
 Download:
Download:




-
Infectious diseases are the largest threat to human health and cause a significant reduction in life expectancy (1). Vaccination has proven to be the most effective way to decrease the incidence of infectious diseases and, correspondingly, increase average life expectancy (2). China’s immunization program has progressed rapidly and comprehensively over the last 70 years, resulting in significant improvements in public health and life expectancy — specifically, in terms of reductions in morbidity and mortality rates due to vaccine-preventable diseases (VPDs). This study aimed to investigate the trends in the number of cases reported and incidence rate of 9 VPDs from 1950 to 2021, as well as the trends in sero-prevalence of hepatitis B surface antigen (HBsAg) from 1980 to 2014, to understand the involving epidemiological patterns and overarching changes in VPDs at the national level. This study’s findings indicate that decreases in VPD incidence are most prominent among children under five years of age. In addition, the sharpest decrease occurred during the Expanded Program on Immunization (EPI) stage.
To complete this work, researchers obtained data on reported cases of 9 infectious diseases (diphtheria, hepatitis A, Japanese encephalitis, measles, meningitis, mumps, pertussis, polio, and rubella) from 1950 to 2003 from the Infectious Disease Statistical Report of the Centers for Disease Control and Prevention, China. The data from 2004 to 2021 were obtained from the National Notifiable Disease Reporting System (NNDRS). Population data from 1950 to 2021 were obtained from the Population Division in the Department of Economic and Social Affairs, United Nations (
https://population.un.org/wpp/ ).The major burden of hepatitis B virus (HBV) is chronic hepatitis B rather than acute hepatitis B; therefore, the prevalence of evidence of HBV infection is a key measure of HBV-related disease burden. This study obtained nationally representative serosurvey data for HBsAg from published scientific documents as evidence of chronic infection. There were 4 national serosurveys in China: one in 1980 (3), one in 1992 (4), one in 2006 (5), and one in 2014(6). These surveys covered ages 0–59 years in 1980, 1–59 years in 1992, 1–59 years in 2006, and 1–29 years in 2014. Given that a vaccine against hepatitis B became available in 1985 and was included in the National Immunization Program (NIP) in 2002 and in the EPI in 2008, serosurveys in 1980, 1992, 2006, and 2014 reflect the hepatitis B disease burden in the prevaccine, pre-NIP, NIP, and EPI stages, respectively, as defined below.
This study used Microsoft Excel 2019 (Microsoft Corporation, Redmond, WA, USA) to construct an analytic VPD incidence database and a statistical analysis system (SAS, version 9.4; SAS Institute, Inc., Cary, NC, USA) to perform the statistical analyses.
First, this study’s researchers divided the study period into four stages based on vaccine availability, history of disease control, and immunization strategy implementation: 1) the prenational immunization program (pre-NIP stage, 1950–1977), which was the period in which there was no national vaccination program; 2) the early-stage NIP (early NIP, 1978–1987), in which vaccines against measles, polio, diphtheria, tetanus, pertussis, and tuberculosis were incorporated into the NIP (in 1978) and when, with support from the government and international organizations, the vaccine cold chain system was established and nearly completed; 3) the late-stage NIP (late NIP, 1988–2007), in which vaccination coverage rates (VCRs) steadily increased toward a target of 85% at the provincial level by 1988, the county level by 1990, and the township level by 1995, and during which the hepatitis B vaccine was included in the NIP (in 2002); and 4) the expanded immunization program stage (EPI, 2008–2021), during which vaccines against mumps, rubella, JE, and invasive meningococcal disease were incorporated into the EPI (in 2008).
Between 1950 and 2021, 172,285,377 cases among the 9 study VPDs were reported in China, representing a cumulative average incidence of 230.8 per 100,000 people. Among these patients, 143,599,524 (83.35%) were diagnosed during the pre-NIP stage, 15,468,640 (8.98%) during the early NIP stage, 8,124,496 (4.72%) during the late NIP stage, and 5,092,717 (2.96%) during the EPI stage. The overall average incidences of these 9 VPDs were 701.01, 151.02, 32.98, and 26.43 per 100,000 for the pre-NIP stage, early NIP, late NIP, and EPI, respectively (Table 1).
VPDs Monitoring start (years) Pre-NIP (1950–1977) Early NIP (1978–1987) Late NIP (1988–2007) EPI (2008–2021) The number of cases Incidence
(/100,000)The number of cases Incidence
(/100,000)Decrease*
(%)The number of cases Incidence
(/100,000)Decrease
(%)The number of cases Incidence
(/100,000)Decrease*
(%)Diphtheria 1950 1,518,016 7.41 74,990 0.73 90.15 1,891 0.01 99.87 2 <0.01 100.00 Polio 1953 356,743 1.90 49,953 0.49 74.21 14,448 0.06 96.84 0 0 100.00 Pertussis 1950 30,083,436 146.86 4,323,810 42.21 71.26 190,689 0.77 99.48 104,385 0.54 99.63 Measles 1950 101,512,542 495.56 9,243,723 90.25 81.79 1,772,811 7.20 98.55 399,905 2.08 99.58 JE 1950 1,734,057 8.47 327,078 3.19 62.34 279,919 1.14 86.54 21,572 0.11 98.70 Meningitis 1950 8,394,730 40.98 1,449,086 14.15 65.47 114,327 0.46 98.88 3,331 0.02 99.95 Hepatitis A 1990 NA NA NA NA NA 4,547,133 20.30 NA 364,380 1.89 90.69† Mumps 2004 NA NA NA NA NA 1,042,052 19.87 NA 3,776,930 19.60 1.36† Rubella 2004 NA NA NA NA NA 161,226 3.07 NA 422,192 2.19 28.66† Abbreviation: VPD=vaccine-preventable disease; NIP=national immunization program; EPI=expanded immunization program; NA=not applicable.
* Decrease in incidence compared with the pre-NIP.
† Decrease in incidence compared with the late NIP.Table 1. Number of reported cases and incidence of nine vaccine-preventable infectious diseases in the overall population by immunization stage in China, 1950–2021.
This study then analyzed the incidences of the 9 VPDs in children under 5 years old using age data that were available from 1997 to 2021 (Table 2). As vaccines against diphtheria, hepatitis A, measles, pertussis, and polio were incorporated into the NIP before 2008, this study divided the examination period for these five diseases into two stages: the pre-EPI stage (1997–2007) and the EPI stage (2008–2021). Vaccines against JE, mumps, rubella, and meningitis were included in the EPI by 2008, so children under 5 years of age would therefore be covered by 2012. This study next divided the period for these diseases into a pre-EPI stage (2004–2012) and an EPI stage (2013–2021). Decreases in the incidences among children under 5 years old were observed for all the VPDs except for pertussis in the EPI stage compared with the pre-EPI stage. The incidence of pertussis increased to 63.77% in the EPI stage compared with the pre-EPI stage. The annual case numbers for children under 5 years old from 1997 to 2021 are presented in Figure 1.
VPDs Pre-EPI* EPI† The number of
cases decreaseIncidence
(/100,000)The number of
cases decreaseIncidence
(/100,000)Decrease
(%)Diphtheria 29 <0.01 0 0 100.00 Measles 370,648 40.38 221,956 18.33 54.60 Pertussis 41,669 4.54 90,016 7.43 −63.77 Polio 0 0 0 0 NA JE 16,123 1.92 881 0.13 93.37 Meningitis 2,385 0.28 296 0.04 84.95 Hepatitis A 97,983 10.67 29,603 2.44 77.10 Mumps 486,718 57.91 320,223 46.23 20.17 Rubella 79,538 9.46 6,590 0.95 89.95 Abbreviation: EPI=expanded program on immunization; VPD=vaccine-preventable disease; JE=Japanese encephalitis; NA=not applicable.
* Period from 1997 to 2007 for diphtheria, measles, pertussis, polio, and hepatitis A and from 2004 to 2012 for JE, meningitis, mumps, and rubella.
† Period from 2008 to 2021 for diphtheria, measles, pertussis, polio, and hepatitis A and from 2013 to 2021 for JE, meningitis, mumps, and rubella.Table 2. Number of reported cases and incidences of nine VPDs in children under 5 years old by immunization stage in China, 1997–2021.
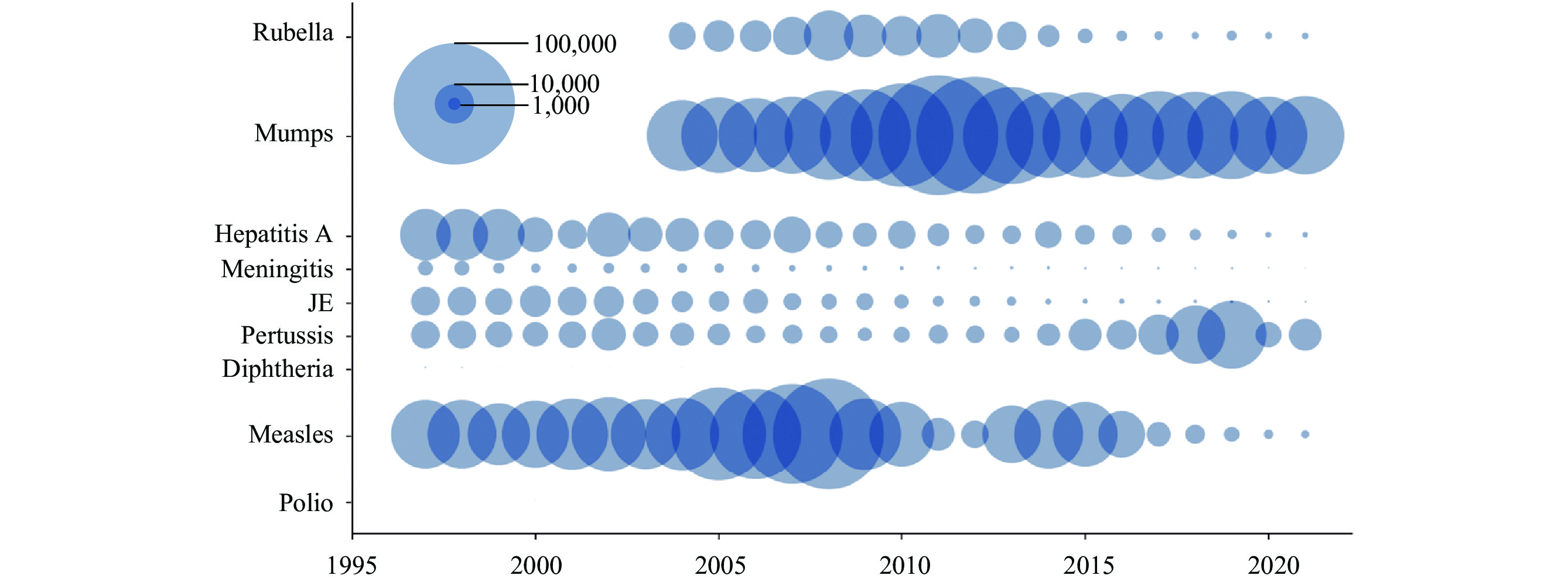 Figure 1.
Figure 1.Number of reported cases of nine VPDs in children under 5 years old, 1997–2021, represented as bubble diagrams.
Abbreviation: VPD=vaccine-preventable disease; JE=Japanese encephalitis.The seroprevalence of HBsAg was significantly lower in 2006 and 2014 than in 1980 and 1992, respectively. HBsAg seroprevalences among children aged 1–4 years were 9.24%, 9.67%, 0.96%, and 0.32% in 1980, 1992, 2006, and 2014, respectively (Figure 2).
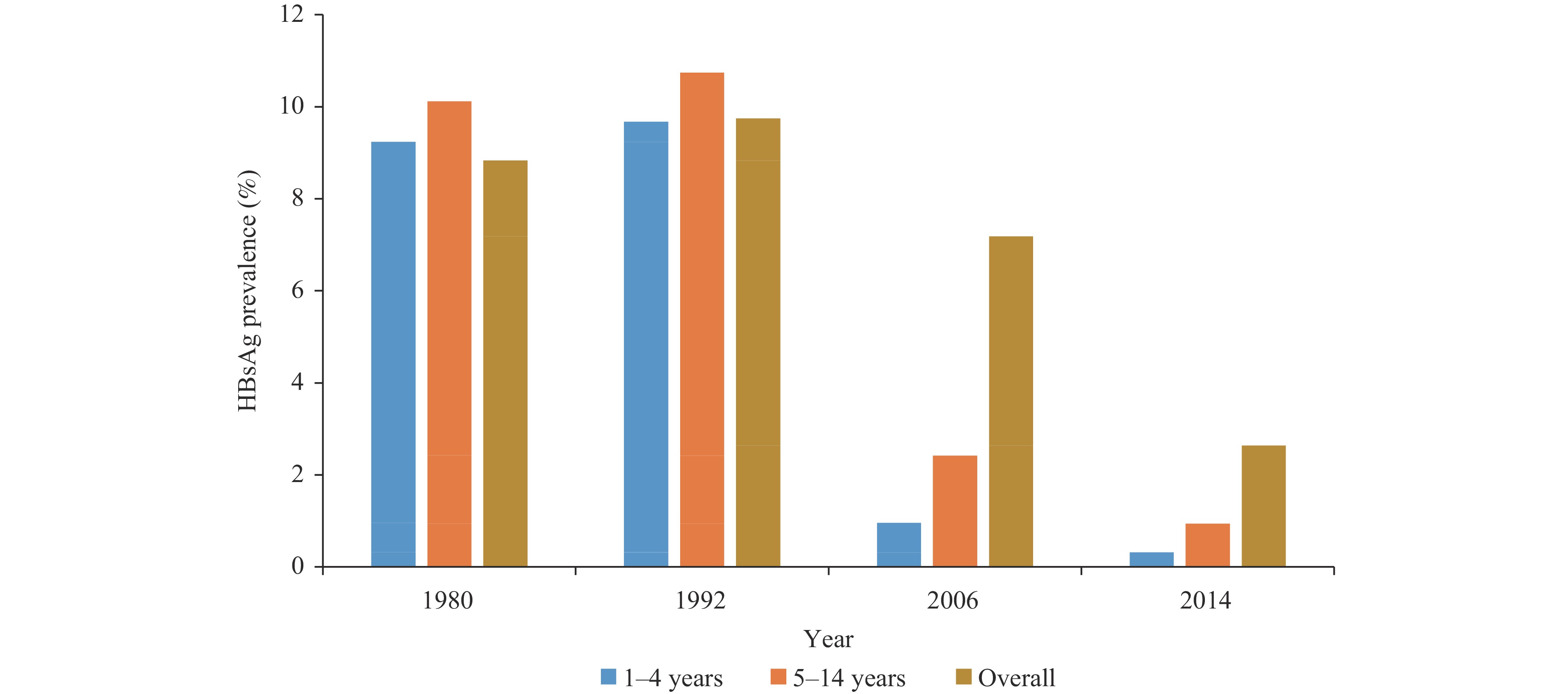 Figure 2.
Figure 2.HBsAg incidence in China from national serosurveys in 1980, 1992, 2006, and 2014.
Note: The sampled populations were 0–59 years, 1–59 years, 1–59 years, and 1–29 years in surveys conducted in 1980, 1992, 2006, and 2014, respectively.
Abbreviation: HBsAg=hepatitis B surface antigen.
-
This study explored patterns in case numbers and incidences of ten VPDs in China to evaluate the impact of different immunization strategies on the prevention and control of infectious diseases. Its findings showed that at the national level and within 72 years — from 1950 to 2021 — the annual case numbers and incidences of VPDs decreased significantly across all four stages of immunization, with particularly notable decreases in the late NIP and EPI stages. For measles, pertussis, diphtheria, JE, meningitis, and polio, there was a greater than 98% reduction in the incidence in the EPI stage. In contrast, the decreases in incidence of rubella and mumps were relatively small in the overall population, but there was a larger decrease in the incidences of these diseases in children under 5 years of age than in the overall population during the EPI stage. This could be explained by the EPI vaccination schedule, which included a target population of children under 5 years old.
This study’s researchers observed notable decreases in HBsAg incidence in different age groups in 2006 and 2014, revealing that increasing hepatitis B vaccine coverage, especially the timely birth dose, has played a major role in the dramatic reduction in HBsAg prevalence in China. These findings are consistent with subnational studies (7) and overseas studies (8). The introduction and implementation of the NIP and EPI increased vaccine coverage and are the predominant contributors to the dramatic reduction in the incidence of VPDs in China. The reported number of mumps cases has shown an increasing trend in recent decades. Yang and colleagues reported a similar trend of infectious disease incidence from 2004 to 2013 (9). Despite the modest decrease in the incidence of mumps during the EPI stage, remarkable decreases were achieved in the late NIP and EPI stages compared with the incidence in the 1990s, based on published data (451.57/100,000) (10). This modest decrease may be partially attributable to the improved sensitivity of the reporting system over time. Additionally, only the single-dose mumps-containing vaccine was included in the national EPI before 2020, and this suboptimal regimen would likely lead to a nonsignificant decrease in mumps. In cities where two-dose schedules were used, greater than 50% reductions in mumps incidences were observed in the two-dose era compared with the one-dose era. The low effectiveness of mumps vaccines due to waning immunity may also be a key contributor to the modest decreases in mumps incidence.
This study has several strengths. First, because its surveillance data spans up to 72 years, researchers were able to observe the impact of four different immunization strategies on VPDs at the national level. Second, this study was able to obtain age data, which allowed it to observe that decreases in incidence were most remarkable among children under 5 years of age.
However, this study also has several limitations. First, this study’s analyses are largely dependent on reported case data across decades. The quality and completeness of the reporting and reporting systems varied across the four stages. Second, although the Bacillus Calmette Guérin vaccine against tuberculosis was one of the first 4 vaccines incorporated into the NIP in 1978, tuberculosis data were not included in this study due to data availability. Finally, the declines in VPDs observed by this study may not be entirely dependent on vaccination and may reflect improved nutrition, health care, and living conditions. Future research should include additional factors to present a comprehensive assessment of the impact of immunization strategies on VPD control. Additionally, additional attention should be given to the full value of vaccines beyond the reduction of illness and death in future studies.
In conclusion, this study found that the implementation of immunization strategies significantly contributed to the decrease in incidence of VPDs in China. In particular, declines were observed during the most recent NIP stage because of the maintenance of a high VCR. VPD incidence declines were most prominent among the populations receiving the immunization strategy at the targeted ages. These findings indicate that a high VCR effectively controls the VPDs in the target population. Measures should be taken to maintain the VCR and optimize immunization strategies for VPDs that still circulate in the vaccine target population. Additionally, to better control the VPDs that were not included in the NIP, a holistic plan should be made to assess the feasibility of incorporating them.
-
No conflicts of interest.
-
We thank Dr. Lance Rodewald, National Immunization Program, Chinese Center for Disease Control and Prevention, for constructive comments on a draft of this manuscript and polishing language.
HTML
| Citation: |

|