

 Download:
Download:




-
Foodborne illnesses pose a persistent threat to global health, commonly manifesting as acute gastroenteritis due to infections spread via contaminated food or water (1). With the increasing globalization and complexity of our food networks, there is an imperative need for rapid and precise pathogen detection methods (2–3). This is especially true in Beijing Municipality, where the distinctive demography and environmental factors underscore the importance of employing advanced diagnostic techniques (4–6). In our investigation, we collected 1,011 stool specimens from patients with presumed foodborne illnesses at 28 health facilities within the city. Utilizing quantitative polymerase chain reaction (qPCR), we identified and enumerated 35 different foodborne pathogens. The findings revealed a significant incidence of Clostridium perfringens, Salmonella enterica, enterotoxigenic Escherichia coli (ETEC), and adenovirus. Remarkably, 71.22% of the samples exhibited multiple concurrent infections. It is crucial for public health officials to consider culture-independent diagnostic tests (CIDTs) for disease identification and the prevalence of co-infections, which will notably improve the monitoring, prevention, and management of foodborne diseases in metropolitan areas. From January 2022 to April 2023, we amassed a total of 1,011 stool specimens from patients diagnosed with foodborne diseases in 28 different hospitals across Beijing. These patients were identified as having a foodborne disease based on symptoms that included recurring watery stool, mucus-laden or bloody stool, or vomiting, occurring three or more times within a 24-hour span, and reported as potentially linked to food consumption. We categorized patients by age: children (≤5 years old), adolescents (6–17 years old), adults (18–64 years old), and seniors (≥65 years old).
Each patient provided a fresh fecal sample weighing 5 mg, preserved in Cary-Blair transport medium CM0935 (Oxoid, Basingstoke, Hampshire, United Kingdom) at 4 °C. The samples were then transported to a designated laboratory within 24 hours for nucleic acid extraction. Nucleic acids were extracted from the fecal samples at the laboratory using a rapid nucleic acid extraction instrument NE-02-K-96 (Guangzhou Baybio Bio-tech Co., Ltd. Guangzhou, Guangdong, China) and a commercially available extraction kit STNM-48-K (Guangzhou Baybio Bio-tech Co., Ltd. Guangzhou, Guangdong, China). Detection of foodborne pathogens was carried out using single qPCR, with specific primers and probes obtained from literature or custom-designed for this study. Details of the pathogens detected, along with their primer and probe sequences, qPCR cycling conditions, and templates are listed in
Supplementary Table S1 .Statistical analysis was conducted using SPSS software (version 20.0; IBM SPSS, Chicago, IL, USA). The frequencies of different pathogens among patients in various age groups were compared using χ2 and Fisher’s exact tests for dichotomous variables. A P-value of <0.05 was considered statistically significant.
A total of 1,011 eligible stool samples were collected, and nucleic acid extraction was successful for all samples. The detection rate for foodborne pathogens overall was 92.48% (935/1,011).
Clostridium perfringens had the highest positivity rate at 52.03% among the samples analyzed (Figure 1A), followed by Salmonella enterica, ETEC, and adenovirus with rates of 20.67%, 20.97%, and 19.88%, respectively. Enteropathogenic Escherichia coli (EPEC) and enteroaggregative Escherichia coli (EAEC) were also prevalent, detected in 19.49% and 15.13% of the samples. Pathogens found in 5% to 15% of the samples included Staphylococcus aureus (S. aureus), Campylobacter jejuni, Bacteroides fragilis, Clostridium difficile, rotavirus, Vibrio parahaemolyticus, Shigella/Enteroinvasive Escherichia coli. (EIEC), Cronobacter spp., Aeromonas spp., norovirus, and Vibrio cholerae. Co-infections were present in 71.22% (720/1,011) of the samples (Table 1). Most infections involved one, two, or three pathogens, with rare cases having up to nine pathogens detected. Some cases of co-infections involved seven to nine pathogens, as detailed in Table 1 along with the onset time of these cases. Pathogen combinations for all samples are presented in Table 1. Pathogens were undetectable in 7.52% of the samples.
 Figure 1.
Figure 1.Prevalence of 35 pathogens in patients with acute diarrhea from Beijing. (A) Frequency distribution of 35 pathogens detected among 1,011 patients with acute diarrhea; (B) Seasonal distribution of Staphylococcus aureus, Aeromonas spp., and norovirus in 1,011 patients with acute diarrhea.
Abbreviation: ETEC=enterotoxigenic Escherichia coli; EPEC=enteropathogenic Escherichia coli; EAEC=enteroaggregative Escherichia coli; STEC=Shiga toxin-producing Escherichia coli; EIEC=Enteroinvasive Escherichia coli.Pattern of infections Time of onset Cases (%) Nonuple infections 2 (0.20) Cronobacter spp. + Clostridium perfringens + STEC O157:H7 + STEC + Clostridium difficile + Salmonella enterica + EAEC + ETEC + adenovirus Aug-22 Clostridium perfringens + rotavirus + Salmonella enterica + EPEC + Cystoisospora belli + Vibrio parahaemolyticus + Yersinia enterocolitica + ETEC + adenovirus Aug-22 Octuple infections 4 (0.40) Cronobacter spp. + Staphylococcus aureus + Clostridium perfringens + sapovirus + Bacteroides fragilis + Campylobacter coli + Yersinia enterocolitica + ETEC Sep-22 Staphylococcus aureus + Clostridium perfringens + STEC O157:H7 + STEC + Campylobacter jejuni + Vibrio parahaemolyticus + Yersinia enterocolitica + adenovirus Sep-22 Clostridium perfringens + rotavirus + Salmonella enterica + Vibrio cholerae + EAEC + Campylobacter coli + ETEC + norovirus Aug-22 Clostridium perfringens + Clostridium difficile + Salmonella enterica + Campylobacter jejuni + Vibrio parahaemolyticus + Yersinia enterocolitica + ETEC + adenovirus Oct-22 Septuple infections 8 (0.79) Cronobacter spp. + Clostridium perfringens + Salmonella enterica + EPEC + Plesiomonas shigelloides + Yersinia enterocolitica + ETEC Sep-22 Cronobacter spp. + Clostridium perfringens + Campylobacter coli + Cystoisospora belli + Vibrio parahaemolyticus + ETEC + adenovirus Aug-22 Staphylococcus aureus + Clostridium perfringens + Aeromonas spp. + Clostridium difficile + Salmonella enterica + EAEC + Cyclospora cayetanensis May-22 Staphylococcus aureus + Clostridium perfringens + EAEC + Campylobacter jejuni + Vibrio parahaemolyticus + ETEC + adenovirus Oct-22 Clostridium perfringens + rotavirus + Salmonella enterica + Vibrio cholerae + EPEC + ETEC + adenovirus Aug-22 Clostridium perfringens + Aeromonas spp. + Clostridium difficile + EAEC + EPEC + Campylobacter jejuni + ETEC Oct-22 Clostridium perfringens + Shigella/EIEC + EAEC + EPEC + Arcobacter skirrowii + Arcobacter cryaerophilus + adenovirus Aug-22 Clostridium perfringens + EAEC + Campylobacter jejuni + Vibrio parahaemolyticus + ETEC + adenovirus + norovirus Oct-22 Sextuple infections 24 (2.37) Quintuple infections 64 (6.33) Quadruple infections 147 (14.54) Triple infections 211 (20.87) Duple infections 260 (25.72) Single infection 215 (21.27) Negative 76 (7.52) Total 1,011 Abbreviation: PCR=polymerase chain reaction; ETEC=enterotoxigenic Escherichia coli; EPEC=enteropathogenic Escherichia coli; EAEC=enteroaggregative Escherichia coli; STEC=Shiga toxin-producing Escherichia coli; EIEC=Enteroinvasive Escherichia coli. Table 1. Results of 1,011 stool samples from patients with foodborne diseases showing co-infections and infection patterns with 7–9 pathogens based on quantitative PCR experiments.
In spring, the prevalence of S. aureus was relatively low, increasing from summer onwards to peak at 33.33% in December (Figure 1B). Aeromonas spp. exhibited a higher positive rate during winter, whereas norovirus showed increased rates in winter and spring, except for December due to limited samples. Seasonal variations were not observed in other pathogens.
An analysis of pathogen positivity rates across different age groups revealed significant differences (Figure 2). Notably, children showed a higher positivity rate for adenovirus compared to adolescents and the elderly. EPEC presented elevated positivity rates in both children and adults when contrasted with elderly populations. S. aureus was more frequently detected in children and adolescents rather than in adult and elderly groups. C. difficile displayed increased positivity in both children and elderly individuals relative to adults. In contrast, V. cholerae was less commonly identified in children than in adults, and C. coli was found to have lower positivity rates in children as opposed to the other three age cohorts.
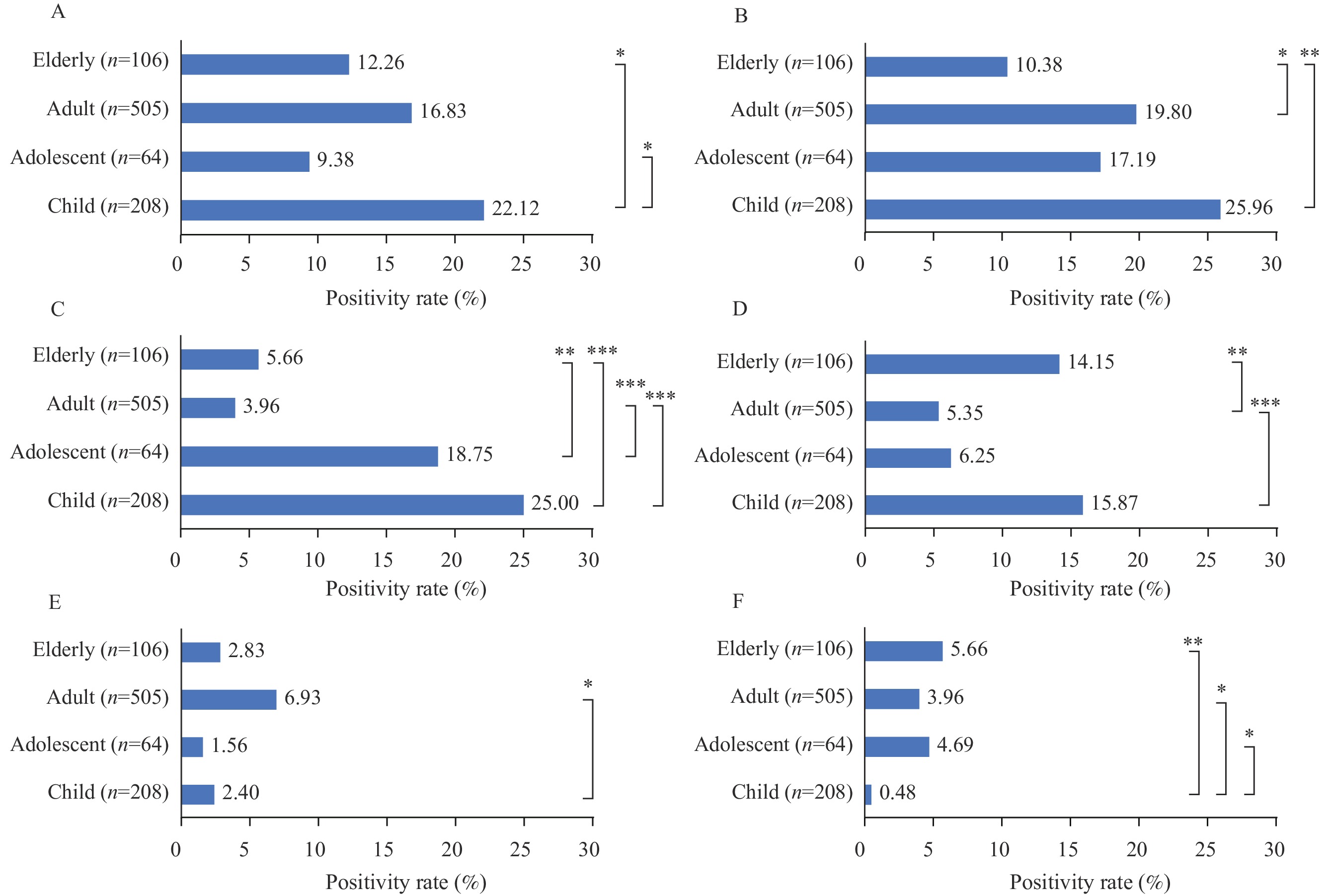 Figure 2.
Figure 2.Isolation rates (%) of six pathogens across different age groups: (A) adenovirus, (B) ETEC, (C) Staphylococcus aureus, (D) Clostridium difficile, (E) Vibrio cholerae, (F) Campylobacter coli.
Note: Because age data was missing for some patients during data collection, only 883 samples were included in this analysis.
* P<0.05.
** P<0.01.
*** P<0.001.
-
In this study, we performed multipathogen testing on stool specimens from 1,011 individuals presenting with foodborne illness in Beijing to characterize the prevalence and diversity of pathogens implicated. Our analysis revealed a notable incidence of coinfections, which underscores the specific challenges and food safety vulnerabilities faced by the city. We observed a considerably high positivity rate for C. perfringens. However, this finding warrants a careful interpretation. Although traditionally associated with the consumption of improperly cooked or stored meats, C. perfringens has been found in 21.2%–36.0% of healthy individuals (7). Therefore, while the detection of C. perfringens is of interest, it does not invariably suggest a pathogenic role in each instance. This finding highlights the critical need to differentiate between true pathogens and commensal organisms within the gastrointestinal tract, offering insights for future efforts to identify bona fide pathogens.
The significant positivity rates for Salmonella enterica, ETEC, and adenovirus align with findings from other surveillance studies (8), indicating broad contamination sources, likely spanning from water sources to diverse food items. Elevated adenovirus detection in children underscores their susceptibility, highlighting the need for precise identification of adenovirus serotypes and tailored preventive measures in environments where children are commonly present (9).
The variations in seasonal patterns, including the increase in S. aureus rates from summer to December and the elevated rates of Aeromonas spp. and norovirus in winter and spring, highlight potential environmental triggers or behavioral patterns that could impact these trends.
Differences in pathogen prevalence across age groups are crucial for understanding disease prevention. Higher adenovirus rates in children may indicate age-specific exposure or susceptibility. A study of 1,715 children demonstrated a high adenovirus positivity rate (10). Variances in C. difficile and other pathogen positivity rates by age imply age-related vulnerabilities or exposure routes.
The significant prevalence of coinfections raises interesting inquiries. When various pathogens are present in one host, identifying the main contributing pathogen to the clinical symptoms is difficult. It is crucial to investigate whether one pathogen is predominantly responsible for the symptomatic manifestation or if the combined effects of multiple pathogens worsen the severity of the disease. Unraveling this intricate interaction is a key focus for future research endeavors.
The study demonstrates the diverse diagnostic capabilities of qPCR-based molecular technology. It is suggested to integrate qPCR into pathogen surveillance for foodborne diseases and utilize it alongside epidemiological and clinical data to effectively inform public health interventions and policy modifications concerning foodborne disease surveillance.
This study is subject to some limitations. The analysis was solely reliant on CIDTs, and over half of the collected samples originated from adult participants, resulting in a lower representation of other age groups. Additionally, the sample collection intervals were not consistently distributed.
Despite these constraints, the sample sizes were adequate to identify trend patterns. To the best of our understanding, this is the most extensive survey of its kind conducted in China to date. We plan to extend our sample collection efforts and conduct concordance assessments between CIDT results and traditional culture methods. Furthermore, we will investigate the prevalence of various pathogenic sequences, including Clostridium perfringens, using metagenomic sequencing. Our future work will also involve contrasting the gut microbiota community structures of individuals with foodborne illnesses and those in good health, with the aim of informing more sophisticated strategies for the prevention and management of foodborne diseases.
-
No reported conflicts.
-
Thank the Beijing Changping, Chaoyang, Daxing, Fangshan, Fengtai, Haidian, Huairou, Mentougou, Shijingshan, and Xicheng Centers for Disease Control and Prevention for providing fecal samples.
HTML
| Citation: |

|