
 Download:
Download:




-
On January 23, 2024, the Anhui provincial CDC received a cooperation report from the Zhejiang provincial CDC and subsequently initiated a retrospective epidemiological study to investigate the epidemiology, clinical characteristics, and etiology involved. On December 1, the patient reported experiencing fever symptoms, although the temperature was not measured; these symptoms persisted without improvement on December 2. Due to a worsening condition, the patient was admitted to the Guangde County Traditional Chinese Medicine Hospital on the morning of December 3 with suspected pneumonia. On January 25, sequencing conducted by the China CDC revealed that the patient’s sample contained the complete genome sequences of both the seasonal influenza A (H3N2) virus and the influenza A (H10N5) virus.
According to the guidelines from the China CDC, close contacts are defined as: 1) medical personnel or other caregivers; 2) household members and individuals with close contact, and 3) others determined by on-site investigators. During the epidemiological investigation, health officials conducted retrospective health follow-ups on 30 close contacts, including 15 medical staff from Guangde Hospital of Traditional Chinese Medicine, 10 staff members from the same ward, 2 neighbors, and 3 family members. None of these individuals showed signs of infection, and all tested negative for the virus using nucleic acid assays. All close contacts last interacted with the cases between December 1–17, 2023. Investigators collected 189 samples from various sources, including live poultry, environmental sites, and individuals in locations linked to the patient, such as their home, adjacent households, supermarkets, mobile vendors, live duck wholesale markets, and stand-alone live chicken vendors. These samples were sent to the CDC, with 167 completing laboratory testing. Analysis revealed 28 positive results: 14 for H10N5, 3 for N5 nucleic acid fragments, and 11 for other subtypes including H5, H6, H9, N1, N2, and N6. Additionally, 30 serum samples from close contacts were subjected to pseudovirus-based neutralization tests for H10N5 antibodies, all of which yielded negative results.
-
On January 30, 2024, a 63-year-old female was confirmed as the first case of co-infection with influenza A viruses H3N2 and H10N5, following laboratory tests at a hospital. The investigation revealed that she had passed away, with activity information obtained from her contacts. Notably, the H10N5 virus sequence was identified in frozen duck meat from her home refrigerator. The patient had slaughtered a live duck at her home on November 26. She began experiencing symptoms on December 1, 2023, including fever (unquantifiable), cough, green sputum, headache, fatigue, and chest pain, suggesting an incubation period of 5 days. She had pre-existing conditions: hypertension, type 2 diabetes, cerebral infarction, gouty arthritis, and heart failure. Her fever, initially unquantified, escalated with high temperatures in the afternoons and evenings, peaking at 40.4 °C from December 4 to 6. Arterial blood gas analysis on December 6 confirmed Type I respiratory failure. Due to worsening conditions, she was transferred to the intensive care unit (ICU) at the First Affiliated Hospital of Zhejiang University School of Medicine (Yuhang District, Hangzhou) on December 7, where she was diagnosed with Type I respiratory failure and severe pneumonia. She succumbed to the illness on December 16. Expanded influenza sentinel surveillance in Guangde City did not detect H10N5 or other avian influenza subtypes. An epidemiological investigation, including retrospective health follow-ups of 30 close contacts, found all to be asymptomatic and negative for the virus (Figure 1A).
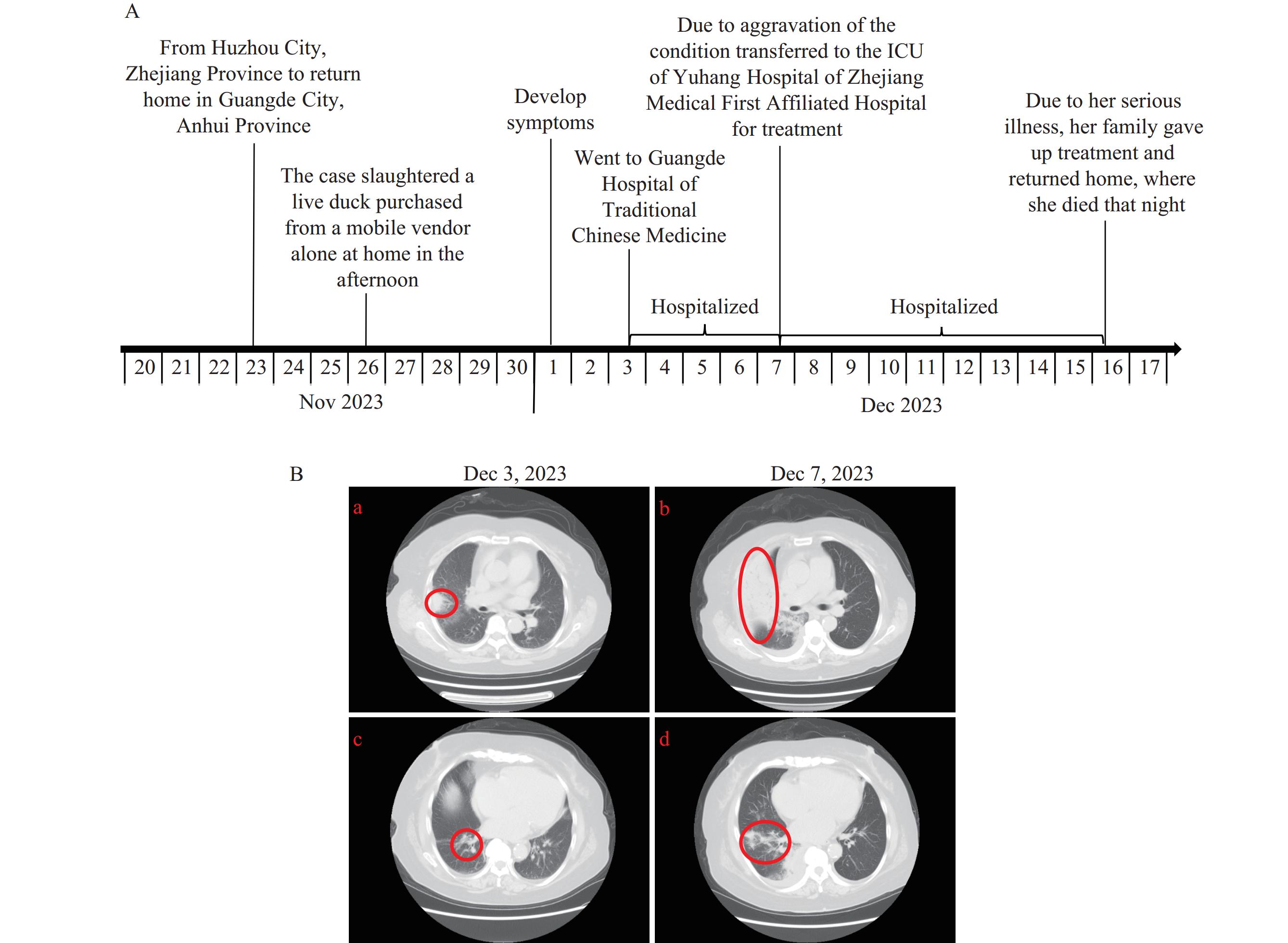 Figure 1.
Figure 1.The timeline and chest CT image of the case. (A) The time-line occurrence in days of this case; (B) The chest CT image characteristics of this case.
Note: In Figure 1B, (a) shows the upper lobe of this case’s right lung on December 3, 2023; (b) shows the upper lobe of this case’s right lung on December 7, 2023; (c) shows the lower lobe of this case’s right lung on December 3, 2023; and (d) shows the lower lobe of this case’s right lung on December 7, 2023.
Abbreviation: CT=computed tomography.
From December 3 to December 7, the patient was admitted to Guangde Traditional Chinese Medicine Hospital, where several abnormal clinical laboratory test results were observed. These tests included complete blood count, high-sensitivity C-reactive protein (CRP), biochemical parameters, coagulation function, glycated hemoglobin, urinalysis, and comprehensive tumor markers, as detailed in Table 1. On December 3, sputum pathogen testing showed white blood cell (WBC) >25/LP, squamous epithelial cell (SEC) <10/LP, Gram-positive cocci 4+, and Gram-negative bacilli 2+. No acid-fast bacilli were detected. Bacterial culture and identification, following 5 days of aerobic and anaerobic incubation, showed no growth. Tests for novel coronavirus nucleic acid and influenza A virus antigen were negative. Imaging studies revealed pathological changes in the patient’s right lung. On December 3, 2023, chest computed tomography (CT) imaging identified patchy high-density shadows in the upper lobe (a) and striated shadows in the lower lobe (c). By December 7, the CT displayed multiple flaky and patchy high-density shadows across the right lung, markedly increased in number compared to earlier images (b), with some areas of lung tissue appearing solid and with indistinct borders. An air bronchogram was visible in the inner lung accompanied by pleural effusion (d) (Figure 1B).
Laboratory test items December 3 Results tips December 7 Results tips Blood cells + Hypersensitive CRP Hematocrit (%) 41.7 33.8 ↓ Platelets (109/L) 149 114 ↓ Large platelet ratio (%) 30.8 45.3 ↑ White blood cells (109/L) 11.94 ↑ 13.3 ↑ Number of neutrophils (109/L) 9.16 ↑ 12.72 ↑ Monocyte count (109/L) 1.28 ↑ 0.23 Number of eosinophils (109/L) 0 ↓ 0 ↓ Neutrophil percentage (%) 76.8 ↑ 95.9 ↑ Lymphocyte percentage (%) 12.1 ↓ 2.2 ↓ Monocyte percentage (%) 10.7 ↑ 1.7 ↓ Eosinophilic percentage (%) 0 ↓ 0.2 C-reactive protein (mg/L) 50.58 ↑ 237.7 ↑ Hypersensitive C-reactive
protein (mg/L)>10.00 ↑ >10.00 ↑ Blood Biochemistry Total bilirubin (umol/L) 33.4 ↑ 22.1 Direct bilirubin (umol/L) 7.5 ↑ 8.9 ↑ Indirect bilirubin (umol/L) 25.9 ↑ 13.2 Albumin (g/L) 49.1 37.9 ↓ White ball ratio 1.38 1.17 ↓ Glutamic-pyruvic transaminase (U/L) 21.1 56.8 ↑ Glutamic oxaloacetic transaminase (U/L) 16.1 67.7 ↑ Lactate dehydrogenase (U/L) 197.4 421.7 ↑ Alpha-hydroxybutyrate
dehydrogenase (U/L)148.1 290.1 ↑ Creatine kinase (U/L) 37.5 ↓ 103 Phosphorus (mmol/L) 1.13 0.61 ↓ Glucose (mmol/L) 16.35 ↑ 18.18 ↑ High-density lipoprotein (mmol/L) 1.64 ↑ 1.06 Potassium (mmol/L) 3.1 ↓ 2.8 ↓ Chlorine (mmol/L) 96 ↓ 96 ↓ Clotting function Fibrinogen (g/L) 6.09 ↑ 8.06 ↑ D-dimer (μg/mL) 0.28 2.35 ↑ Hemoglobin A1C Hemoglobin A1C (%) 7.3 ↑ Urine routine Glucose 3+ ↑ Urinary occult Blood 1+ ↑ White blood cells 1+ ↑ Protein +- ↑ Ketone bodies +- ↑ Vitamin C 1+ ↑ Tumor set Free triiodothyronine (pmol/L) 3.22 ↓ SARS-CoV-2 antibody SARS-CoV-2-IgG Positive (+) Notes: “↑” indicates the high side; “↓” indicates the low side.
Abbreviation: CPR=C-reactive protein; SARS-CoV-2=severe acute respiratory syndrome coronavirus 2.Table 1. The results of laboratory tests during the treatment of the case — Anhui Province, China, December 2023–January 2024.
Investigations identified H10N5 nucleic acid fragments in environments linked to the transmission chain, including homes, mobile vendors, and live duck wholesale facilities. Retrospective field investigations revealed that the live ducks slaughtered by the patient were purchased from a mobile vendor, with two of the vendor’s storage locations testing positive for H10N5. The mobile vendor sourced these live ducks from a wholesale factory, where five samples also tested positive for H10N5. This wholesale factory obtained its live ducks from two sources: a breeding farm in Xuanzhou District and from Yichun City in Jiangxi Province. However, neither of these supply chains tested positive for H10N5 in this retrospective investigation. Despite these findings, field investigations detected H10N5 in seven frozen duck meat samples from the patient’s refrigerator. Genetic analysis of the H10N5 sequences isolated from these samples confirmed that the Hemagglutinin (HA) and Neuraminidase (NA) genes shared 96.2% and 99.9% similarity, respectively, with those identified in the patient. The HA genes were part of the American lineage of H10N5, showing 95.2% homology with A/Anser albifrons/South Korea/22JN-163-1/2022 (H10N7) (GenBank: OQ296824.1). Conversely, the NA genes belonged to the Eurasian lineage, with the highest homology (97.82%) to A/Spot-billed duck (Anas poecilohyncha)/Korea/KNU17/2022 (H6N5) (GenBank: OR674089.1) (Figures 2 and 3). Resistance analysis revealed no mutations that confer resistance to neuraminidase inhibitors (e.g., oseltamivir) or polymerase inhibitors (e.g., baloxavir), suggesting these antiviral agents remain effective against the virus. All close contacts of the patient tested negative for H10N5 (Table 2).
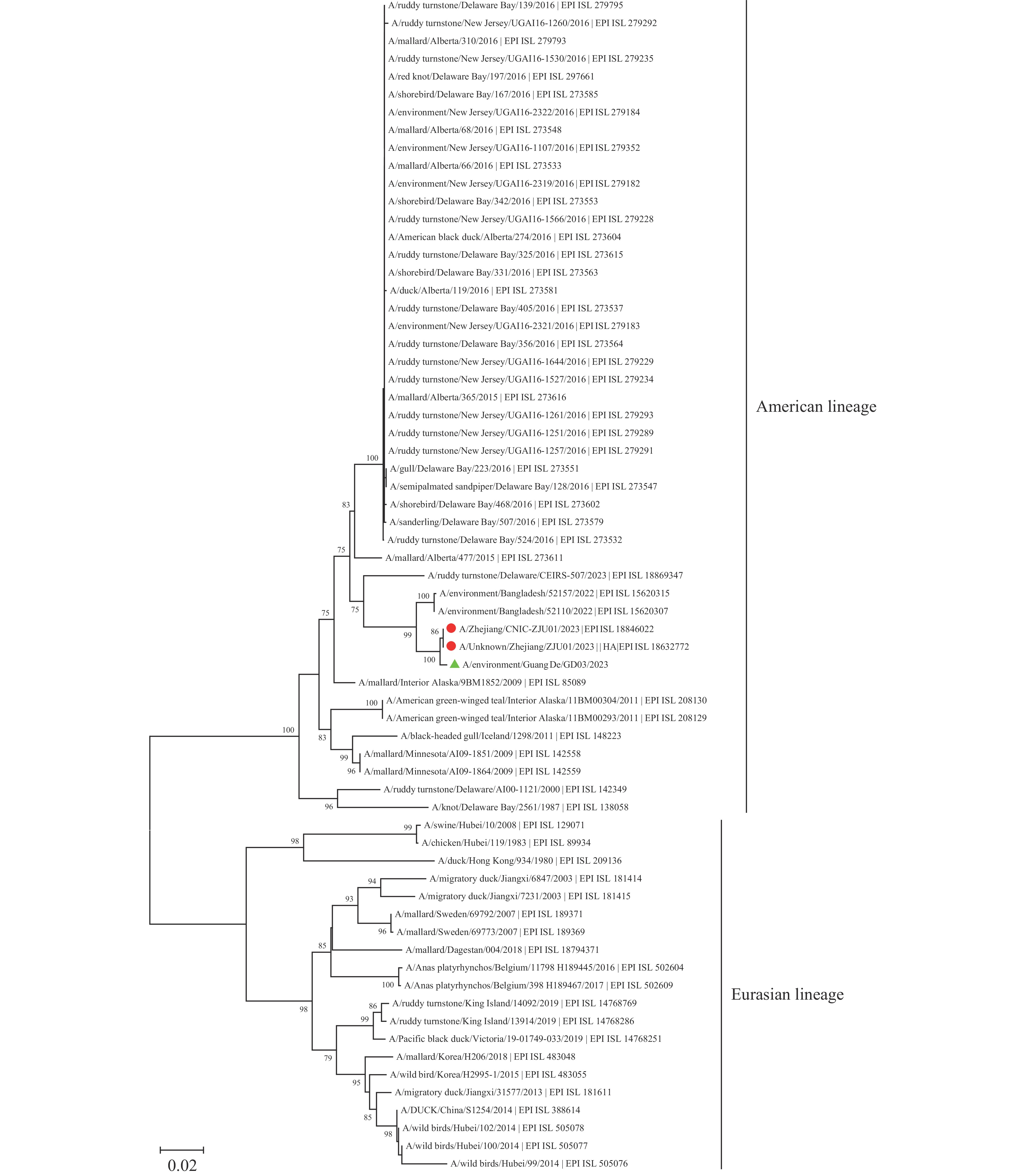 Figure 2.
Figure 2.Neighbor-joining phylogenetic tree of HA gene of the H10N5 in this study.
Note: the red circle represented the HA gene sequence of the H10N5 isolated from the case. The green triangle represented the HA gene sequence of the H10N5 isolated from the frozen duck meat samples in the patient’s refrigerator.
Abbreviation: HA=Hemagglutinin.
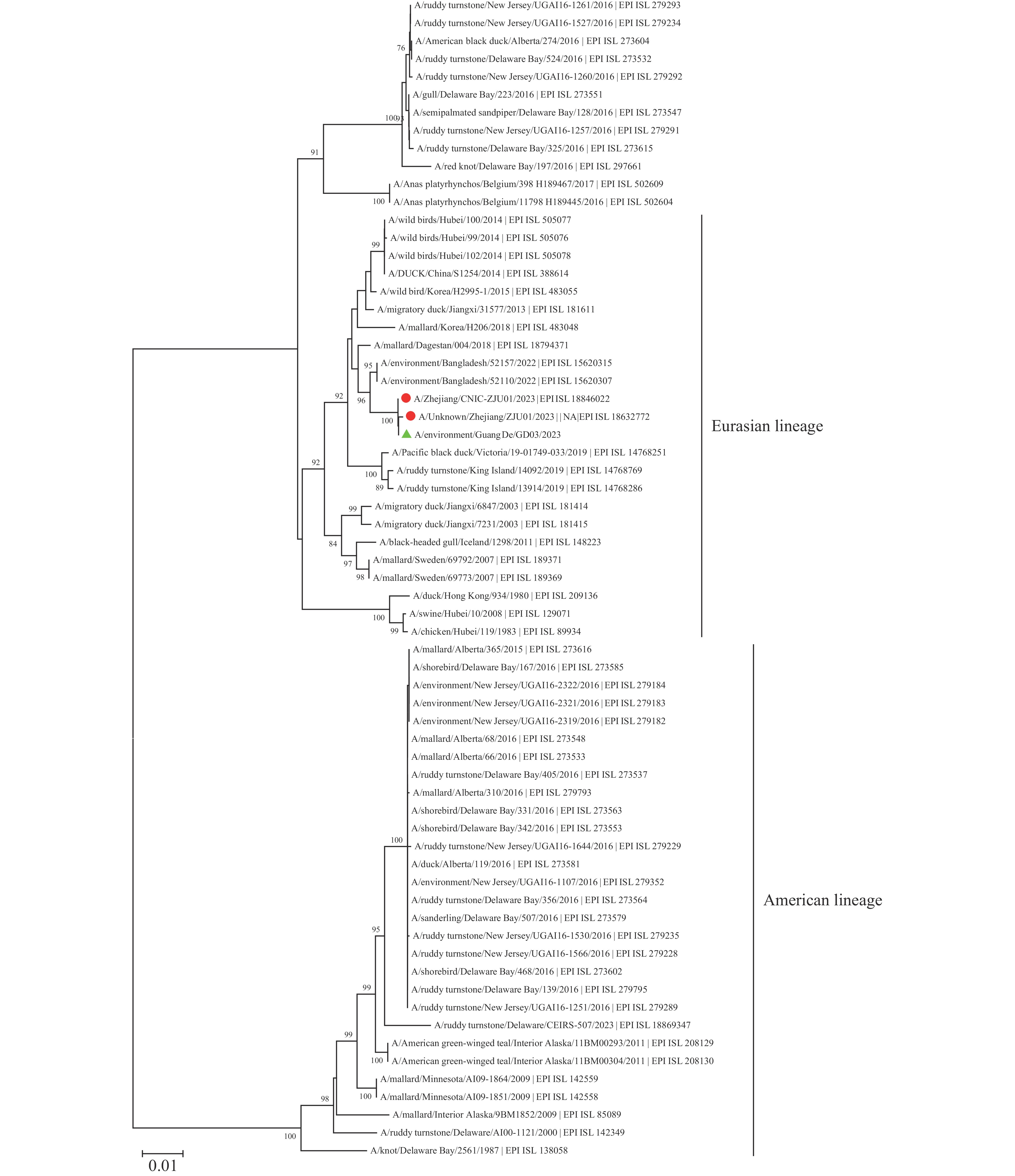 Figure 3.
Figure 3.Neighbor-joining phylogenetic tree of NA gene of the H10N5 in this study.
Note: the red circle represented the NA gene sequence of the H10N5 isolated from the case. The green triangle represented the NA gene sequence of the H10N5 isolated from the frozen duck meat samples in the patient’s refrigerator.
Abbreviation: NA=Neuraminidase.
-
In response to the epidemic, government departments have prioritized establishing joint investigation teams, conducting thematic risk assessments, performing epidemiological investigations, tracing potential sources of infection and situations of common exposure or close contact, and collecting environmental specimens for testing. Enhanced surveillance of influenza-like illnesses has also been implemented. Management measures include cleaning and disinfecting poultry markets, closing and rectifying affected live poultry markets, and conducting terminal disinfection.
Healthcare workers are being instructed on personal protection and the prevention and control of nosocomial infections. Concurrently, the public is being educated on the prevention and control of human avian influenza. Sustained and effective intervention measures have been implemented to curb the spread of avian influenza, which include enhancing the capacity of medical institutions to detect, diagnose, and report human cases of avian influenza.
Additionally, a two-week, citywide intensive surveillance of influenza-like cases has been mandated. This surveillance will particularly focus on laboratory screening for human avian influenza virus in suspected severe pneumonia cases. Concurrently, public health education efforts will be reinforced. A crucial measure involves local government organization and leadership to foster cooperation among health, agriculture, and market departments to further enhance human and avian influenza surveillance (1–5).
-
The case under investigation, managed in Anhui Province from December 1 to 3, was retrospectively analyzed for this period. Epidemiologically and clinically, the patient resembled those in previous reports of human infections with H10N8 in Jiangxi Province during 2013–2014 (6–7). All patients were elderly, had pre-existing health conditions, and had either direct or indirect exposure to poultry. They exhibited a short incubation period followed by rapid disease progression. Importantly, no transmission to close contacts was observed in these cases (8–9). Comparing H10N8 to H10N3 infections, similarities include exposure to live poultry and symptoms such as cough, fever, and chest CT imaging showing patchy high-density shadows. Elevated levels of C-reactive protein, lactate dehydrogenase, and D-dimer were also common (8,10). Both H10N5, H10N3, and H10N8 infections can lead to severe pneumonia and Type I respiratory failure (11). However, unlike H10N5, H10N3 can infect healthy young individuals and is associated with leukopenia (8,10).
Investigations identified H10N5 nucleic acid fragments in households associated with cases, mobile vendors, and live duck wholesale facilities. Retrospective inquiries, however, found no evidence of H10N5 in the original sources of the live ducks, suggesting that the virus might have been introduced or transmitted at later stages. Sequence analysis of the H10N5 subtype of the avian influenza A virus revealed that the HA segment belongs to the American lineage, while the NA segment originates from the Eurasian lineage. The spread of H10 viruses is closely linked to wild bird migration (12); these viruses, due to their low pathogenicity and absence of noticeable symptoms, can continuously replicate within bird populations, increasing the likelihood of viral mutations and complex reassortment events (13). Previous studies have demonstrated that in southern China, domestic ducks serve as a crucial intermediary between migratory waterfowl and terrestrial poultry (14–16), thus playing a key role in inter-subtype interactions among influenza viruses (17).
Given that this is the first recorded case of H10N5 infecting humans, there is limited understanding of its infection mechanism, and follow-up cases are scarcely documented. Previous studies have indicated that after multiple passages in mice, the H10N5 virus exhibits increased virulence and mutations in its PB2 and HA proteins, suggesting a significant risk to human health (12). The H10N5 avian influenza virus shares exposure patterns, epidemiological characteristics, and clinical manifestations with other avian influenza viruses that infect humans, such as H5N8 and H10N3. Currently, there is no evidence of human-to-human transmission. Sequence analyses and local trace-back results imply that the likelihood of the virus originating locally is minimal, with speculation pointing to long-distance transmission from wild birds.
-
No conflicts of interest.
-
No. Sex Occupation Earliest contact date Latest contact date Frequency of contact Place of contact Mode of contact Nucleic acid test result Serum test results 1 Male Self-employed electrician Dec 2 Dec 17 1 1, 2 7, 8 Neg. Neg. 2 Female Worker Dec 2 Dec 17 1 1, 2 7, 8 Neg. Neg. 3 Male Worker Dec 2 Dec 17 1 1, 2 7, 8 Neg. Neg. 4 Female Nurse Dec 2 Dec 7 1 2 6 Neg. Neg. 5 Female Nurse Dec 2 Dec 7 1 2 6 Neg. Neg. 6 Female Nurse Dec 2 Dec 7 1 2 6 Neg. Neg. 7 Female Nurse Dec 2 Dec 7 1 2 6 Neg. Neg. 8 Female Nurse Dec 2 Dec 7 1 2 6 Neg. Neg. 9 Female Nurse Dec 2 Dec 7 1 2 6 Neg. Neg. 10 Female Nurse Dec 2 Dec 7 1 2 6 Neg. Neg. 11 Female Nurse Dec 2 Dec 7 1 2 6 Neg. Neg. 12 Female Nurse Dec 2 Dec 7 1 2 6 Neg. Neg. 13 Male Doctor Dec 2 Dec 7 1 2 6 Neg. Neg. 14 Male Doctor Dec 2 Dec 7 1 2 6 Neg. Neg. 15 Female Doctor Dec 2 Dec 7 1 2 6 Neg. Neg. 16 Male Doctor Dec 2 Dec 7 1 2 6 Neg. Neg. 17 Female Doctor Dec 2 Dec 7 1 2 6 Neg. Neg. 18 Female Doctor Dec 2 Dec 7 1 2 6 Neg. Neg. 19 Male Farmer Dec 1 Dec 7 2 1 7 Neg. Neg. 20 Female Farmer Dec 2 Dec 7 2 1 7 Neg. Neg. 21 Male Patient in same ward Dec 3 Dec 7 1 2 3 Neg. Neg. 22 Female Patient in same ward Dec 3 Dec 7 1 2 3 Neg. Neg. 23 Male Patient in same ward Dec 5 Dec 7 1 2 3 Neg. Neg. 24 Female Patient in same ward Dec 5 Dec 1 1 2 3 Neg. Neg. 25 Male Patient in same ward Dec 5 Dec 1 1 2 3 Neg. Neg. 26 Male Patient in same ward Dec 3 Dec 5 1 2 3 Neg. Neg. 27 Female Patient in same ward Dec 3 Dec 5 1 2 3 Neg. Neg. 28 Female Patient in same ward Dec 3 Dec 5 1 2 3 Neg. Neg. 29 Female Patient in same ward Dec 3 Dec 7 1 2 3 Neg. Neg. 30 Male Patient in same ward Dec 3 Dec 7 1 2 3 Neg. Neg. Note: Frequency of contact: 1=daily; 2=multiple times (with specified dates or date range); and 3=once only. Places of contact: 1=home; 2=medical institution; 3=workplace; 4=restaurant; 5=park; and 6=other. Modes of contact (multiple options possible): 1=shared meals; 2=same room; 3=same ward; 4=shared personal items; 5=secretions, excreta, etc.; 6=medical treatment, nursing; 7=visitation; 8=accompaniment; and 9=other. “Neg.” indicates Negative. Table 2. List of close contact information with the case in Guangde between December 1–17, 2023.
HTML
| Citation: |

|