

 Download:
Download:




-
The World Health Organization (WHO) defines multimorbidity as the coexistence of two or more chronic diseases in an individual (1). In China, the prevalence of multimorbidity among older adults is approximately 50%, with resulting disabilities and cognitive impairments posing a significant threat to their health (2). As the number of chronic diseases continues to increase, the patient’s physical function gradually declines, and the risk of activities of daily living (ADL) disability increases (3). While previous studies using traditional statistical methods have identified combinatorial patterns and influencing factors of multimorbidity, they often fail to explain the dynamic relationship between multimorbidity and disability during the aging process (4). This study addresses this gap by using data from the China Health and Retirement Longitudinal Study (CHARLS) to construct a multi-state Markov model (MSM). This model explores the risk ratio and transition probabilities between ADL independence, disability, and death in adults aged 60 years and older in China, estimating both life expectancy (LE) and disability-free life expectancy (DFLE) with and without multimorbidity. Our findings indicate that multimorbidity significantly increases the risk of disability and reduces both LE and DFLE in older adults. This study provides a comprehensive assessment of the dynamic impact of multimorbidity on the functional status and mortality risk of older Chinese adults, offering valuable insights to policymakers developing targeted health interventions.
Data were drawn from five waves of the CHARLS collected between 2011 and 2020. The study sample included adults aged 60 years and older at baseline with complete information on ADL, chronic conditions, and mortality during the follow-up. Sample size and composition for each wave are presented in Table 1. CHARLS ascertained chronic disease information through respondent self-report, including hypertension, dyslipidemia, diabetes, cancer, chronic lung disease, liver disease, heart disease, stroke, kidney disease, stomach or other digestive disease, emotional, nervous, or psychiatric problems, memory-related disease, arthritis or rheumatism, and asthma. Multimorbidity was defined as having at least two chronic diseases. The ADL scale used in CHARLS includes six indicators: eating, dressing, getting in and out of bed, bathing, using the toilet, and controlling urination and defecation. Disability was defined as limitations in two or more ADLs (5). Health state (ADL independence, disability, and death,
Supplementary Figure S1 ) transition probabilities and risks were calculated using R (4.3.1, R Foundation for Statistical Computing, Vienna, Austria). An MSM was used, assuming that health state transitions depend only on the current state and can occur multiple times between observation periods. The maximum likelihood method was used to estimate parameters and obtain health state transition probabilities for different characteristic groups (6). Age- and sex-specific LE and DFLE by multimorbidity status were estimated using the micro-simulation method in SAS (version 9.4, SAS Institute Inc, Cary, USA). A cohort of 100,000 individuals aged 60 years and older was simulated, and survival time in different health states from age 60 to death was obtained by controlling the cohort’s health and survival trajectory.Status Survey year 2011 2013 2015 2018 2020 Total 5,530 5,157 4,887 4,445 4,167 ADL independence 5,265 4,599 4,232 3,605 3,458 Disability 265 271 283 285 288 Death 0 287 372 555 421 Abbreviation: ADL=activities of daily living. Table 1. Trends in health status and sample size from 2011 to 2020.
Table 2 demonstrates that multimorbidity is a significant risk factor for transitioning from an independent state to disability [hazard ratio (HR) 1.49, 95% confidence interval (CI) 1.25, 1.77]. However, multimorbidity did not significantly affect transitions from independence to death, recovery from disability, or disability to death.
Transition state HR (95% CI) ADL independence to disability 1.49 (1.25, 1.77) ADL independence to death 1.26 (0.98, 1.63) Disability to ADL independence 1.30 (0.92, 1.84) Disability to death 1.13 (0.87, 1.47) Abbreviation: HR=hazard ratio; CI=confidence interval; ADL=activities of daily living. Table 2. Risk of health state transitions in individuals with multimorbidity versus those without multimorbidity.
As shown in
Supplementary Table S1 , multimorbidity significantly affected LE, DFLE, and the percentage of DFLE in older adults, with variations observed across gender and age. Specifically, multimorbidity had a more pronounced adverse effect on the LE and DFLE of males younger than 75 years, while its impact was greater on females aged 75 years and older. The percentage of DFLE exhibited a consistent decline across genders before the age of 75, but a steeper decline was observed among males aged 75 years and older.Figure 1 illustrates the influence of multimorbidity on LE, DFLE, and the proportion of disability life expectancy (DLE) to LE (DLE/LE) in older men and women. Multimorbidity significantly impacts DLE/LE, exhibiting age-related variations. Before age 75, men have a slightly lower proportion of DLE/LE than women. However, around age 75, the proportion for men surpasses that of women and increases at a significantly faster rate, creating a widening gap. Conversely, without multimorbidity, DLE/LE ratio remains comparable between sexes and is not significantly affected by age.
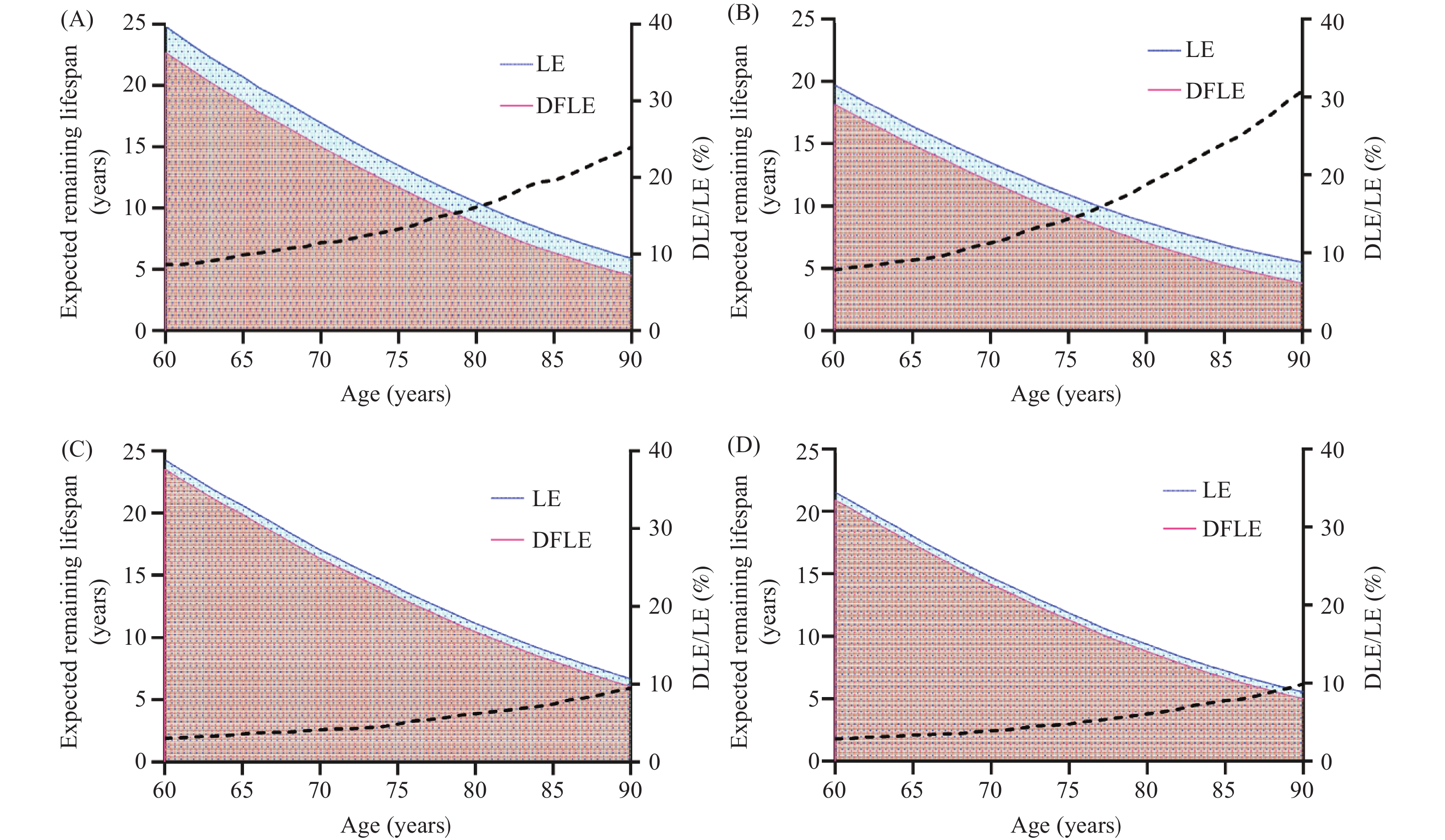 Figure 1.
Figure 1.Expected remaining lifespan and disabled life expectancy for males and females aged 60–90 with and without multimorbidity. (A) Females with multimorbidity; (B) Males with multimorbidity; (C) Females without multimorbidity; (D) Males without multimorbidity.
Abbreviation: LE=life expectancy; DLE=disability life expectancy; DFLE=disability-free life expectancy. -
Current life table models often neglect multimorbidity when calculating health status transitions and health expectancy in older adults (7). Few studies have estimated the impact of multimorbidity on LE and health expectancy loss in aging populations. This study addresses this gap by using longitudinal data and advanced statistical methods to analyze the effects of multimorbidity on functioning and longevity in older Chinese adults. Our findings provide new insights into population health dynamics within the context of global aging.
This study demonstrates that multimorbidity increases the risk of older adults transitioning from ADL independence to ADL disability, but does not significantly impact the risk of other health status transitions. Further research disaggregating degrees of disability may yield more nuanced findings.
This study demonstrates that multimorbidity negatively impacts LE and DFLE in older adults, with differing effects observed between sexes. After age 75, males exhibit lower DFLE and higher DLE/LE ratios compared to females. This aligns with previous research indicating decreased health expectancy in men (8), potentially attributable to the female life advantage (9) and greater healthcare utilization among women (10).
This study is subject to some limitations. First, it did not investigate the correlation between multimorbidity patterns, the number of chronic diseases, and disability, limiting the ability to tailor interventions based on risk levels. Second, disability was defined as the limitations in two or more ADLs, without in-depth analysis of subgroups with single or multiple ADL limitations, making it difficult to provide a full picture of the entire disability spectrum. Finally, the study focused solely on 14 common chronic diseases in CHARLS and did not adequately address psychological and mental illnesses, potentially underestimating their impact on disability.
In conclusion, multimorbidity significantly impacts the functional status of older adults in China, increasing disability risk and reducing healthy life years. This underscores the need to transition from a disease-oriented model to a patient-centered, holistic approach encompassing lifelong and life-cycle management (11). Notably, shifts in LE, DFLE, and the DLE/LE ratio before and after age 75 highlight the importance of enhanced health management for older men with multimorbidity. This includes early comprehensive geriatric assessments encompassing physical health, functional status, mental health, and social factors. The Chinese government should prioritize the development of multimorbidity-focused healthcare systems, moving away from single-disease management towards a multimorbidity management model. This transition can be facilitated through policy guidance, discipline development, and support for clinical projects to promote healthy aging (12).
-
No conflicts of interest.
HTML
| Citation: |

|