
 Download:
Download:




-
Influenza, a highly contagious respiratory illness, is responsible for a substantial number of severe cases and respiratory-related deaths worldwide (1). The annual incidence of influenza in adults is estimated to be between 5% and 10%, while in children, it can be even higher, ranging from 20% to 30% (2). Infected children, who typically have a prolonged high viral load lasting up to two weeks, play a significant role in spreading the virus and leading to a greater number of secondary infections. This places a considerable socioeconomic and clinical burden on society (3).
Annual influenza vaccination is recommended by many countries to address antigenic drift and declining serum antibody levels over time (4). Research has indicated that, for children under 9 years with no prior vaccination, two doses of trivalent influenza vaccine offer higher protective efficacy compared to a single dose (5–7). The quadrivalent influenza vaccine (QIV) contains strains of influenza A/H1N1, A/H3N2, B/Yamagata, and B/Victoria. Studies have demonstrated that QIV exhibits comparable immunogenicity to trivalent influenza vaccine, but outperforms non-trivalent influenza B lineage (8). This study aims to assess the immunogenicity and safety of QIV with one or two doses in children aged 3 to 8 years in China while considering their influenza vaccination history.
In this open-label, self-paired clinical trial conducted in Donghai County, Jiangsu Province, China (ClinicalTrials.gov number: NCT05313893), we enrolled healthy children aged 3–8 years. The children were categorized into two groups based on their previous influenza vaccine history: Group A (received two or more doses) and Group B (never received). Please refer to
Supplementary Material for detailed inclusion and exclusion criteria. Each group received a two-dose regimen of the QIV on days 0 and 28. The QIV vaccine, manufactured by Changchun Institute of Biological Products Co., Ltd., is meant for seasonal influenza immunization in individuals aged 3 years or older. Each 0.5 mL dose contained 15 μg hemagglutinin for A/Victoria/2570/2019 (H1N1) pdm09, A/Cambodia/e0826360/2020 (H3N2), B/Washington/02/2019 (B/Victoria lineage), and B/Phuket/3073/2013 (B/Yamagata lineage). The trial was reviewed and approved by the Ethics Committee of the Jiangsu CDC, conducted following Good Clinical Practice Guidelines and the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants before enrollment.Blood samples were collected at three time points: baseline (referred to as day 0), day 28, and day 56, to quantify antibody titers. The quantification was performed at the China National Institutes for Food and Drug Control using a hemagglutination inhibition (HI) assay. The strains used for HI testing corresponded to the prevalent influenza strains for the season, which were also included in the vaccine composition. Following vaccination, participants were monitored for 30 minutes to identify any immediate reactions. Solicited local and systemic adverse events within 7 days, unsolicited adverse events within 28 days, and serious adverse events within 6 months after vaccination were also recorded. The severity of adverse events was assessed according to the “Guidelines for Grading Adverse Reactions in Clinical Trials of Preventive Vaccines.” The causal relationships between vaccination and adverse events were evaluated by an expert committee organized by Jiangsu CDC.
The primary endpoint for assessing immunogenicity included the measurement of geometric mean titers (GMT) of HI antibodies on day 0, day 28, and day 56, as well as the geometric mean fold increase (GMFI), seroprotection rate (SPR), and seroconversion rate (SCR) at 28 days post-vaccine dose. The SCR was defined as the percentage of participants meeting either of the following criteria: having a pre-vaccination HI titer <1∶10 and a post-vaccination HI titer ≥1∶40, or having a pre-vaccination HI titer ≥1∶10 and a minimum fourfold increase in post-vaccination HI titer. The primary safety endpoint was the occurrence of adverse reactions within 28 days following each vaccination. A post-hoc analysis was conducted to evaluate the combined effects of dose, sex, age, and baseline serostatus (seronegative if >1∶10, seropositive if ≤1∶10) on the antibody response providing protection.
The sample size calculation was performed to determine the number of participants needed in this study. It was based on the difference in SCR, with a non-inferiority margin set at 0.1 for the lower bound of the one-sided 97.5% confidence interval. Based on the results from a phase III clinical trial, the minimum observed SCR was 64.67%, which was rounded to 60% for conservative estimation. In order to achieve a testing power of 80% (1-β) and account for a dropout rate of 15%, a final determination was made to include approximately 120 participants per group for observation. Further details on additional statistical analysis plans can be found in
Supplementary Material . The statistical analysis was conducted using SAS (version 9.4; SAS Institute, Cary, NC).A total of 252 participants were included in the study, with 129 in Group A and 123 in Group B, enrolled from November 12 to December 30, 2021 (Figure 1). Among them, 16 participants were lost to follow-up, and 9 participants refused to provide blood samples. All 252 children who received at least one dose were included in the final safety analysis. Additionally, 227 children who completed two doses of vaccination and had two blood samples available were included in the immunogenicity analysis. The mean age of children in Group A was 6.00±1.00 years, while in Group B it was 5.00±2.00 years. The proportion of males was 48.06% (62/129) in Group A and 51.22% (63/129) in Group B (
Supplementary Table S1 ). Figure 1.
Figure 1.Inclusion and follow-up in analyses of immunogenicity and safety in two groups.
Note: Group A is classified as individuals who received two or more doses of influenza vaccine before the current season, while Group B is classified as individuals who have never received influenza vaccine in the past. Additionally, 25 participants dropped out after vaccination.Antibody responses were examined in Group A. Following the first dose, there was a significant increase in GMTs for all four strains: a fold increase of 8.51 for H1N1 (from GMTs: 672.19 to 79.02), 4.84 for H3N2 (from GMTs: 368.49 to 76.17), 8.15 for BY (from GMTs: 138.10 to 16.95), and 8.40 for BV (from GMTs: 132.29 to 15.74). However, after the second dose, Group A showed a slight decrease in H1N1 and BV strains, with a reduction of 0.92-fold [95% confidence interval (CI): 0.85, 0.99] and 0.86-fold (95% CI: 0.80, 0.93), respectively, compared to the response after the first dose. There were no notable differences in SCR and SPR between the first and second doses, except for a slight increase in SCR for BY strains after the second dose (P=0.039) (Table 1).
Statistic GMT T (95% CI) GMFI (95% CI) SCR (95% CI) SPR (95% CI) Pre-vaccination 28-day
post-dose 128-day
post-dose 228-day
post-dose 1*28-day
post-dose 2†28-day
post-dose 1*28-day
post-dose 2 *P value 28-day
post-dose 1 *28-day
post-dose 2 *P value Group A A(H1N1) 79.02
(62.10, 100.57)672.19 (581.95, 776.42) 616.87
(540.36, 704.22)8.51
(6.69, 10.82)0.92
(0.85, 0.99)82.30
(74.00, 88.84)77.88
(69.10, 85.14)0.063 100
(96.79, 100)100
(96.79, 100)1 A(H3N2) 76.17
(63.26, 91.71)368.49
(291.52, 465.77)323.95
(267.92, 391.7)4.84
(3.79, 6.18)0.88
(0.75, 1.03)57.52
(47.87, 66.77)55.75
(46.11, 65.09)0.824 97.35
(92.44, 99.45)99.12
(95.17, 99.98)0.500 BY 16.95
(14.24, 20.16)138.10
(113.99, 167.30)138.95
(119.75, 161.22)8.15
(6.69, 9.93)1.01
(0.91, 1.11)76.99
(68.13, 84.39)84.07
(76.00, 90.28)0.039 91.15
(84.33, 95.67)96.46
(91.18, 99.03)0.070 BV 15.74
(13.36, 18.56)132.29
(111.01, 157.66)114.18
(97.10, 134.27)8.40
(6.92, 10.20)0.86
(0.80, 0.93)84.07
(76,.00, 90.28)79.65
(71.04, 86.64)0.125 96.46
(91.18, 99.03)93.81
(87.65, 97.47)0.250 Group B A(H1N1) 26.13
(20.93, 32.63)533.29
(387.90, 733.16)791.77
(679.33, 922.83)20.41
(15.93, 26.13)1.48
(1.04, 1.31)88.60
(81.29, 93.79)94.74
(88.90, 98.04)0.039 96.49
(91.26, 99.04)100
(96.82, 100)0.125 A(H3N2) 34.57
(29.17, 40.97)283.36
(202.79, 395.94)321.95
(260.09, 398.53)8.20
(6.26, 10.73)1.14
(0.94, 1.38)72.81
(63.67, 80.72)91.23
(84.46, 95.71)<0.001 79.82
(71.28, 86.76)98.25
(93.81, 99.79)<0.001 BY 10.00
(8.55, 11.70)70.84
(54.58, 91.94)152.40
(132.52, 175.26)7.08
(5.8, 8.66)2.15
(1.74, 2.66)68.42
(59.05, 76.81)94.74
(88.90, 98.04)<0.001 71.05
(61.81, 79.16)99.12
(95.21, 99.98)<0.001 BV 10.25
(8.70, 12.07)62.35
(45.29, 85.84)97.78
(78.45, 121.87)6.09
(4.89, 7.58)1.57
(1.33, 1.84)54.39
(44.79, 63.74)85.96
(78.21, 91.76)<0.001 57.02
(47.41, 66.25)88.60
(81.29, 93.79)<0.001 Note: Group A refers to individuals who have received two or more doses of influenza vaccine prior to the current season, while Group B refers to individuals who have never received influenza vaccine in the past.
Abbreviation: GMT=geometric mean titer; GMFI=geometric mean fold increase based on a reference; SCR=seroconversion rate; SPR=seroprotection rate; CI=confidence interval.
* Reference is made to pre-vaccination antibody levels.
† Reference is made to post-dose 1 antibody levels.Table 1. Geometric mean titers, geometric mean fold increase, seroconversion rate, seroprotection rate, and 95% confidence intervals before and after vaccination in two groups.
Antibody responses were observed in Group B. The GMTs increased significantly after the first dose for H1N1 (533.29 to 26.13, fold change=20.41), H3N2 (283.36 to 34.57, fold change=8.20), BY (70.84 to 10.00, fold change=7.08), and BV (62.35 to 10.25, fold change=6.09). After the second dose, Group B showed slight increases in H1N1, BY, and BV strains with fold changes of 1.48 (95% CI: 1.04, 1.31), 2.15 (95% CI: 1.74, 2.66), and 1.57 (95% CI: 1.33, 1.84) compared to the first dose, respectively. For H3N2, BY, and BV strains, both SCR and SPR consistently increased after the second dose compared to the first dose (P<0.001) (Table 1).
In a multivariate analysis adjusting for age, sex, number of doses, and baseline serostatus, we found that baseline serostatus significantly impacts antibody titers against four influenza virus strains. Regardless of the dosage, individuals who were seropositive at baseline consistently exhibited higher antibody titers compared to those who were seronegative. Specifically, children who were seropositive at baseline had significantly higher HI GMTs after the first dose compared to children who were seronegative at baseline after the second dose. Therefore, a stratified analysis based on baseline serostatus was conducted in both groups to examine GMTs, SCR, and SPR indicators. Among seronegative individuals before vaccination in Group B, the second dose showed higher GMT, SCR, and SPR compared to the first dose (P<0.001). However, no statistically significant differences were observed in seropositive individuals (
Supplementary Tables S2 –S3 ).Both groups demonstrated good tolerability to QIV after each dose. In the 28-day period following administration of two doses, the overall incidence of adverse reactions in Group A and Group B was 38.8% (50/129) and 22.5% (29/123) respectively. Within 7 days after the first dose, the overall incidence of solicited adverse reactions in Group A and Group B was 31.8% (41/129) and 16.3% (20/123) respectively. Within 7 days after the second dose, the incidence of solicited adverse reactions in Group A and Group B was 16.7% (20/120) and 10.9% (13/119) respectively. It was observed that the incidence of solicited adverse reactions at 28 days after the second dose in Group A was lower than that observed at 28 days after the first dose (P<0.05). Adverse reactions were mainly grade 1 and grade 2, with pain at the injection site as the main local adverse reaction and cough as the main systemic adverse reaction (Figure 2). The incidence of Grade 3 adverse reactions was fever, 0.8% (1/129) in Group A and 1.6% (2/123) in Group B. No serious adverse events were reported during the trial.
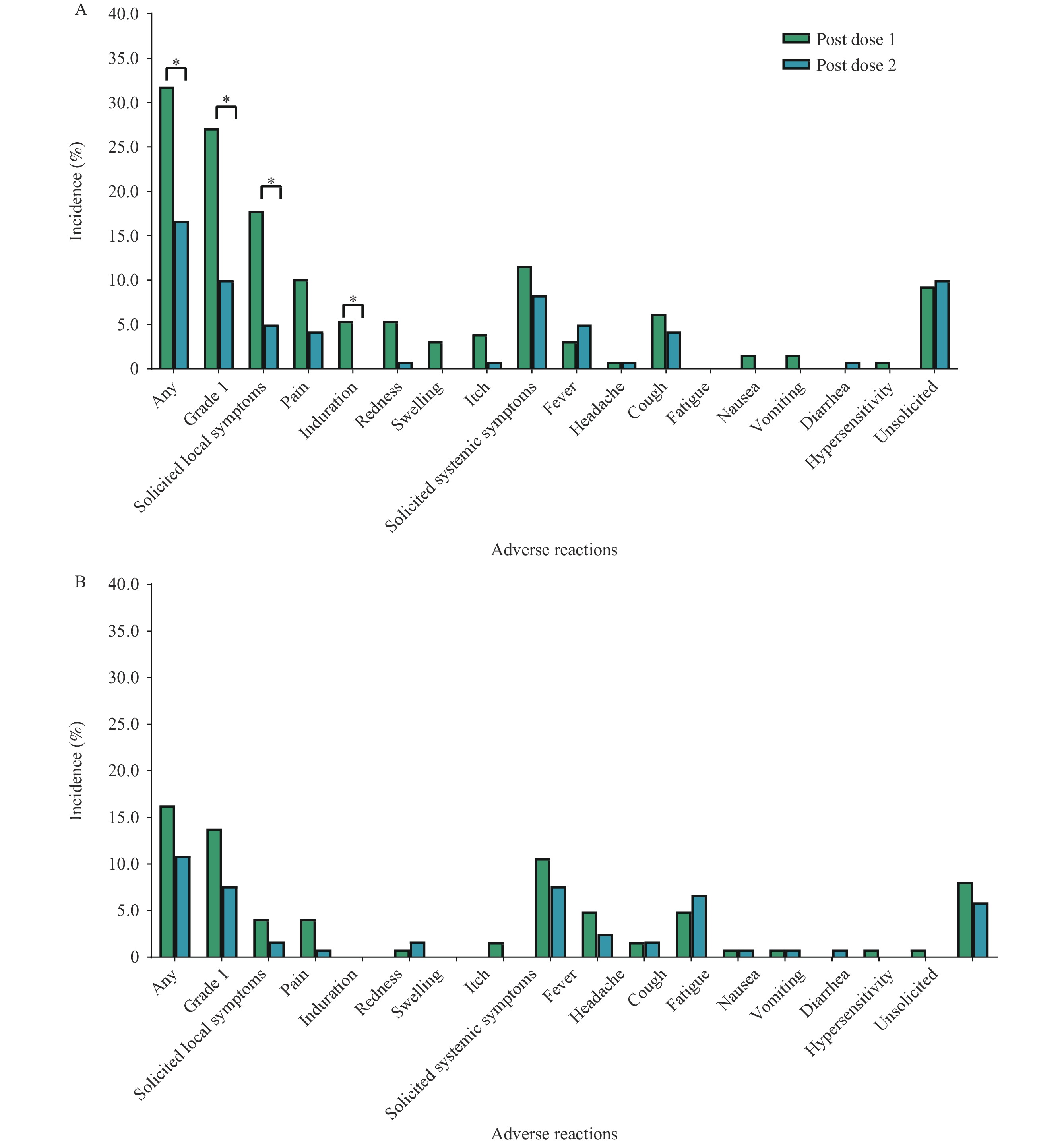 Figure 2.
Figure 2.Incidence of adverse reactions within 28 days after each vaccine in two groups. (A) Incidence of adverse reactions within 28 days after each vaccine in Group A; (B) Incidence of adverse reactions within 28 days after each vaccine in Group B.
Note: Adverse reactions in this context refer to any adverse events associated with the vaccination. The x-axis represents the different types of adverse reactions, while the y-axis represents the incidence of these reactions. The P value for comparing the incidence of adverse reactions between different doses is statistically significant (P<0.05). Group A refers to individuals who have received two or more doses of influenza vaccine in previous seasons, while Group B refers to individuals who have never received the influenza vaccine before. -
Our study demonstrated that Group A, comprising individuals who received two or more doses of influenza vaccines prior to the study, exhibited robust immune responses after the first dose, with GMFIs ranging from 4.84 to 8.51. However, there was a slight decrease in antibody titers against H1N1 and BV following the second dose, while there was no significant change in antibody titers against H3N2 and BY. The second dose did not confer any additional benefits in terms of SCR and SPR for all four viral strains, as the SPR after the first dose was already at least 93.81%.
In contrast, Group B, which consisted of individuals without a vaccination history, also exhibited high antibody titers after the first dose, with GMFIs ranging from 6.09 to 20.41. Following the second dose, antibody titers against H1N1, BY, and BV further increased, with GMFIs ranging from 1.48 to 2.15 compared to post-dose 1 titers. The SPR and SPR against H3N2, BY, and BV were higher after the second dose compared to the first dose. The SPR against BV consistently remained the lowest after each dose, but it did increase from 55.02% to 88.50%.
Additional analysis based on the initial serostatus revealed that the disparities between the two dosage levels were primarily observed in individuals who tested negative for B-type strains before vaccination. Particularly, among seronegative individuals with pre-vaccination serum antibody titers less than 1∶10, administering two doses of the QIV led to a significant elevation in antibody titers against all four viral strains. Our findings endorse the recommendation of administering two doses of QIV to unvaccinated children who have never received an influenza vaccine and are seronegative for maximum protection against B-type influenza viruses.
Differences in immune responses between two doses mainly stem from seronegative individuals in vaccine-naive children. It is hypothesized that these individuals may not have the prior exposure to the antigens that naturally or artificially induce immune memory. Previous studies have indicated that an individual’s history of influenza infection can greatly influence the formation of immune memory and the effectiveness of vaccination (9). This suggests that immune system imprinting is involved in conferring protection against specific viral strains. As a result, individuals may display diverse immune responses when exposed to either influenza infection or vaccination.
One limitation of this study is the failure to investigate the durability of immune responses following vaccination. Although we examined immune responses at day 28 after each vaccination, we did not evaluate their persistence over time. For a more comprehensive understanding of how immune responses evolve over time, in relation to the seasonal prevalence of influenza viruses, it would have been ideal to randomly assign participants to two groups: one receiving one dose and the other receiving two doses of the QIV. This approach would have allowed for a comparison not only of immediate immune responses but also their long-term durability. The other limitation is that we did not assess vaccine efficacy. While previous research has established a correlation between antibody titers and influenza protection, further validation through real-world studies is necessary.
In conclusion, for children aged 3 to 8 years who have previously received two or more doses of the influenza vaccine, a single dose of the seasonal influenza vaccine each year may be sufficient for protection. However, it is recommended that children who have never been vaccinated complete a two-dose immunization regimen, particularly for influenza B.
-
The quadrivalent influenza vaccine used in the trial was supplied by Changchun Institute of Biological Products Co., Ltd. W.J., X.G., XH.W., and SX.Z. are employees of Changchun Institute of Biological Products Co. No other conflicts of interest.
HTML
| Citation: |

|