

 Download:
Download:




-
The initiation of the pandemic’s fifth wave has been attributed to the emergence of the Omicron variant, with the initial outbreak traced back to the Seaview Silhouette Hotel, a quarantine facility where cross-infection occurred in early January 2022 (1). The concurrence of this outbreak with the Chinese New Year celebrations, a period characterized by increased social interactions, significantly exacerbated the spread of the virus. The escalation in case numbers began to place an immense burden on the healthcare infrastructure from February 9 onward, ultimately leading to an overwhelming of public hospitals and isolation centers (2).
In the past, the Hong Kong Special Administrative Region (HKSAR) has faced four outbreaks and has generally adopted China’s epidemic prevention policies effectively (3). However, during the fifth wave of the pandemic, the prevalent strain was Omicron subtype BA.2, known for its high infectivity but low pathogenicity. Coupled with a significant number of asymptomatic cases, the dense population in HKSAR, China, and inadequate medical tracing methods, this scenario resulted in challenges in implementing effective control measures and contributed to the rapid spread of the pandemic.
To support the HKSAR and decrease mortality rates, the Central Government of China mobilized resources on February 16, 2022. These resources included testing facilities, medical staff, construction of isolation centers, medical equipment, and provision of coronavirus disease 2019 (COVID-19) medications (4). Furthermore, the HKSAR government made a crucial decision by introducing effective oral medications for COVID-19 treatment, specifically Nirmatrelvir/ritonavir (Paxlovid, Pfizer). This drug significantly reduced hospitalizations and mortality by 89% among high-risk COVID-19 patients and has been authorized for commercialization following successful clinical trials (5).
The study aims to evaluate the impact of timely medical resource allocation and oral medication usage on decreasing mortality during the fifth wave of the HKSAR pandemic. The findings will serve as a scientific reference for managing future pandemics caused by other SARS-CoV-2 strains or viruses.
HTML
-
Data were extracted from the Oxford COVID-19 Government Response Tracker (OxCGRT) (6) to analyze the evolution of government responses during the pandemic. Information on twelve indicators was collected from October 1, 2020, to July 7, 2022, from the OxCGRT database (
https://github.com/OxCGRT/covid-policy-tracker ). COVID-19 confirmed cases, deaths, and serial interval data were obtained from the official HKSAR Department of Health database (7). -
We examined 12 specific indicators concerning interventions implemented to reduce COVID-19 spread in HKSAR. Details on the definition, source, and unit of measurement for each indicator can be found in
Supplementary Table S1 . Among these indicators, eight pertain to closures and containment measures (school closure, workplace closure, cancelation of public events, restrictions on gatherings, public transport closure, stay-at-home orders, restrictions on internal movement, and international travel controls), while four are associated with health measures (testing policy, contact tracing, vaccination policy, and protection of older adults).To evaluate the impact of different control measures on the growth of the pandemic in HKSAR, we utilized the R vars package (Bernhard Pfaff, Germany) within the R statistical software (version.3.6.1; R Foundation for Statistical Computing, Vienna, Austria) (8). Initially, we employed vector autoregression (VAR) modeling to examine the interrelationships of various variables over time. To strengthen the causality assessment, we incorporated the Granger Causality test into the VAR model to determine if changes in predictors lead to alterations in infection growth. A Wald test was conducted to calculate the P value.
-
To facilitate the transmission of SARS-CoV-2 Omicron variants in the HKSAR, we established a pandemic model known as the Susceptible-Exposed-Infected-Active-Quarantined-Recovered-Hospitalized-Death (SEIAQRHD) model (
Supplementary Figure S1 ). The model parameters predominantly encompass viral properties and variables associated with severity rates and mortality. Our calculations and analyses were conducted using R statistical software and Python (version 3.8; Python Software Foundation, Beaverton, OR, US). -
In order to assess whether the distribution of domestic medical resources to HKSAR was associated with a reduction in fatalities during the pandemic, this study created simulations of the fatality curves with and without the allocation of these resources. The medical resource allocation to HKSAR commenced on February 16, 2022. It was hypothesized that there would be a seven-day lag in the initiation of an effective response and in the turnaround time for nucleic acid test results. Therefore, daily mortality rates were calculated for the periods before and after February 22 to evaluate the impact of resource distribution. The fifth wave of the outbreak in HKSAR, which began to result in fatalities on February 7, served as a baseline. For the control scenario, actual data from February 7 to February 22, a period with no medical resource allocation, was used. For the intervention analysis, actual data from February 23 to March 26, following the commencement of resource distribution, was collated.
The study simulated the trend in fatalities without domestic medical resource allocation by referencing the Omicron mortality rate in Japan from January 16 to March 26, 2022, as control measures in HKSAR mirrored those in Japan during this time (
Supplementary Figure S2 ) (9). Exponential regression was applied to estimate the mortality rate trend in HKSAR from February 7 to February 22 using fatalities data, given the exponential distribution of the overall trend (Equation 1). Subsequently, the modified SEIAQRHD model was used to project fatalities from the fifth wave of the pandemic without domestic medical resource allocation. For scenarios involving domestic medical resource allocation, logarithmic regression demonstrated superiority over other methods, as shown inSupplementary Table S3 . Therefore, the mortality rate trend in HKSAR was forecasted using fatalities data from February 23 to March 26, 2019, through logarithmic regression (Equation 2), followed by predicting the number of deaths using the SEIAQRHD model.$$ \mathrm{\lambda }=\mathrm{k}\times \mathrm{e}^\mathrm{x}+\mathrm{b} $$ (1) $$ \mathrm{\lambda }\mathrm{\text{'}}=\mathrm{k}\mathrm{\text{'}}\times \mathrm{l}\mathrm{n}\left(\mathrm{x}\mathrm{\text{'}}\right)+\mathrm{b}\mathrm{\text{'}} $$ (2) COVID-19 oral medications (nirmatrelvir/ritonavir, molnupiravir) were introduced in the HKSAR on March 15, 2022 to potentially reduce pandemic fatalities. This study evaluated the effectiveness of these medications in a transmission dynamics model at that time to determine their impact on reducing mortality rates.
Data Sources
Correlation and Causality Analysis
Construction of the Dynamics Model
Simulation Scenarios


-
In early January 2022, the Omicron variant was first identified in the HKSAR and quickly spread. Subsequently, on January 7, the HKSAR government reinforced social distancing measures, leading to the cancellation of traditional events like the New Year’s Eve Flower Market and Chinese New Year celebrations. The HKSAR recorded 1,161 new confirmed COVID-19 cases on February 9, marking the highest daily tally in the past two years (Figure 1).
 Figure 1.
Figure 1.The fifth wave of the pandemic in HKSAR.
Note: The orange areas indicate the distribution period in the Chinese mainland since February 16, 2022.
Abbreviation: HKSAR=Hong Kong Special Administrative Region.
One week later, the Chinese central government provided a substantial quantity of medical resources to HKSAR, which included hospital beds, medical personnel, and materials for epidemic prevention. A module hospital in Tsingyi and a temporary nucleic acid testing laboratory were established (Table 1). Subsequently, the “Vaccine Pass” policy was officially enacted, allowing individuals with at least one vaccine dose or those exempted to access public areas such as shopping centers and hotels. Additionally, the HKSAR government introduced new medicines to combat coronavirus infections (Figure 2). However, on March 12, HKSAR reported 32,430 new confirmed cases, the highest daily count in this pandemic wave. Following April 16, the fifth wave of the COVID-19 pandemic in HKSAR began to gradually decrease, leading to a significant reduction in the number of fatalities.
Medical resource Before distributing to HKSAR After distributing to HKSAR Medical bed
Common beds, isolation beds (or negative pressure)A total of 29,000 medical beds in HKSAR About 20,000 isolation beds be added after the aid to HKSAR Nucleic acid detection capability The largest nucleic acid production in HKSAR is 100,000 per day Nucleic acid production reached 300,000 per day after mainland China’s aid to HKSAR Number of doctors By the end of 2020, there were 15,298 doctors and 61,295 nurses in HKSAR The number of doctors from the Chinese mainland who assisted HKSAR:
First batch; 4 experts, 8 nucleic acid testers
The second batch: 114 medical personnel
The third batch: 300 medical personnel and 5 experts
Fourth batch: 132 medical personnel
Fifth batch: 6 expertsMedical consumables – 100 million rapid antigen test kits, more than 120 million N95, KN95, 1.10656 million new coronavirus detection kits, 157 million surgical masks, 19 million pairs of surgical gloves, 3.62 million protective suits, 6.45 million thermometers, 194 million sheets of alcohol paper, etc. Drug – 195,000 boxes of Jinhua Qinggan Granules, more than 6 million boxes of Lianhua Qingwen Capsules, and 24,000 boxes of Huoxiang Zhengqi Tablets Other – 730,000 clip-on pulse oximeters, 2 mobile nucleic acid testing vehicles and 1 material transportation support vehicle Note: “–” means no medical resources.
Abbreviation: HKSAR=Hong Kong Special Administrative Region.Table 1. Distribution of medical resources to HKSAR during the fifth wave of the pandemic.
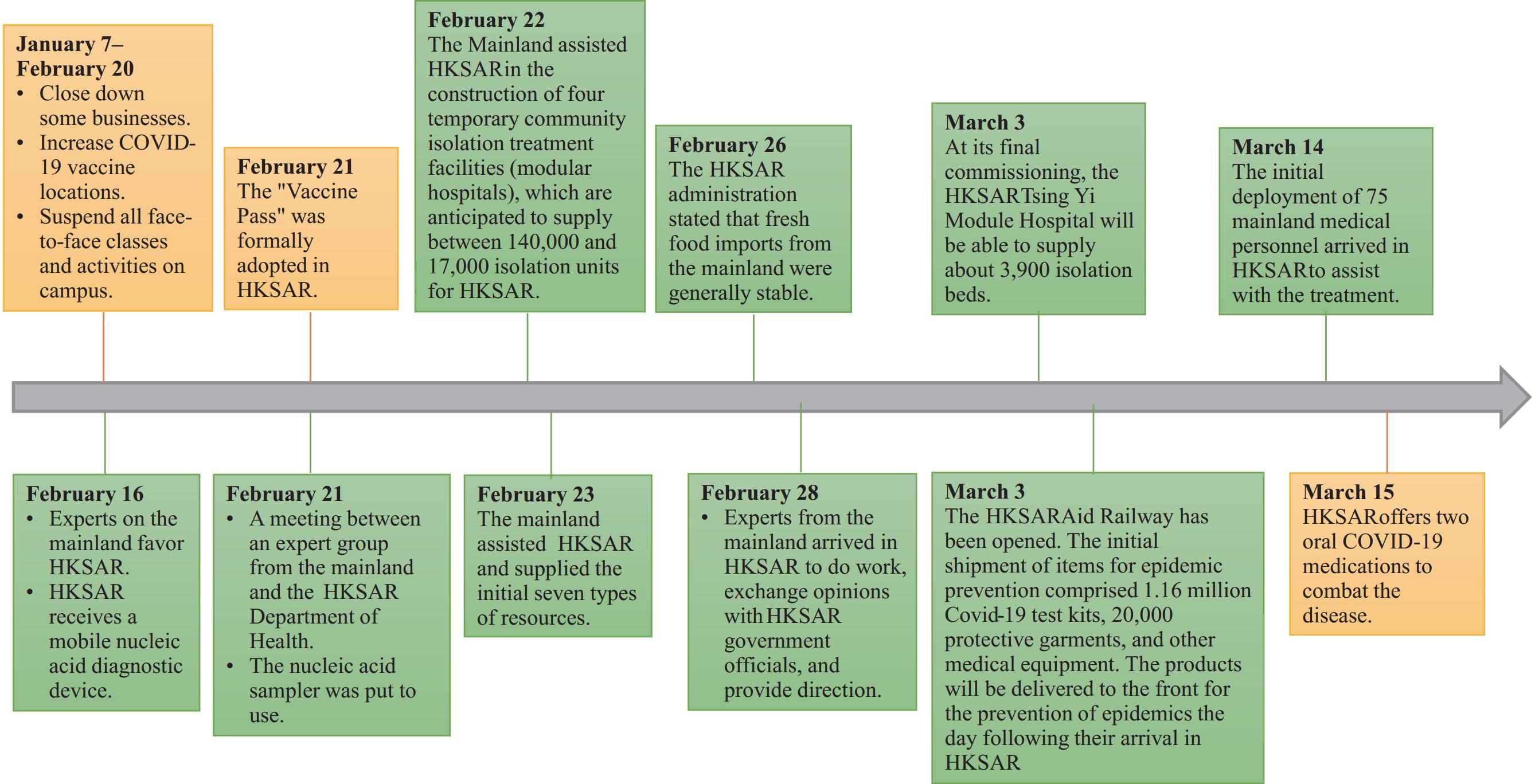 Figure 2.
Figure 2.Timeline of HKSAR government interventions during the fifth wave of the COVID-19 pandemic in 2022.
Note: The yellow boxs indicate the anti-epidemic measures taken by the HKSAR government, while the green boxs represent the allocation of medical resources from the Chinese central government.
Abbreviation: HKSAR=Hong Kong Special Administrative Region; COVID-19=coronavirus disease 2019.
-
Twelve specific indicators (C1–C8, H2, H3, H7, and H8) were analyzed to assess their trends in HKSAR during different pandemic waves. Results depicted in Table 2 and Figure 3 show that during the first to fourth waves, only C2, C3, C7, and C8 had a significant correlation with incident cases. However, the Granger causality test revealed that interventions were not significantly related to incident cases during the fifth wave before medical aid (Table 2). These findings suggest that the previous measures were insufficient in controlling the surge in cases caused by the Omicron variant.
Factor Definition First-Forth wave
(January 1, 2020–April 30, 2021)The fifth wave
(December 1, 2021–Febuary 15, 2022)†Granger AIC days Granger AIC day C1 School closing 0.43 1 0.92 1 C2 Workplace closing 0.88 1 N/A 1 C3 Cancel public events 0.75 1 0.26 1 C4 Restrictions on gatherings 0.98 1 0.95 1 C5 Close public transport 0.27 1 N/A 1 C6 Stay at home requirements 0.32 1 N/A 1 C7 Movement restrictions 0.66 1 N/A 1 C8 International travel 0.0045* 1 N/A 1 H2 Testing policy 0.011* 1 N/A 1 H3 Contact tracing 0.16 1 N/A 1 H7 Vaccination policy 0.015* 1 N/A 1 H8 Protection of older adults 0.0002* 1 N/A 1 Note: N/A means that according to the VAR model, the indicator shows no significant correlation with incident cases.
Abbreviation: HKSAR=Hong Kong Special Administrative Region; VAR=vector autoregression.
* The P value from a Wald test was less than 0.05, suggesting that an increase in the predictor is linked with a reduction in infections.
† To assess the specific influence of HKSAR governmental actions on the fifth wave of the pandemic, data was analyzed from December 1, 2021 (one month prior to the outbreak) to February 15, 2022 (the day preceding medical intervention).Table 2. Results of the Granger causality test and Akaike information criterion (AIC) days for various waves of the pandemic in HKSAR.
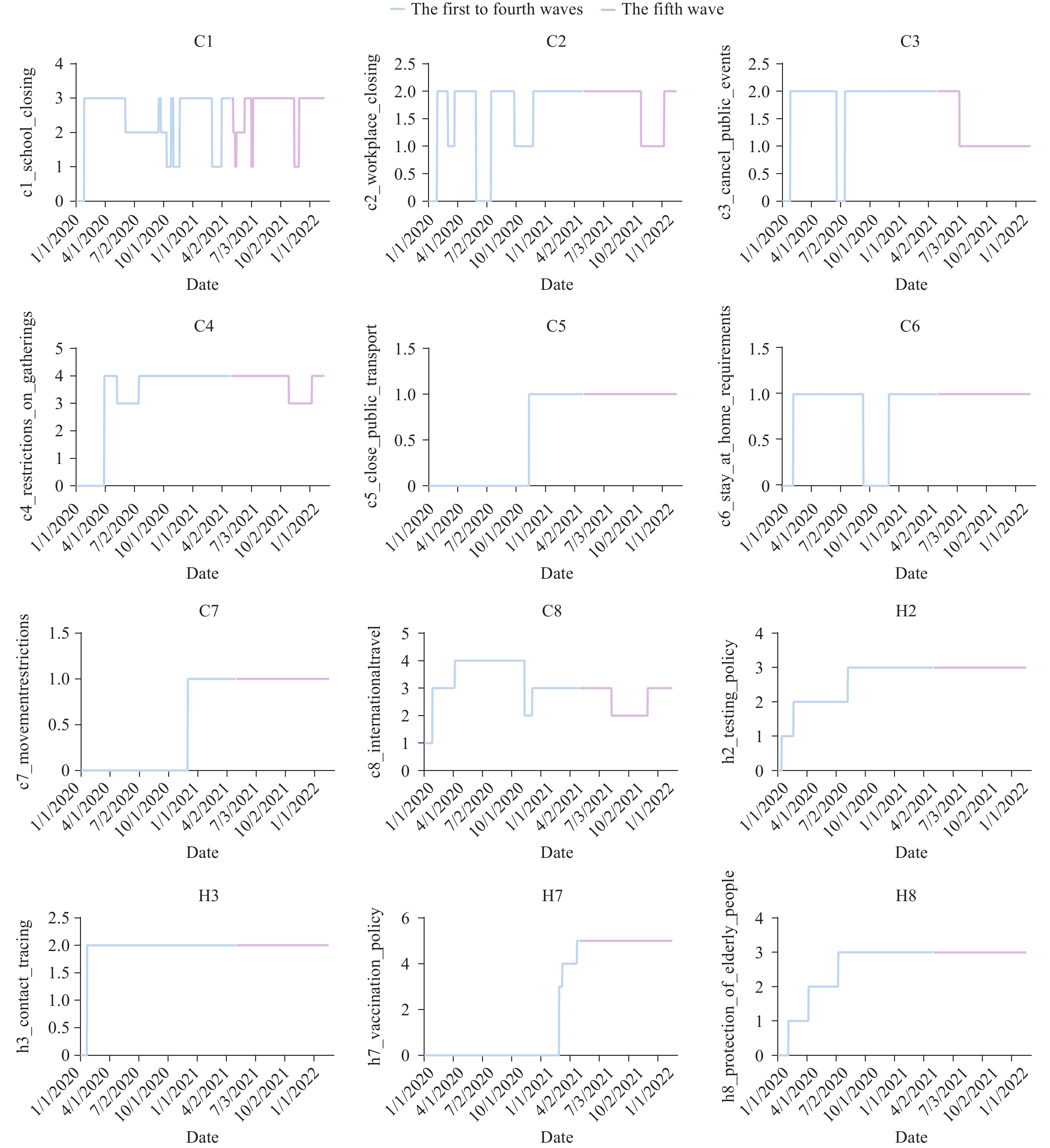 Figure 3.
Figure 3.Scores of indicators related to measures in the OxCGRT.
Note: The measures include School closure (C1), Workplace closure (C2), Cancellation of public events (C3), Restrictions on gatherings (C4), Closure of public transport (C5), Stay-at-home requirements (C6), Restrictions on internal movement (C7), International travel controls (C8), Testing policy (H2), Contact tracing (H3), Vaccination policy (H7), and Protection of older adults (H8). The blue line represents the period from the beginning of the COVID-19 pandemic (January 1, 2020) until before the onset of the fifth wave (December 30, 2022), while the purple line depicts the fifth wave of the COVID-19 pandemic.
Abbreviation: OxCGRT=Oxford COVID-19 Government Response Tracker; COVID-19=coronavirus disease 2019.
-
In the model without timely domestic medical resource allocation, the fatality rate increased through day 10, stabilizing at 1.07% by day 50 (Figure 4A). Conversely, with prompt deployment of domestic resources, the model projected a continual decrease in the death rate to 0.73% by day 30 (Figure 4B). The study compared actual and predicted fatality rates under scenarios with or without domestic medical resource deployment through a modified transmission dynamics model. Without timely domestic resource allocation, the maximum cumulative fatalities were estimated at 12,057 [95% confidence interval (CI): 11,454, 12,660] (Table 3, Figure 5). Most infected individuals were aged over 80, comprising 8,563 cases (95% CI: 8,135, 8,992). Following the deployment of domestic medical resources, the projected maximum cumulative fatalities reduced to 9,917 (95% CI: 9,421, 10,413), indicating a 17.7% decrease, with 7,044 deaths in the over-80 age group (95% CI: 6,692, 7,396). Furthermore, with the inclusion of molnupiravir on February 22 and nirmatrelvir/ritonavir on March 15 in the model, the total deaths decreased to 8,851, showing a continuous 10.7% decline. Overall, the combined effect of domestic medical resources and COVID-19 oral medications led to a 26.6% reduction in the number of deaths.
 Figure 4.
Figure 4.Mortality simulations without or with medical resource provision. (A) without medical resource provision; (B) with medical resource provision in 2022.
Measures Age groups Number of fatality cases Actual data All age groups 9,094 Without medical resource distribution from Chinese mainland All age groups 12,057 (95% CI: 11,454, 12,660) <60 years 476 (95% CI: 452, 500) 60–79 years 3,018 (95% CI: 2,867, 3,168) >80 years 8,563 (95% CI: 8,135, 8,992) With medical resource distribution from Chinese mainland All age groups 9,917 (95% CI: 9,421, 10,413) <60 years 391 (95% CI: 371, 411) 60–79 years 2,482 (95% CI: 2,358, 2,606) >80 years 7,044 (95% CI: 6,692, 7,396) With medical resource distribution from Chinese mainland and oral drug All age groups 8,851 (95% CI: 8,408, 9,293) <60 years 350 (95% CI: 332, 366) 60–79 years 2,215 (95% CI: 2,104, 2,326) >80 years 6,286 (95% CI: 5,972, 6,601) Abbreviation: CI=confidence interval. Table 3. Number of fatalities simulated by the model among different age groups.
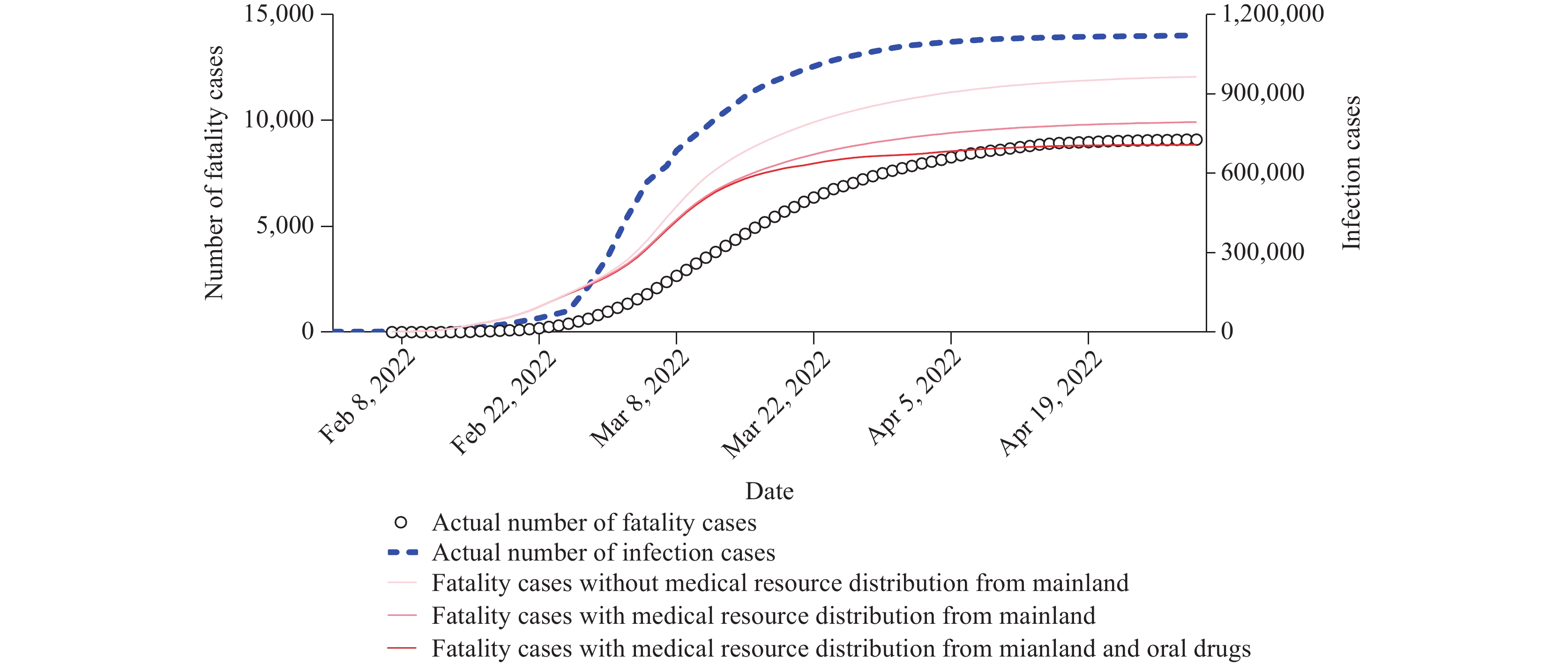 Figure 5.
Figure 5.Number of fatality cases under various scenarios.
Note: The actual fatality case data points were fitted onto the curve (circles).
The Fifth COVID-19 Pandemic in HKSAR
Evaluation of the HKSAR Government’s Efficacy in Combating Various Waves of the Pandemic
Effectiveness of Medical Resources and Oral Antiviral Drugs on Preventing Deaths
-
The Omicron variant is highly transmissible, with an estimated basic reproduction number (R0) of up to 8.2. Despite its high transmissibility, studies have shown that the Omicron variant predominantly causes mild upper respiratory tract infections with low pathogenicity, leading to mostly mild symptoms (10). By April 2022, the Omicron variant had spread to 166 countries and regions (11), contributing to a more severe fifth wave of the pandemic compared to previous waves. Previous interventions such as international travel restrictions, nucleic acid testing, contact tracing, vaccination strategies, and protection measures for older adults were effective during the initial four waves of the pandemic in the HKSAR. However, these measures became less effective during the fifth wave. Our study suggests that the timely allocation of domestic resources could significantly reduce deaths by 2,140, and the introduction of oral COVID-19 medications further decreased deaths by 1,066. The prompt deployment of resources from mainland China potentially reduced deaths among infected patients by 17.7%. Moreover, our model, which includes parameters for oral COVID-19 medications, aligns closely with actual trends. The utilization of oral drugs continued to reduce deaths among infected patients by 10.2%, particularly effective for severely ill patients. Stockpiling oral medications for SARS-CoV-2 infection, both in China and globally, is crucial for future management strategies.
By the end of 2022 and since 2023, globally prevalent strains include BQ.1, BQ.1.1, XBB, XBB.1, and XBB.1.5, alongside EG.5. Currently, EG.5, a variant derived from XBB.1.9.2, exhibits a spike protein amino acid profile shared with XBB.1.5. Notably, there is an additional F456L amino acid substitution in the spike protein of EG.5 compared to its precursor XBB.1.9.2 subvariant and XBB.1.5 (12).
The likelihood of secondary infections is expected to increase due to the enhanced transmissibility and immune evasion capabilities of emerging mutant strains, necessitating a reliance on targeted therapeutics. The primary treatment modalities for COVID-19 include therapeutic repurposing, monoclonal antibody therapy, convalescent plasma therapy, and drug development based on specific viral targets (13). Drug repurposing is a rapid and efficient approach, utilizing approved drugs for alternative indications, such as remdesivir, lopinavir/ritonavir, and hydroxychloroquine, including RAY 1216, to manage COVID-19 (14-15). Nonetheless, resistance to antiviral medications may develop due to mutations in viral proteins targeted by these drugs, suggesting that a combination of antiviral agents with different mechanisms of action might provide a viable treatment strategy for certain drug-resistant strains.
However, this study was subject to some limitations. It is challenging to differentiate the impact of the strengthening measures implemented by the government of HKSAR on the anticipated fatalities from mainland China’s resource allocation. Therefore, this study aims to objectively assess the outcomes of mainland China’s support for HKSAR and the policies implemented by HKSAR through a comprehensive observation of both factors.
The prompt allocation of medical resources in HKSAR and the use of appropriate medications could effectively reduce the mortality rate linked to Omicron infection.
-
No conflicts of interest.
-
Tong Wu for providing technical support in model building, the colleagues involved in the Oxford COVID-19 Government Response Tracker, as well as the epidemiological investigators, staff of local community offices, medical personnel, and volunteers for their dedicated efforts in assisting with outbreak control.
| Citation: |

|