
 Download:
Download:




-
Injuries pose a significant global challenge to the health and safety of children and adolescents (1). According to estimates by the Global Burden of Disease (GBD) study group, injuries caused 595,621 deaths and 233,114,563 incident cases worldwide among individuals aged 0–19 years in 2019. Of these, 6.5% of the deaths and 9.3% of the incident cases occurred in China (2).
The United Nations (UN) has outlined several Sustainable Development Goals (SDGs) pertinent to preventing injuries amongst children and adolescents (3). In the same vein, the Chinese central government promulgated a series of developmental outlines for children, and the current outline (2021–2030) sets an ambitious goal of a 20% reduction in child injury mortality by 2030 compared to 2020 (4).
To effectively mornitor the progress towards the specified targets in China, it is critical to regularly analyze nationwide data to discern patterns in child and adolescent mortality due to injuries. Several studies have documented trends in this field until 2020. Research by Luo et al. (5) analyzed the temporal progression of mortality due to injuries in children and adolescents aged 1–24 years, utilizing the Chinese Cause of Death Surveillance dataset spanning from 2010 to 2020. Zheng et al. (6) reported a notable reduction in mortality from drowning and road traffic crashes in children and adolescents aged 5–19 years between 2008 and 2019. Elevated injury mortality were reported occurring among boys, children, and early adolescents aged 5–14, and individuals residing in the western and rural areas. Yao et al. explored disparities in injury-induced mortality among children by gender and area (urban vs. rural) in Sichuan Province (7), but their findings were not nationally representative.
This study scrutinized nationally representative data to assess trends in overall injury mortality rates among Chinese children and adolescents (aged 0–19 years) from 2010 to 2021. In addition, we evaluated subgroup mortality rates according to demographic factors including area (rural vs. urban), sex, and age group.
-
This study sourced annual data on child and adolescent injury mortality from the Chinese Health Statistical Yearbook (2010–2021), which provides age-specific mortality data for 11 categories of unintentional and intentional injuries (8): motor vehicle crashes, non-motor vehicle crashes, poisoning, falls, fire/burn injuries, drowning, mechanical suffocation, falling object injuries, electric shocks, homicide, and suicide. To estimate the year-end population for each year from 2010 to 2021, we employed linear interpolation (9) using China’s census data of 2010 and 2020. The population data from 2020 was then utilized as the standard population for calculating age-standardized injury mortality.
Linear graphs were utilized to display variations in both overall and subgroup injury mortality, separated by area, gender, and age group for Chinese children and adolescents aged 0 to 19 years. Furthermore, stacked area charts were constructed to show the cause spectrum of child and adolescent injury mortality from 2010 to 2021, segmented by area and age group.
Significant injury mortality changes throughout the study time period were quantified using average annual percent change (AAPC) and annual percent change (APC), alongside their corresponding 95% confidence intervals (95% CIs), which were estimated via Joinpoint regression models. We used the Joinpoint Regression Program (Version 4.9.1.0, National Cancer Institute, Calverton, USA) to perform statistical analysis.
-
Between 2010 and 2021, the overall age−standardized injury mortality for children and adolescents in China decreased from 21.87 to 9.41 per 100,000 population (AAPC=−6.7%, 95% CI: −8.2%, −5.2%). The age−standardized injury mortality for urban children was continuously lower than and declined more slowly than that for rural children (urban−rural mortality ratio: 0.53 to 0.70; AAPC: −4.6% vs. −6.9%) (Figure 1A and Table 1). Injury mortality declined significantly during 2010−2021 in four age groups (under 1 year: AAPC=−7.9%, 1−4 years: AAPC=−11.6%, 5−9 years: AAPC=−7.5%, 15−19 years: AAPC=−3.6%), while significant decreases only occurred between 2013 and 2021 for the age group of 10−14 years (Figure 1B−F and Table 1).
 Figure 1.
Figure 1.Age-standardized and age-specific mortality rates for injuries among children and adolescents in various regions of China, from 2010 to 2021. (A) Age-standardized injury mortality rates in individuals aged 0–19 segmented by area. (B) Mortality caused by injuries in children under 1 year, differentiated by area. (C) Injury-caused mortality in children aged 1–4, broken down by area. (D) Injury-associated mortality in children aged 5–9, classified by area. (E) Mortality due to injuries in adolescents aged 10–14, outlined by area. (F) Injury mortality trends in adolescents aged 15–19, divided by area.
Age group Area Block 1 Block 2 Block 3 AAPC (95% CI) Time period APC (95% CI) Time period APC (95% CI) Time period APC (95% CI) All ages Total 2010–2021 −6.7 (−8.2, −5.2)* −6.7 (−8.2, −5.2)* Urban 2010–2021 −4.6 (−6.5, −2.6)* −4.6 (−6.5, −2.6)* Rural 2010–2021 −6.9 (−8.4, −5.5)* −6.9 (−8.4, −5.5)* 0–1 years Total 2010–2021 −7.9 (−9.7, −6.1)* −7.9 (−9.7, −6.1)* Urban 2010–2021 −7.2 (−9.7, −4.6)* −7.2 (−9.7, −4.6)* Rural 2010–2012 15.9 (−1.8, 36.8) 2012–2015 −14.1 (−27.3, 1.4) 2015–2021 −7.0 (−9.5, −4.3)* −5.3 (−9.0, −1.4)* 1–4 years Total 2010–2021 −11.6 (−14.1, −9.0)* −11.6 (−14.1, −9.0)* Urban 2010–2021 −8.8 (−11.1, −6.4)* −8.8 (−11.1, −6.4)* Rural 2010–2021 −11.7 (−14.6, −8.6)* −11.7 (−14.6, −8.6)* 5–9 years Total 2010–2021 −7.5 (−9.6, −5.3)* −7.5 (−9.6, −5.3)* Urban 2010–2013 −9.6 (−9.4, 32.6) 2013–2021 −8.6 (−12.3, −4.7)* −3.9 (−8.6, 1.0) Rural 2010–2014 −8.0 (−10.4, −5.6)* −8.0 (−10.4, −5.6)* 10–14 years Total 2010–2013 18.1 (6.7, 30.6)* 2013–2021 −5.4 (−7.5, −3.3)* 0.5 (−2.1, 3.2) Urban 2010–2013 17.0 (2.1, 34)* 2013–2021 −4.7 (−7.5, −1.9)* 0.7 (−2.8, 4.4) Rural 2010–2013 20.1 (8.1, 33.4)* 2013–2021 −5.3 (−7.4, −3.1)* 1.1 (−1.7, 3.9) 15–19 years Total 2010–2021 −3.6 (−5.9, −1.3)* −3.6 (−5.9, −1.3)* Urban 2010–2021 −2.1 (−4.8, 0.7) −2.1 (−4.8, 0.7) Rural 2010–2014 4.6 (−7.0, 17.7) 2014–2018 −11.1 (−26.2, −7.1) 2018–2021 1.5 (−15.7, 22.3) −2.2 (−8.5, 4.6) Abbreviation: APC=annual percent change; AAPC=average annual percent change; CI=confidence interval.
* P<0.05.Table 1. APC and AAPC in injury mortality among Chinese children and adolescents from 2010 to 2021.
-
Between 2010 and 2021, age-standardized injury mortality decreased from 28.52 to 11.24 per 100,000 population for boys, and decreased from 14.34 to 7.30 per 100,000 population for girls. The age-standardized injury mortality for boys was continuously higher than and declined faster than that for girls in both urban and rural areas (Figure 2A and Table 2).
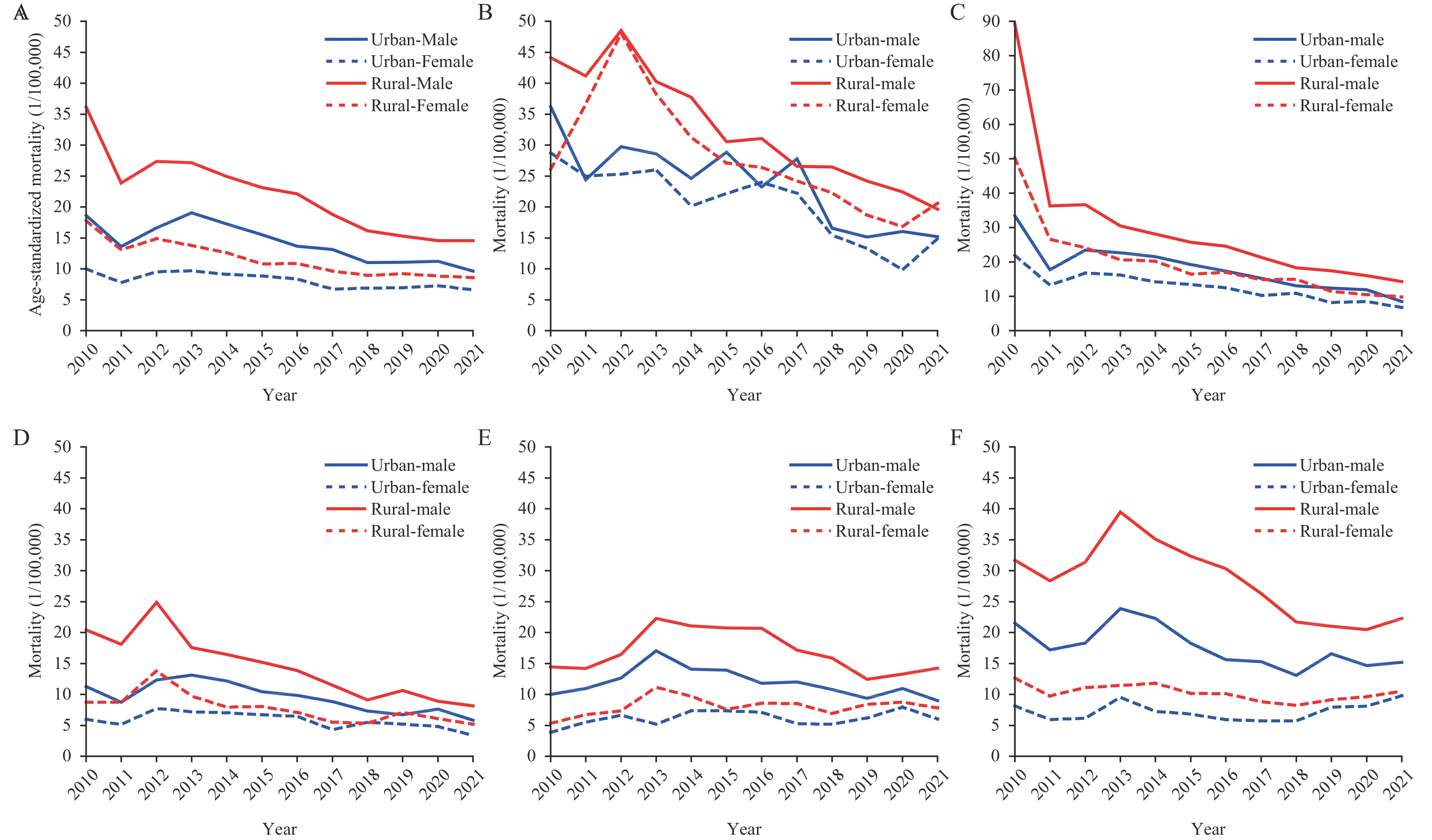 Figure 2.
Figure 2.Overall age-standardized and age-specific mortality rates due to injury among Chinese children and adolescents, categorized by sex and area, spanning the years 2010–2021. (A) Age-standardized injury mortality in children and adolescents aged 0–19, separated by sex and area. (B) Injury mortality in infants under one year of age, reported by sex and area. (C) Injury mortality in toddlers aged 1–4, delineated by sex and area. (D) Injury mortality in young children aged 5–9, categorized by sex and area. (E) Injury mortality in early adolescents aged 10–14, divided by sex and area. (F) Injury mortality in late adolescents aged 15–19, sorted by sex and area.
Age group Area Boys Girls Mortality in 2010 Mortality in 2021 AAPC (95% CI) Mortality in 2010 Motrality in 2021 AAPC (95% CI) All ages Total 28.52 11.24 −7.4 (−9.0, −5.7)* 14.34 7.30 −5.6 (−6.9, −4.2)* Urban 18.62 9.61 −5.3 (−7.4, −3.1)* 9.97 6.61 −3.4 (−5.1, −1.7)* Rural 36.14 14.53 −7.4 (−9.1, −5.8)* 17.75 8.56 −6.0 (−7.4, −4.7)* Under 1 year Total 41.05 16.82 −8.0 (−9.4, −6.6)* 27.15 16.96 −7.7 (−10.5, −4.8)* Urban 36.21 15.19 −7.0 (−9.7, −4.2)* 28.74 14.87 −7.5 (−10.5, −4.5)* Rural 44.15 19.62 −7.5 (−8.8, −6.2)* 26.10 20.58 −3.5 (−13.0, 7.0) 1–4 years Total 66.00 10.41 −11.9 (−14.7, −9.0)* 38.40 7.79 −11.0 (−13.1, −8.8)* Urban 33.42 8.51 −9.0 (−11.5, −6.4)* 21.93 6.79 −8.4 (−10.4, −6.2)* Rural 89.24 14.28 −11.9 (−15.2, −8.5)* 50.31 9.82 −12.8 (−15.9, −9.7)* 5–9 years Total 16.45 6.65 −8.3 (−10.3, −6.3)* 7.53 4.05 −5.9 (−8.7, −2.9)* Urban 11.29 5.80 −4.5 (−9.3, 0.6) 6.00 3.41 −4.3 (−7.6, −0.8)* Rural 20.42 8.14 −9.0 (−11.0, −6.9)* 8.71 5.16 −6.1 (−9.2, −2.8)* 10–14 years Total 12.49 11.08 −0.8 (−3.6, 2.1) 4.67 6.75 3.0 (−2.0, 8.2) Urban 10.02 8.99 −0.6 (−3.5, 2.3) 3.85 6.03 2.3 (−1.3, 6.2) Rural 14.45 14.21 −0.8 (−4.9, 3.5) 5.32 7.83 3.3 (−1.2, 8.0) 15–19 years Total 26.26 17.03 −4.8 (−7.1, −2.5)* 10.22 9.96 −0.9 (−3.8, 2.1) Urban 21.54 15.19 −3.5 (−6.0, −1.0)* 8.17 9.79 1.1 (−2.6, 5.0) Rural 31.67 22.28 −3.6 (−7.2, 0.2) 12.66 10.52 −2.1 (−4.0, −0.1)* Abbreviation: AAPC=average annual percent change; CI=confidence interval.
* P<0.05.Table 2. Mortality due to injuries and AAPC among Chinese children and adolescents, categorized by sex, from 2010–2021.
Subgroup analyses showed significant injury mortality decreases in three younger age groups for both sexes in both urban and rural areas (under 1 year, aged 1–4 years and aged 5–9 years, with AAPCs ranging from −12.8% to −4.3%), with exceptions for rural girls under 1 year and for urban boys aged 5–9 years old. Strikingly, overall and subgroup injury mortality by area and sex did not change significantly among early adolescents aged 10–14 years old. Significant reductions appeared only in urban boys (AAPC=−3.5%, 95% CI: −6.0%, −1.0%) and rural girls (AAPC=−2.1%, 95% CI: −4.0%, −0.1%) for the age group of 15–19 years (Figure 2B–D, Table 2, and
Supplementary Tables S1–S3 ). -
Supplementary Figure S1 depicts the distribution of the top six causes of injury-related deaths, segmented by age group and geographical area. Drowning and road traffic crashes were the predominant causes of injury-related mortality for the four older age groups. Among infants under the age of 1 year, suffocation emerged as the primary cause, accounting for 56.0%–76.7% of injury deaths during 2010–2021. Suicide has come to light as a significant cause of injury-related deaths among adolescents aged 10–19 years.During 2010–2021, significant injury mortality decreases were detected for suffocation among children under 1 year (urban: AAPC=−7.7%, rural: AAPC=−6.8%). Drowning mortality decreased significantly among children and adolescents aged 0–19 years (urban: AAPC=−8.0%, rural: AAPC=−9.5%). The overall and age-specific road traffic injury mortality reduced substantially since 2014 (e.g., 0–19 years, urban area: APC=−10.6%, rural area: APC=−10.2%). In contrast, notable suicide mortality increases were observed in the two oldest age groups for both urban and rural areas (with an AAPC changing between 4.7% and 11.5%) (
Supplementary Figure S1 andSupplementary Table S4 ). -
This study, using nationally representative data, analyzed current trends in injury mortality among Chinese children aged 0–19 years. The research produced four critical findings: First, the overall age-standardized injury mortality saw a decrease of 57% between 2010 and 2021. Second, the mortality rate due to injuries was comparatively higher in rural areas and among boys, with a faster decline rate than in urban areas and among girls. Third, the predominant cause of injury mortality differed by age groups, where unintentional suffocation was the leading cause of death for infants under one year and drowning was the main cause for the four older age groups. Lastly, suicide emerged as a leading cause of injury mortality among adolescents aged 10–19 years.
The significant decrease in injury mortality rates in Chinese children and adolescents over the past ten years are likely be attributed to two main factors. First, the reduction may symbolize the enormous efforts made by the Chinese government regarding injury prevention. As an instance, the implementation of changes to traffic laws — such as making drunk driving a criminal offense — has decreased traffic crash risks (10). Furthermore, the Chinese administration issued a variety of injury prevention guidelines and commenced education programs in schools across the country. These initiatives probably have a positive impact on child injury prevention.
Second, the notable decline in mortality due to injuries might be correlated with the swift urbanization throughout the nation. The percentage of Chinese residents residing in rural areas dropped from 48.17% in 2011 to 35.28% in 2021 (11). This could possibly lead to lower exposure to specific injury risks and hazards, such as drowning, for children.
Our results corroborate earlier findings that injury-related death rates are significantly elevated among children in rural regions and boys, compared to their urban and fema counterparts (5). The heightened injury mortality rates among young people in China’s rural areas are linked to insufficient adult supervision of children who are left behind (12), as well as a lack of adequate public facilities including readily accessible medical centers. The higher injury fatality rates among boys could be attributed to their increased physical activity, impulsivity, and heightened energy levels, predisposing them to engage in high-risk behaviors (5).
The substantial decrease in injury mortality rates in rural areas between 2010 and 2021 is promising. It may be attributable to accelerated socio-economic advancement experienced in rural China over the past decade. The National Precision Poverty Alleviation Project has seen considerable progress in strengthening rural economic growth and distribution of healthcare resources. From 2010 to 2021, there was an impressive 115.8% rise in the number of health technicians per thousand population in rural sectors, greatly surpassing the 32.9% increase observed in urban sectors (8). Furthermore, the count of children left behind in rural primary and middle schools declined from 15.51 million in 2017 to 12.00 million in 2021 (11).
Our findings indicate that the reasons for injury-related mortalities vary among the five age groups, reflecting different levels of exposure to certain hazards during various stages of child development. Infants under one-year-old, for instance, are more prone to unintentional suffocation due to underdeveloped respiratory systems, making them susceptible to potentially fatal obstructions while eating, playing, or sleeping (13). Older children, on the other hand, are more likely to engage in dangerous activities when left unsupervised, especially near roads or bodies of water (1). During adolescence, the rapid maturation of the brain and hormonal changes coupled with increased exposure to internet and social media, may exacerbate interpersonal stress and emotional instability (14). Such factors could potentially contribute to a rise in suicide rates among adolescents (14). The escalating trend of adolescent suicides that we have observed in China mirrors a global pattern, although the reported rates in China remain lower than in many other countries (15).
Our findings have two policy implications. First, the substantial injury mortality reductions suggest that government goals to reduce child and adolescent injury mortality between 2011 and 2020 have been successful in China. Reduced injury mortality gaps between urban and rural areas and between boys and girls indicate slight improvement in reducing disparities and achieving injury mortality equity across population subgroups.
Second, systematic and intensified prevention efforts should continue according to prevention priorities listed by the Child Development Program of China (2021–2030). Priority should be identification of a government department responsible for injury prevention programs in China to lead implementation of proven prevention programs nationwide like the recent adoption of national child safety seat law.
This study has several limitations. First, due to the absence of data on non-fatal injuries, the results for injury morbidity over the past decade may differ. Second, because data were lacking, this research did not study relevant influencing factors. Conducting research to identify associated risk factors is necessary to fully interpret epidemiological data trends, quantify causal relations between influencing factors and injury mortality, and develop prevention programs.
-
From 2010 to 2021, there was a significant decline in child injury mortality in China. Moreover, injury mortality disparities across area (urban vs. rural) and gender (boys vs. girls) diminished during this period. The dramatic injury mortality decrease likely echoes the impact of governmental interventions. Considering the notably high child injury mortality, however, comprehensive and intensified efforts are encouraged to meet the objectives set forth by the Child Development Program of China (2021–2030).
-
No conflicts of interest.
HTML
Overall Injury Mortality and Subgroup Mortality by Area and Age Group
Subgroup Injury Mortality by Age Group, Sex, and Area
Cause Spectrum of Injury Mortality by Age Group and Area
| Citation: |

|