
 Download:
Download:




-
Hepatitis B virus (HBV) infection is a significant global public health concern (1). According to the World Health Organization (WHO), in 2019, an estimated 296 million individuals worldwide had chronic hepatitis B, with 1.5 million new cases reported annually and approximately 820,000 deaths (2). In China, universal hepatitis B vaccination for newborns was introduced in 1992, resulting in a high vaccination rate among university students. However, the antibody response to HBsAg (anti-HBs) decreases over time after vaccination (3). Additionally, university students are at a higher risk of HBV infection due to various factors such as tattoos, unprotected sexual contact, pierced ears, and accidental blood exposure to medical students. The WHO recommends booster vaccination for high-risk populations (4). However, there is a growing reluctance among individuals to receive recommended vaccinations (5). Despite this, there have been limited efforts to evaluate hepatitis B vaccine hesitancy among medical university students. This study was conducted among the class of 2017 at a medical university from April to June 2020, with a total of 1,003 students from different professions completing a questionnaire. The results illustrated that hepatitis B-related knowledge, attitudes, and practices had a negative impact on hepatitis B vaccine hesitancy. The findings from this study provide insights for developing a health education-based hepatitis B vaccination strategy.
A cross-sectional study was conducted in the class of 2017. Out of the 27 professions, nine were randomly selected for recruitment, and all students in those nine professions were included in the study. Prior to enrollment, written informed consent was obtained from all participants. A self-designed questionnaire, consisting of 15 questions on HBV knowledge, 15 questions on HBV attitudes, and 10 questions on practices (
Supplementary Table S1 ), was distributed through the Wenjuanxing platform. The questionnaire was administered on-site by trained investigators. Students were asked to independently complete the questionnaire. The internal consistency of the questionnaire, measured by Cronbach’s α, was determined to be 0.855, indicating good reliability.Hepatitis B knowledge was categorized into four dimensions based on their relevance to infectious disease epidemics among humans: etiological knowledge (EK), transmission route knowledge (TRK), prevention measures knowledge (PMK), and epidemic status knowledge (ESK). Each correct answer was scored 1 point, while incorrect or unclear answers received 0 points. Hepatitis B attitudes were assessed using a 5-point Likert scale, ranging from “very consistent” to “very inconsistent,” with scores of 5 to 1, respectively, indicating personal inclination. Questions 3, 4, 5, 12, 13, and 14 were reverse-scored. Hepatitis B practices were divided into two dimensions based on behavioral characteristics: health-seeking practices (HSP) and high-risk practices (HRP). A score of 1 point was given for “yes” responses to hepatitis B practice items, while “no” or “unknown” responses received 0 points. Knowledge, attitudes, and practices related to hepatitis B were classified into two groups based on the mean score.
In our study, “vaccine hesitancy” (VH) was defined as the participants’ response of “unsure”, “basically inconsistent”, or “very inconsistent” when asked about their willingness to be vaccinated against hepatitis B in the absence of detectable anti-HBs. This term was used to describe the hesitation towards receiving the hepatitis B vaccine.
The database was established using Microsoft Excel (version 2016; Microsoft Corp, Redmond, USA), and analyses were conducted using SAS (version 9.4; SAS Institute, Cary, NC, USA). The chi-square test was used to assess the difference between the groups with vaccine hesitancy and those without. Logistic regression analysis was employed to examine the associations between the independent variables and hepatitis B vaccine hesitancy. Independent variables with P<0.05 in the univariate analysis were included in the logistic regression model. Structural equation modeling (SEM) was performed using Amos software (web version 24.0; IBM, New York, USA) to elucidate the interrelationships between latent variables. The model parameters were estimated using maximum likelihood estimation.
A total of 1,012 students were contacted, and 1,003 students responded, resulting in a response rate of 99%. The respondents were predominantly female (75.37%), with a sex ratio of 0.33∶1. Among the respondents, the majority (n=961) were of Han ethnicity. The participants consisted of 747 medical professionals (74.48%) and 256 nonmedical professionals (25.52%) (Table 1).
Variables N Hepatitis B vaccine hesitancy Univariate analysis Yes (n=199) No (n=804) χ2 P value Gender 10.935 0.001 Male 247 (24.63) 67 (27.13) 180 (72.87) Female 756 (75.37) 132 (17.46) 624 (82.54) Locality <0.001 0.998 Urban 368 (36.69) 73 (19.84) 295 (80.16) Rural 635 (63.31) 126 (19.84) 509 (80.16) Ethnicity 0.851 0.356 Han ethnicity 961 (95.81) 193 (20.08) 768 (79.92) Other 42 (4.19) 6 (14.29) 36 (85.71) Medical Professional 9.766 0.002 Yes 747 (74.48) 131 (17.54) 616 (82.46) No 256 (25.52) 68 (26.56) 188 (73.44) Etiological knowledge 62.620 <0.001 Good mastery (≥1.82) 662 (66.00) 84 (12.69) 578 (87.31) Poor mastery (<1.82) 341 (34.00) 115 (33.72) 226 (66.28) Prevention measures knowledge 68.217 <0.001 Good mastery (≥1.44) 605 (60.32) 69 (11.40) 536 (88.60) Poor mastery (<1.44) 398 (39.68) 130 (32.66) 268 (67.34) Transmission routes knowledge 51.415 <0.001 Good mastery (≥5.12) 686 (68.39) 94 (13.70) 592 (86.30) Poor mastery (<5.12) 317 (31.61) 105 (33.12) 212 (66.88) Epidemic status knowledge 31.464 <0.001 Good mastery (≥0.57) 570 (56.83) 78 (13.68) 492 (86.32) Poor mastery (<0.57) 433 (43.17) 121 (27.94) 312 (72.06) Attitude toward the source of infection 45.103 <0.001 Inclusion (≥8.94) 630 (62.81) 84 (13.33) 546 (86.67) Stigmatization (<8.94) 373 (37.19) 115 (30.83) 258 (69.17) Life contact attitude 32.020 <0.001 Inclusion (≥18.12) 398 (39.68) 44 (11.06) 354 (88.94) Stigmatization (<18.12) 605 (60.32) 155 (25.62) 450 (74.38) Self-protection attitude 20.715 <0.001 Inclusion (≥8.04) 436 (43.47) 115 (26.38) 321 (73.62) Stigmatization (<8.04) 567 (56.53) 84 (14.81) 483 (85.19) Vaccine effect attitude 104.763 <0.001 Inclusion (≥9.99) 551 (54.94) 45 (8.17) 506 (91.83) Stigmatization (<9.99) 452 (45.06) 154 (34.07) 298 (65.93) Health-seeking practices 18.168 <0.001 More practices (≥1.06) 295 (29.41) 34 (11.53) 261 (88.47) Fewer practices (<1.06) 708 (70.59) 165 (23.31) 543 (76.69) High-risk practices 0.069 0.794 More practices (≥1.25) 376 (37.49) 73 (19.41) 303 (80.59) Fewer practices (<1.25) 627 (62.51) 126 (20.10) 501 (79.90) Table 1. Characteristics of university students with hepatitis B vaccine hesitancy [n (%)].
The Kaiser-Meyer-Olkin coefficient was found to be 0.785, indicating satisfactory sampling adequacy. Additionally, Bartlett’s test showed statistical significance (P<0.001), supporting the factor analysis. Based on eigenvalues, a total of four factors were extracted, explaining 69.54% of the cumulative variance. These factors were identified as attitude toward the source of infection (ASI), self-protection attitude (SPA), life contact attitude (LCA), and vaccine effect attitude (VEA).
A total of 199 respondents expressed hesitancy towards the hepatitis B vaccine, resulting in a vaccine hesitation rate of 19.84% (199/1,003). In the univariate analysis, significant associations were observed between vaccine hesitancy and factors such as knowledge, attitudes, and health-seeking practices (P<0.05) (Table 1).
The logistic regression model revealed that university students with lower TRK and PMK scores had a higher likelihood of hesitating to receive the hepatitis B vaccine (OR=1.947, 95% CI: 1.309, 2.897; OR=2.501, 95% CI: 1.682, 3.719). Participants who held stigmatizing attitudes toward the source of infection were 1.854 times more likely to hesitate in getting the hepatitis B vaccine compared to those with more inclusive attitudes (95% CI: 1.280, 2.684). Vaccine hesitancy was also associated with concerns about vaccine efficacy (OR=6.529, 95% CI: 4.417, 9.650). Furthermore, individuals who adopted fewer health-seeking behaviors were more likely to hesitate to receive the vaccine and had a 2.119-fold increased likelihood of adopting such behaviors (95% CI: 1.357, 3.308) (Table 2).
Variables β S $ {{\bar{{\boldsymbol{x}}}}} $ Wald χ2 OR (95% CI)* P value Transmission routes knowledge Good mastery 1 Poor mastery 0.666 0.203 10.801 1.947 (1.309, 2.897) 0.001 Prevention measures knowledge Good mastery 1 Poor mastery 0.917 0.203 20.492 2.501 (1.682, 3.719) <0.001 Attitude toward the source of infection Inclusion 1 Stigmatization 0.617 0.189 10.686 1.854 (1.280, 2.684) 0.001 Life contact attitude Inclusion 1 Stigmatization 0.663 0.210 10.002 1.940 (1.287, 2.925) 0.002 Vaccine effect attitude Inclusion 1 Calculation 1.876 0.199 88.573 6.529 (4.417, 9.650) <0.001 Health-seeking practices More behaviors 1 Fewer behaviors 0.751 0.227 10.913 2.119 (1.357, 3.308) 0.001 Abbreviation: OR=odds ratio; CI=confidence interval.
* Adjusted by Gender, Medical Professional, epidemic status knowledge, and self-protection attitude.Table 2. Multivariate analysis of hesitancy towards hepatitis B vaccine among university students.
SEM was developed using the knowledge, attitude, and practice theory model as a basis. The initial model included knowledge-related latent variables as independent variables, attitude and behavior-related latent variables as mediators, and the observed variable VH as the dependent variable. Non-significant paths between latent variables in the hypothetical model (P>0.05) were removed and corrected using the correction index. Model fit measurements indicated that the revised model demonstrated a satisfactory fit, and the model was professionally interpreted. The reference standards for the fit indicators, as well as the fit indicators for the final model, are provided in
Supplementary Table S2 . A diagram of the standardized model can be seen in Figure 1. The values assigned to each variable in the revised model are presented inSupplementary Table S3 .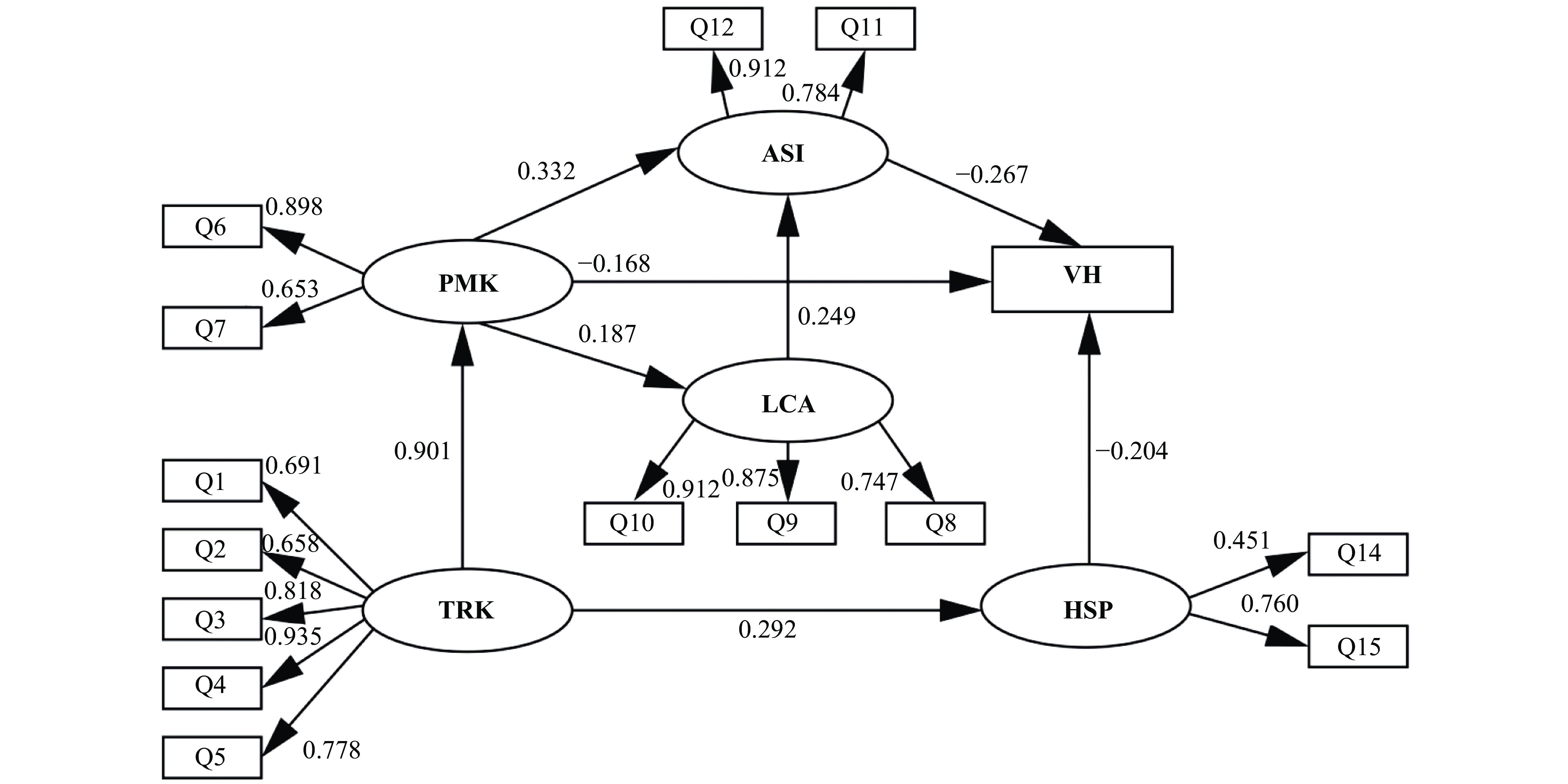 Figure 1.
Figure 1.Revised model (SEM).
Note: The ellipse and arrow in the structural model represent the effects of factors. One-way straight arrows in the structural model depict the paths of each factor with standardized regression weights, and one-way straight arrows in the measurement model show the measurement loadings of each item in the scale.
Abbreviation: PMK=prevention measures knowledge; ASI=attitude toward the source of infection; PMK=prevention measures knowledge; VH=vaccine hesitancy; LCA=life contact attitude; TRK=transmission route knowledge; HSP=health-seeking practices.
Supplementary Table S4 presents the associations between different factors (TRK, PMK, ASI, HSP, LCA) and vaccine hesitancy for hepatitis B. TRK had an indirect effect on vaccine hesitancy [standard indirect effect (SIE)=−0.301]. PMK, on the other hand, influenced vaccine hesitancy through both direct and indirect effects (standard direct effect (SDE)=−0.168, SIE=−0.101). ASI (SDE=−0.267) and HSP (SDE=−0.204) only had direct effects on hepatitis B vaccine hesitancy. Additionally, LCA had an indirect effect on vaccine hesitancy (SIE=−0.066), and this relationship was partially mediated by ASI. The analysis also revealed a negative correlation between hepatitis B-related knowledge, attitudes, and practices, and vaccine hesitancy. Further details regarding the structural model parameters can be found inSupplementary Table S5 . These findings indicate the importance of health education that focuses on enhancing knowledge, attitudes, and practices related to hepatitis B, as part of an effective hepatitis B vaccination strategy. -
The survey results revealed that the rate of vaccine hesitancy for hepatitis B among university students was 19.84%, which was lower compared to other migrant workers (6). This difference may be attributed to the medical students’ curriculum, specifically their education on infectious diseases, which contributes to a more accurate comprehension of hepatitis B-related knowledge.
Previous research has indicated that being aware of vaccine-preventable diseases can encourage vaccination (7). Our study found that students who were hesitant about vaccines had significantly less knowledge about hepatitis B compared to students who were accepting of vaccines. SEM also showed that knowledge had an indirect impact on vaccine hesitancy. These results are consistent with previous studies, highlighting the importance of increasing awareness of hepatitis B-related knowledge among university students. This can be achieved through initiatives like campus-wide events and interdisciplinary curricula, which can help mitigate vaccine hesitancy.
Stigma presents a significant obstacle to the effective implementation of preventive measures against HBV infection (8). Our study found that students who expressed stigmatizing attitudes towards hepatitis B patients and carriers were more likely to hesitate in getting vaccinated against hepatitis B. These findings highlight the need for universities and government organizations to provide early and positive guidance to enhance student education and promote understanding of the transmission routes of HBV and other viruses, in order to reduce counterproductive stigmatization among university students.
A survey conducted by the WHO and UNICEF from 2014 to 2016 revealed that doubts regarding vaccine safety and concerns about potential side effects were significant factors contributing to vaccine hesitancy (9). Our study, consistent with previous research on vaccine hesitancy in other contexts (10), identified concerns about the effectiveness and safety of vaccines as crucial determinants for refusing vaccination or lacking the intention to receive it (OR=6.529). We observed that university students who exhibited worry towards the hepatitis B vaccine were more likely to demonstrate vaccine hesitancy, which can have a negative impact on vaccine confidence and communication with both their families and future patients. Thus, our findings underscore the importance of educating university students about the safety and effectiveness of vaccines, as well as raising awareness about the critical role vaccines play in disease prevention. These ongoing issues persistently contribute to confusion and uncertainty surrounding vaccines.
Risk factors associated with hepatitis B vaccine hesitancy among university students include inadequate knowledge, stigmatization of attitudes towards the source of hepatitis B infection, and lacking health-seeking behaviors. Poor understanding, unfavorable attitudes, and inadequate practices related to hepatitis B are associated with increased vaccine hesitancy. Therefore, prioritizing knowledge dissemination is crucial for the development of effective hepatitis B vaccination strategies. Implementing educational programs at universities plays a vital role in raising awareness about prevention and enhancing vaccine coverage among students.
Previous research has primarily examined hepatitis B vaccine hesitancy in migrant workers, with limited attention given to medical university students. However, understanding the factors influencing vaccine hesitancy among medical students and developing effective health education strategies is crucial. This study aimed to address this gap by evaluating hepatitis B vaccine hesitancy in a medical university setting.
This study was subject to some limitations. First, the study utilized closed-ended questions, which limited the students’ ability to provide nuanced insights into their knowledge, attitudes, and practices regarding hepatitis B. Second, this study was conducted in a single medical university, and therefore may not fully capture the current status and determinants of hepatitis B vaccine hesitancy among Chinese university students. Future surveys should include a more diverse range of universities to ensure a representative sample.
-
No conflicts of interest.
HTML
| Citation: |

|