

 Download:
Download:




-
Human life expectancy (LE) has seen remarkable growth over the past century, with China’s LE rising from 35 years in 1949 to 78.99 years in 2024 (1). LE, a key metric in public health initiatives globally, is not influenced by population structure, allowing for comparisons across various demographics (2). However, traditional LE calculation methods, based predominantly on overall mortality rates, have hindered advances by not accounting for the different factors influencing mortality (3-4). Given the disparities in health risks among populations, particularly along gender and urban-rural lines, distinct mortality patterns (LE) are evident (5). Examining the influence of these gender-specific and urban-rural mortality patterns on the increase in LE enhances our understanding of health disparities among populations and provides an essential scientific basis and direction for improving public health policies and interventions (6).
To investigate the influence of diverse diseases and age-specific mortality rates on LE growth in China over the past 35 years, this study employs the Arriaga method. This technique provides a quantitative and systematic methodology for assessing the effects of shifts in population survival and mortality across different age brackets on LE. The analysis is conducted separately for urban and rural populations and is further stratified by gender.
Age-specific and cause-specific mortality data at the national level were sourced from the National Health Commission of China’s Death Registration System. This comprehensive system gathers data from a range of records, including medical certificates, population records, cancellation of household registrations from the Ministry of Public Security, civil affairs cremation records, and terminations from social security records (7). Using a multistage stratified cluster random sampling approach, the Death Registration System selects representative disease surveillance points across all 31 provincial-level administrative divisions (PLADs) in China. Initially, in 1990, the system monitored a population of 10 million, representing approximately 1% of the total population at that time. Since then, it has been progressively expanded; by 2021, it encompassed over 300 million people, approximately 24% of the national population, thereby enhancing its representativeness significantly.
In this study, participants were divided into age groups initially categorized as under 1 year, 1 to 4 years, and subsequently in 5-year intervals for those aged 4 years and older, culminating in an open-ended category for those aged 85 and above, resulting in a total of 19 groups. For analytical simplicity and clarity, these groups were further consolidated into four broader categories: 0–19 years, 20–59 years, 60–79 years, and 80 years and above. Diseases were classified based on the International Classification of Diseases, Tenth Revision (ICD-10). The categories included infectious and parasitic diseases (A00–B99, G00, G03–G04, N70–N73); respiratory diseases (H65–H66, J00–J06, J10–J18, J20–J22, U07.1); circulatory diseases (I00–I99); neoplasms, subdivided into malignant neoplasms (C00–C97) and other neoplasms (D00–D48); diseases of the digestive system (K00–K93); conditions originating in the perinatal period (P00–P96); external causes of morbidity and mortality, categorized as injury (V01–Y89); and other diseases.
Based on all-cause mortality rates across different age groups, a cohort of 100,000 individuals was created using life tables to calculate LE at birth. This study utilized annual data on attributed deaths and all-cause mortality obtained from the China Health Statistics Yearbook, covering urban and rural residents. Mortality rates for each cause were estimated accordingly (5). To analyze changes in mortality rates from 1987 to 2021, we employed the Arriaga decomposition technique. This method allowed us to break down the changes by age and cause, highlighting the direct, indirect, and interactive effects of changes in age-specific mortality rates on LE for specific diseases (8).
Statistical analyses were performed using R (version 4.3.3, R Foundation for Statistical Computing, Vienna, Austria) and Microsoft Office (version 2406, Microsoft, Redmond, Washington, USA).
As depicted in Figure 1, during the 35-year span from 1987 to 2021, both urban and rural regions in China exhibited a consistent increase in LE for both males and females. In 1987, the LE for urban males was 70.99 years, which climbed to 79.30 years by 2021, marking an increase of 8.31 years. Urban females experienced a rise from 73.96 years in 1987 to 84.52 years in 2021, an improvement of 10.56 years, which was notably greater than that observed in males. In rural areas, the LE for males advanced from 66.65 years in 1987 to 77.26 years in 2021, representing a significant gain of 10.61 years. Similarly, rural females saw their LE increase from 72.52 years in 1987 to 82.86 years in 2021, a total rise of 10.34 years.
 Figure 1.
Figure 1.Trends in life expectancy changes by gender in (A) rural and (B) urban areas in China from 1987 to 2021.
Abbreviation: LE=life expectancy.Figure 2 illustrates the contribution of various disease categories to LE growth across different demographic groups. For urban females, the decrease in mortality rates from circulatory and respiratory diseases contributed significantly to LE expansion, adding 2.91 and 2.69 years, respectively. Neoplasms accounted for a 1.23-year increase, while digestive system diseases contributed 0.62 years. Perinatal conditions and injuries each added 0.56 and 0.76 years, respectively. Infectious and parasitic diseases contributed 0.37 years, and other diseases added 1.41 years to LE growth. In urban males, reductions in mortality from respiratory diseases and circulatory diseases contributed 1.96 and 1.87 years, respectively, to LE growth. Neoplasms have accounted for a 1.27-year increase, and digestive system diseases added 0.52 years. Both perinatal conditions and injuries added 0.71 years each. Infectious and parasitic diseases contributed 0.46 years, while other diseases added 0.82 years to LE growth. For rural females, significant reductions in mortality from respiratory diseases contributed 3.81 years to LE growth. Circulatory diseases and infectious and parasitic diseases added 1.85 and 0.83 years, respectively. Neoplasms and digestive system diseases contributed 0.55 and 0.72 years, respectively. Perinatal conditions and external causes of morbidity and mortality contributed 0.51 and 0.29 years, respectively. Other diseases made a substantial contribution of 1.78 years to LE growth. In rural males, reductions in mortality from respiratory diseases marked a notable LE growth by contributing 2.84 years. Infectious and parasitic diseases made a significant contribution of 0.80 years. Circulatory diseases added 0.79 years, while neoplasms and digestive system diseases contributed 0.46 and 0.74 years, respectively. Perinatal conditions added 0.61 years, and injuries accounted for 0.13 years. Other diseases had the largest impact on LE growth, contributing 4.24 years.
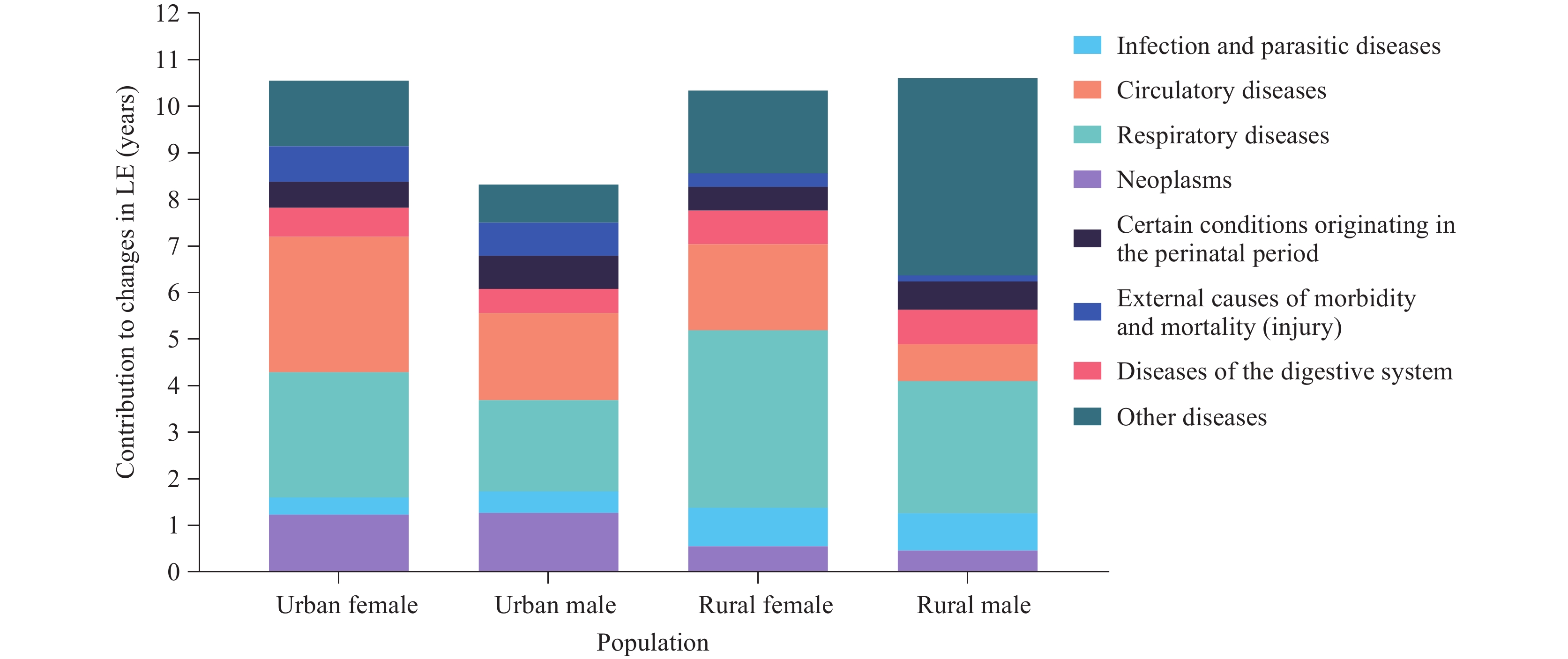 Figure 2.
Figure 2.Contributions of different causes of death to life expectancy growth for urban and rural populations in China between 1987 and 2021.
Abbreviation: LE=life expectancy.Figure 3 demonstrates how reductions in mortality rates across various age groups have contributed to LE increases for urban and rural males and females. For urban females, the most substantial increase originates from the 60–79 age group, which contributed a 5.0-year increase. This was followed by the 20–59 age group, which added 2.1 years. Contributions from the 0–19 and 80+ age groups were comparatively lower, at 1.6 years and 1.9 years, respectively. Among urban males, the most significant increase was noted in the 60–79 age group, contributing 3.6 years. The 0–19 age group added 1.8 years, and the 20–59 age group contributed 1.6 years. The smallest contribution came from the 80+ age group, adding just 1.3 years. In rural settings, females in the 60–79 age group saw the largest increase, contributing 3.2 years to LE. This was followed by the 20–59 age group, which added 2.7 years. Contributions from the 0–19 and 80+ age groups were 2.4 years and 2.1 years, respectively. For rural males, the highest contribution again came from the 60–79 age group, adding 3.8 years. Contributions from the 0–19 age group were 3.2 years, the 20–59 age group contributed 2.5 years, and the lowest was from the 80+ age group, at 1.1 years.
Supplementary Figure S1 further illustrates the changes in LE contributions from 1987 to 2021 by different age groups, including a more detailed categorization into 5-year intervals. Figure 3.
Figure 3.Contributions of different age groups to life expectancy growth for urban and rural males and females in China between 1987 and 2021.
Abbreviation: LE=life expectancy. -
Over the 35-year span from 1987 to 2021, LE in both urban and rural areas of China has seen a notable increase among both genders. This growth reflects substantial enhancements in the health status of urban and rural populations, driven by economic progress, elevated living standards, and significant improvements in medical conditions. The most substantial rise in LE was observed among rural males, at 10.61 years, exceeding the increases for urban males (8.31 years) and rural females (10.34 years). This trend suggests rapid advancements in rural regions, starting from a relatively lower baseline. Despite these gains, urban areas continue to exhibit higher overall LE, underscoring the ongoing health disparities between urban and rural settings.
The findings of this study indicate that the impact of various disease categories on LE varies across different genders and geographic locations. In urban environments, controlling circulatory (2.91 years) and respiratory diseases (2.69 years) is vital for extending the LE of females. Urban males, on the other hand, would benefit substantially from improved management and intervention for respiratory diseases (1.96 years) and other diseases (0.82 years). In rural settings, respiratory diseases markedly affect LE for both females (3.81 years) and males (2.84 years), which requires particular attention (9). Additionally, infectious and parasitic diseases significantly contribute to the increase in LE among rural males (0.80 years) and females (0.83 years). The greater increase in LE observed in urban females compared to urban males may be due to a variety of factors, including biological differences, lifestyle choices, and access to healthcare. Notably, women generally exhibit healthier behaviors and more proactive healthcare-seeking behaviors. To effectively address these gender disparities, targeted health strategies such as tailored health education programs and gender-specific medical interventions should be implemented.
Furthermore, declines in mortality rates across diverse age cohorts have played a crucial role in the extension of LE. In urban environments, females aged 60–79 have shown the greatest increase in LE, contributing an additional 5.0 years, with those aged 20–59 contributing a further 2.1 years. Urban males mirror this trend, with the 60–79 age group providing the most substantial LE increase of 3.6 years, underscoring the significance of health advancements within this demographic. Similarly, in rural settings, female LE gains were most pronounced in the 60–79 age group, with an extension of 3.2 years, followed closely by the 20–59 age group at 2.7 years. Rural males experienced the largest LE increment from the 60–79 age cohort, adding 3.8 years.
Our results corroborate previous research emphasizing the pivotal role of non-communicable diseases (NCDs) in shaping LE trends (7). Consistent with other studies, both in developed and developing countries, circulatory and respiratory diseases have been identified as significant contributors to LE enhancements (5). The decline in mortality rates from circulatory diseases can largely be attributed to public health policies such as the “Healthy China 2030” initiative, which centers on cardiovascular health by promoting preventive approaches, facilitating early detection, and ensuring effective management. Similarly, efforts aimed at curtailing respiratory diseases, including nationwide smoking cessation programs and initiatives to improve air quality, have markedly reduced mortality rates. In comparison with countries like Japan and South Korea, which have also achieved improvements in LE through public health policies and advancements in healthcare, China’s “Healthy China 2030” program embodies analogous successful tactics. These international instances underscore that specific interventions and robust healthcare infrastructures are critical for boosting LE. Furthermore, research exploring health disparities between genders shows that females typically see more substantial increases in LE than males — a finding that aligns with our observation of more pronounced LE gains among urban females compared to urban males (4,10).
This study is subject to some limitations. First, although the data are representative, the analysis may be impacted by potential inaccuracies due to changes in ICD coding over the years. Second, the focus on broad disease categories may obscure more nuanced insights that could be gained from examining sub-classifications within each category. This oversight could potentially conceal significant trends within these subcategories. Future research would benefit from a more detailed classification of these external causes to facilitate a deeper understanding. Third, external influences such as environmental changes and socioeconomic developments could also affect LE, yet these factors were not comprehensively accounted for in our analysis.
Despite these limitations, the results offer actionable recommendations for future public health initiatives. Public health authorities should create targeted interventions that address significant factors contributing to LE growth, specifically circulatory and respiratory diseases, with a focus on at-risk groups such as residents of rural communities and the elderly. Strengthening healthcare delivery systems and mitigating health disparities between urban and rural areas are essential for the successful achievement of sustainable health development goals. Additionally, future studies should incorporate environmental and socioeconomic variables to yield a more holistic understanding of the determinants of LE.
In conclusion, this study highlights several factors contributing to the increase in LE in China over the past 35 years. Key factors include reductions in mortality from specific diseases and overall health improvements across various age demographics. Notably, the significant decline in mortality rates among individuals aged 60–79 has played a pivotal role in raising the national LE, which underscores the importance of targeting health interventions within this age group. Additionally, marked improvements in managing diverse diseases across different groups highlight the crucial role of comprehensive healthcare services and effective disease control strategies. These findings provide a robust scientific foundation for developing public health policies and offer insightful lessons for other developing nations seeking to improve LE through similar measures derived from China’s experiences.
-
No conflicts of interest
HTML
| Citation: |

|