and 0.66 (95% CI: 0.62, 0.71) for low, intermediate, and high endemic areas, respectively (Figure 2).
In high-endemic areas, a consistent decline in the cohort effect was observed among males. In contrast, in low and intermediate endemic areas, the cohort effect decreased rapidly between 1921 and 1926, slightly increased in the cohort born between 1926 and 1951, and then continued to decline (Figure 2).
-
This study revealed that the incidence of reported AHB was highest among individuals aged 15–39 years in 2005, similar to patterns observed in the early period in the United States (5). This age group experienced the largest decline in incidence, particularly males in high endemic areas, from 23.14 per 100,000 in 2005 to 4.59 per 100,000 in 2021 and among females from 10.62 per 100,000 to 3.21 per 100,000. Additionally, this study’s findings indicated a rapid decrease in AHB incidence among 15–39-year-olds following the introduction of a plasma-derived HepB vaccine in China in 1985. Among children under 15 years old in low, intermediate, and high endemic areas, the incidence dropped from 1.65, 2.33, and 2.56 per 100,000 in 2005–2010 to 0.56, 0.58, and 0.48 per 100,000 in the 2016–2021 period, reflecting the success of China’s EPI, which included HepB in 2002. Although the incidence decline among individuals over 40 years old was smaller, China has made significant strides in controlling AHB. Analysis of long-term trends in AHB incidence showed that low endemic areas experienced rapid declines in the early stages and gradual declines later on, whereas intermediate endemic areas had consistent downward trends. High endemic areas experienced slow declines initially and more rapid declines in later stages, likely influenced by HepB vaccination coverage and regional variations in hepatitis B endemicity.
-
Age is a crucial factor influencing AHB incidence. Historically, the predominant mode of HBV transmission in China has been mother-to-child transmission (6). This study’s findings indicate that the age effect peaks in the 0–4-year-old group, likely due to the high infection risk from mother-to-child transmission, weakened passive immunity, and lowered resistance to HBV in this age group. The age effect diminishes in the 5–14-year-old group, aligning with Liu et al.’s study on hepatitis B incidence in children aged 0–10 years (7). In the 15–19-year-old group, a slight increase in the age effect may be attributed to declining hepatitis B antibody levels and increased social activity-related infection risk. Factors influencing hepatitis B infection in this demographic warrant further investigation. In adults, the age effect decreases and stabilizes in individuals aged 45 years and older, possibly due to established immunity.
-
This study observed decreasing period effects across all endemic areas, indicating that enhanced immunization strategies and comprehensive prevention and control measures have been pivotal in reducing the reported incidence of AHB in China. The HepB vaccine has been provided free of charge to children in China since 2002. Moreover, from 2009 to 2011, China conducted a HepB catch-up campaign targeting children under 15 years of age born between 1994 and 2001 (4). In 2010, China became the first country to propose the integrated prevention of mother-to-child transmission of HIV, syphilis, and hepatitis B (iPMTCT) Program, which expanded nationwide by 2015 (8). These significant measures likely contribute to the sustained downward trend in period effects. Additionally, the AHB surveillance pilot project, which began in 2013, selected 200 counties as surveillance sites. This project aimed to improve the accuracy of AHB reporting in the NNDRS by standardizing diagnostic procedures and promoting IgM anti-HBc testing to differentiate between AHB and chronic hepatitis B flare-ups (4). This initiative has also played a role in the decline in AHB incidence.
-
This study observed declining cohort effects across all endemic areas, indicating that younger birth cohorts have a lower risk of AHB. This trend aligns with the implementation of comprehensive hepatitis B prevention and control measures, such as increased hospital delivery rates and enhanced HepB vaccination coverage for newborns. However, there was a slight rise in cohort effects in those born between 1951 and 1955, warranting further investigation.
The strengths of this study include utilizing national surveillance data from the NNDRS spanning 2005–2021, which ensures consistency in methodology and offers a comprehensive depiction of nationwide incidence trends. Additionally, it analyzed incidence trends and age-period-cohort effects by endemic area, age group, and gender, providing robust evidence of successful hepatitis B control practices in China.
However, the study was subject to some limitations, primarily due to variations in the diagnosis of AHB in NNDRS. Previous studies indicated that flare-ups of chronic hepatitis B were often misreported as AHB (9-10). Consequently, the reported AHB incidence in NNDRS is likely higher than the actual incidence. Furthermore, the observation period was relatively short, including only case data since 2005.
In conclusion, this study assessed the incidence of AHB from 2005 to 2021, revealing a decrease across all age groups and endemic areas. Notably, the reported incidence of AHB in children aged 14 years and below has dropped to low levels. However, the incidence remains higher in individuals aged 15 years and above compared to younger populations. To further reduce AHB incidence among adolescents and adults, it is crucial to enhance HepB vaccination rates in these age groups. Additionally, maintaining high vaccination coverage, conducting comprehensive HBV screening, administering antiviral agents to pregnant mothers, and ensuring a low AHB incidence rate are vital strategies for eliminating HBV transmission.
-
No conflicts of interest.
-
Dr. Lance Rodewald from the Chinese Center for Disease Control and Prevention for his comments and English language editing.
HTML
Data Sources
Statistical Analysis
AHB Incidence by Endemic Area, Age, and Gender
Trends in AHB Incidence
Age-period-cohort Model Results
Age Effect
Period Effect
Cohort Effect
| Citation: |

|