
 Download:
Download:




-
At 2 p.m. on June 25, 2023, the Zengcheng District CDC reported to Guangzhou CDC that a blood sample from a severely ill child admitted to F Hospital for meningitis at F Hospital had tested positive for Neisseria meningitidis (Nm) via Metagenome Next Generation Sequencing (mNGS). The patient, a 16-year-old student from E School, prompted a collaborative effort between Guangdong CDC, Guangzhou CDC, and Zengcheng District CDC to conduct a comprehensive epidemiological field investigation. This investigation aimed to confirm the diagnosis, assess the extent, characteristics, and potential transmission risk factors of a suspected outbreak, and implement effective outbreak control measures.
-
E School is a private secondary vocational school situated in Zengcheng District, Guangzhou City. The matriculating class of 2022 comprises 1,847 students, as students from the 2020 and 2021 classes have departed for internships, with a total of 177 teachers and staff. The school operates as a closed boarding management institution with regular morning inspections and employs a full-time doctor. The school premises consist of repurposed old factories, situated in an industrial environment.
The confirmed case involved a male student residing in a school dormitory who had been previously healthy and had not received any MenY-containing vaccinations. As shown in Figure 1, symptoms began at 7 a.m. on June 23, manifesting as fever, headache, dizziness, and limb weakness. The individual took ibuprofen at noon and sought care at F Hospital’s fever clinic at 8 p.m. Due to the rapid deterioration of his condition, he was promptly transferred to the emergency department at 9 p.m. and hospitalized in the ICU by 11 p.m. Progression of the illness was swift, characterized by lethargy, sepsis, shock, disseminated intravascular coagulation (DIC), multi-organ system failure, and widespread petechiae and ecchymosis — an indicative profile of fulminant meningococcal meningitis. Subsequent mNGS results from a blood sample taken on June 25 revealed the presence of an Nm sequence, with a serogroup Y meningococcal meningitis (fulminant) diagnosis confirmed on June 26 through positive Nm nucleic acid polymerase chain reaction (PCR) test results. Owing to dry necrosis in his limbs, surgical amputation was necessary. Following discharge from H Hospital on September 5, the patient transitioned to a local rehabilitation facility. Presently, he survives albeit with a compromised quality of life. Further details regarding the timeline, key symptoms, diagnosis, and management approaches can be observed in Figure 1.
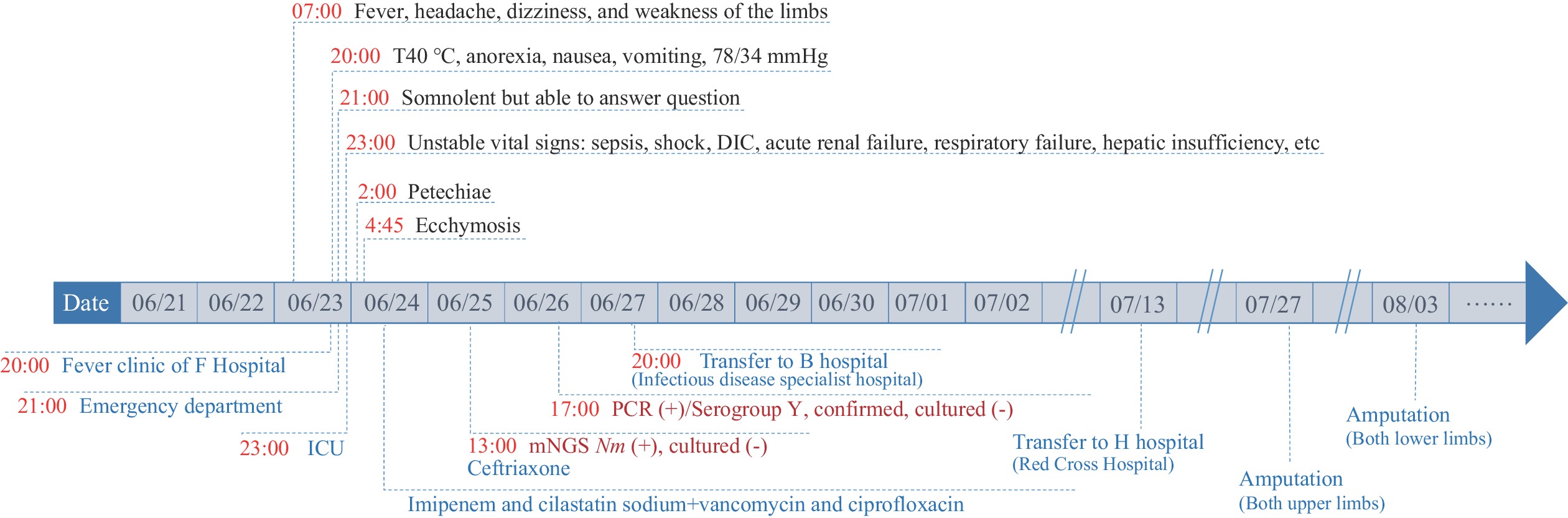 Figure 1.
Figure 1.Timeline of symptoms, diagnosis, and treatment of the confirmed case.
Abbreviation: T=temperature; DIC=disseminated intravascular coagulation; ICU=intensive care unit; PCR=polymerase chain reaction; mNGS=metagenome next generation sequencing; Nm=Neisseria meningitidis.A case definition was formulated, and a thorough case investigation was initiated to determine the extent of a potential outbreak. Following relevant national and provincial surveillance and diagnostic guidelines, a suspected case was characterized as an individual exhibiting fever, headache, vomiting, and/or meningeal irritation. This individual would either be associated with E school, residing in the school vicinity, or the surrounding community between June 1 and June 25, with no definitive exclusion of other diseases. A possible case was identified as a suspected case displaying skin (mucosal) petechiae and ecchymosis. A confirmed case was classified as a suspected or possible case where Nm was successfully cultured and isolated, or there was a positive result for Nm nucleic acid via PCR testing. A carrier was delineated as an individual with a positive Nm culture, or nucleic acid PCR result, but did not meet the criteria for a confirmed case. Close contacts were defined as individuals who had prolonged exposure to a confirmed case through shared living, educational, medical treatment, or dining settings.
Utilizing the specified case definitions, additional cases were sought through a comprehensive approach encompassing a review of school absence and medical records, interviews with various stakeholders including school administrators, doctors, classroom teachers, and classmates, along with scrutiny of medical records from two nearby healthcare facilities (F Hospital and a community health service center). No new confirmed, possible, or suspected cases were identified beyond the primary instance. A total of 82 close contacts were pinpointed, and throat swab samples were collected from them for Nm nucleic acid testing via PCR. Of these close contacts, 24 individuals (29.3%) tested PCR(+). Specifically, 23 were classmates of the index case, and one was the father of the index case. Among the 24 PCR(+) close contacts, 14 exhibited serogroup Y Nm, while the remaining ten were unclassified. A retrospective cohort study was conducted among the close contacts, revealing that the Nm nucleic acid PCR(+) rate was significantly higher among those who shared educational and living quarters with the confirmed case compared to other close contacts {46.0% vs. 3.1%, relative risk (RR): 14.7 [95% confidence interval (CI): 2.1, 103.7]}. Given the elevated carrier rate observed among the close contacts, a risk assessment was carried out by extending the sampling procedure to include the two classes adjacent to the index case’s class, as well as individuals who dined in the school’s cafeteria or engaged in activities such as sports with the confirmed case in outdoor areas, and individuals from surrounding factories and kindergartens. A total of 125 individuals were tested, all returning negative results. The testing outcomes for close contacts and other examined populations are detailed in Table 1 for reference.
Category N Nm nucleic acid PCR(+) n (%) Nm serogroup Close contact 82 24 (29.3) 14 Serogroup Y, 10 unclassified Studied and lived in the same room 50 23 (46.0) 14 Serogroup Y, 9 unclassified Learning in the same class 50 23 (46.0) 14 Serogroup Y, 9 unclassified Living in the same dormitory 5* 3* (60.0) Serogroup Y Other close connection 32 1 (3.1) Unclassified Eating out together 3 0 (0) – Class teacher 9 0 (0) – Patient in the same ICU 16 0 (0) – Patient in the same emergency department 1 0 (0) – Family member 3 1† (33.3) Unclassified Expanded sample 1 — other people in the same school 80 0 (0) – Two adjacent classes 40 0 (0) – Dined in the canteen, played ball, etc. 40 0 (0) – Expanded sample 2 — outdoor activities places 15 0 (0) – Billiards club staff 4 0 (0) – Steak buffet restaurant staff 11 0 (0) – Expanded sampling 3 — factories and kindergartners
around the school30 0 (0) – Note: “–” means not applicable.
Abbreviation: PCR=polymerase chain reaction; ICU=intensive care unit; Nm=Neisseria meningitidis.
* Classmates of the confirmed case.
† Father of the confirmed case.Table 1. Sampling and detection of Nm nucleic acid PCR in close contacts and other populations.
We conducted an analysis of the seating arrangements among the 23 classmates who tested PCR(+). As depicted in Figure 2, groups that included the confirmed case or individuals who were roommates with the confirmed case showed higher rates of PCR(+) compared to groups without the confirmed case or his roommates (69.2% and 57.1% vs. 23.1% and 30.0%, respectively; P<0.05). Notably, the PCR(+) rates between Group 3, including the confirmed case, and Group 1, including the roommates of the confirmed case, did not exhibit a statistically significant difference (69.2% vs. 57.1%; χ2=0.063, P=0.802).
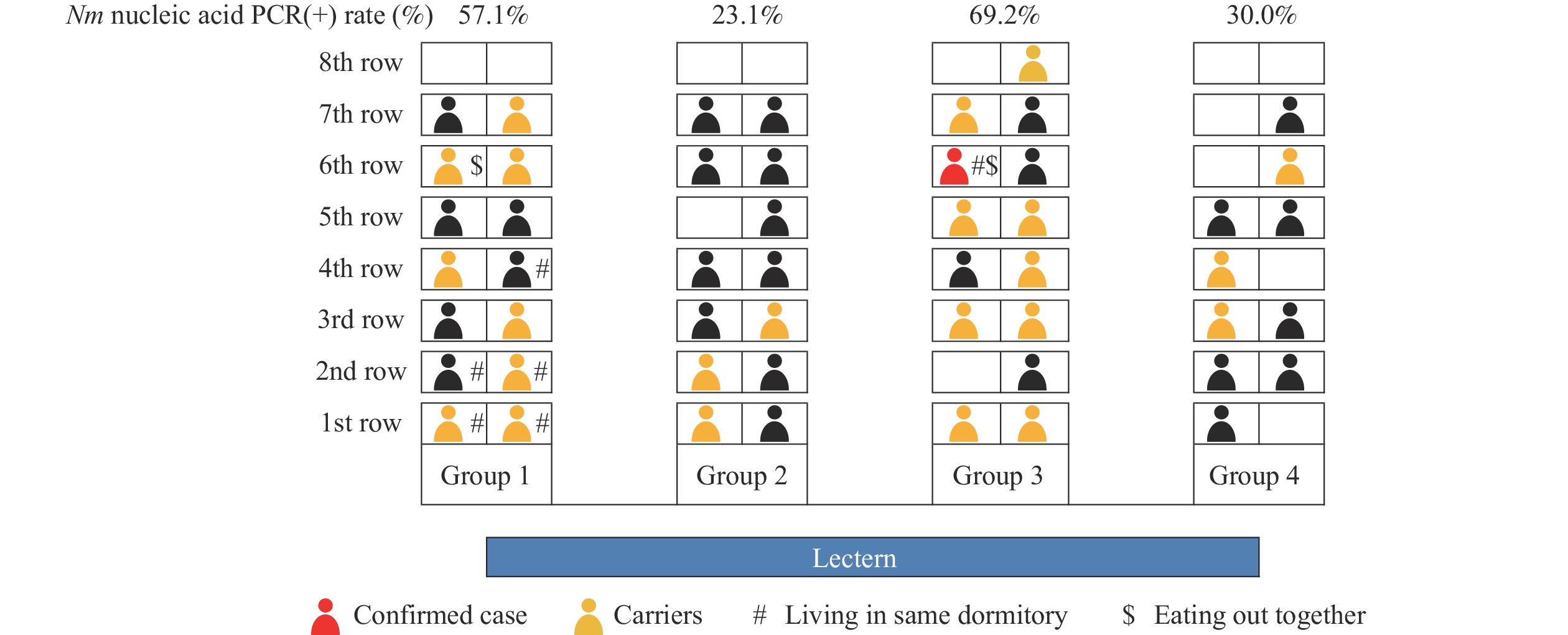 Figure 2.
Figure 2.Seating patterns in the confirmed case’s classroom showing Nm nucleic acid PCR(+) status of classmates.
Abbreviation: PCR=polymerase chain reaction; Nm=Neisseria meningitidis.Cerebrospinal fluid could not be obtained from the confirmed case due to the comatose state. Blood samples from the confirmed case were culture-negative, likely attributed to prior administration of antibiotics before sampling. We successfully cultured and isolated three Nm strains from the 24 Nm nucleic acid PCR(+) close contacts. Through third-generation, whole-genome sequencing, we identified a 1655 Nm sequence type (ST-1655) within clonal complex 23 (CC-23), closely related to strains found in eight cases of serogroup Y Nm previously documented in Guangdong Province.
We conducted an evaluation of vaccination status and identified that neither the confirmed case nor any of their close contacts had a history of receiving MenY-containing vaccines. Given that the school population comprised peers or older individuals compared to the confirmed case, and MenY-containing vaccines were initially approved for use in China in 2008 and are not part of the routine immunization program, we deduced that MenY-containing vaccine coverage among the school population was likely negligible. Through the utilization of the immunization information system, we determined that MenY-containing vaccine coverage was meager in Zengcheng District, with only 3.01% of children aged 2–6 years and 0.45% of children aged 7–18 years having received a MenY-containing vaccine.
Results of antimicrobial susceptibility testing on Nm strains and comprehensive control measures taken in the investigation were shown in the
Supplementary Material . -
Invasive meningococcal disease (IMD) is characterized by its rapid onset and poor prognosis, with untreated cases having a case fatality rate of up to 80% and 4%–20% when appropriately treated (1). Nm comprises twelve serogroups, with serogroups A, B, C, W, X, and Y accounting for almost all IMD cases. Global IMD incidence has generally decreased due to effective meningococcal immunization programs and temporal trends (2). In China, the occurrence of meningococcal meningitis has reached historically low levels (3–4). Notably, there has been ongoing diversification of global meningococcal serogroups. Surveillance data from China over the last decade reveal a shift in the predominant epidemic serogroup of Nm from A to C and B, along with an increase in cases of serogroups Y and W (3).
The confirmed case in this outbreak exhibited an acute onset of illness that quickly escalated to a severe state, a characteristic presentation of fulminant meningococcal meningitis. The rapid advancement to irreversible physical damage underscores the potent pathogenicity of serogroup Y Nm. Despite the current low incidence of meningococcal meningitis, the gravity of the illness, poor outcomes, and potential sequela warrant significant attention, even in sporadic cases. Timely detection and treatment are crucial once Nm infection is suspected.
The outbreak analysis revealed that serogroup Y Nm, similar to other Nm serogroups, commonly exists in a carrier state. Nm colonizes the human respiratory tract as an opportunistic pathogen, which can be challenging to detect but can be present in respiratory secretions. Carriers play a crucial role as potential sources of infection. Therefore, it is imperative that upon diagnosing an Nm infection, efforts be made to identify other infected individuals and implement prophylactic measures to curtail further transmission.
Nm is a fragile pathogen with limited viability outside the host, requiring specific time and space conditions for survival and transmission. Our investigation demonstrates that individuals carrying Nm are frequently identified among classmates or roommates of confirmed case, highlighting the role of sustained close contact in shared environments as a significant transmission risk factor. An analysis of seating arrangements within the confirmed case’s classroom revealed that both the classroom groups of the confirmed case and his roommates exhibited higher rates of Nm carriage compared to other classroom groups. This increased risk of infection could be attributed to cohabitation with a confirmed case, as evidenced by the presence of three PCR(+) roommates serving as potential sources of infection. Furthermore, the confirmed case’s frequent visits to his roommates’ classroom group may have contributed to this observed similarity in infection risk. The findings underscore the importance of close contact in fostering Nm transmission. Therefore, during a meningococcal meningitis outbreak, individuals with prolonged exposure to a case in shared spaces should be prioritized for active surveillance, monitoring, and appropriate medical intervention.
The confirmed case in this outbreak marked the ninth reported instance of serogroup Y meningococcal meningitis in Guangdong Province since the initial serogroup Y case was documented in Dongguan City in 2019 (5). The genotype observed in this outbreak aligns with what has been documented in Hunan and other provincial-level administrative divisions (PLADs) of China (5–6). Pathogen surveillance data indicates that there were no reports of serogroup Y meningococcal meningitis in China before 2014 (4). However, since then, five cases of serogroup Y meningitis in Guangdong Province since the initial serogroup Y case was documented in Dongguan City in 2019 (5). The genotype observed in this outbreak aligns with what has been documented in Hunan and other provincial-level administrative divisions (PLADs) of China (5–6). Pathogen surveillance data indicates that there were no reports of serogroup Ymeningococcal meningitis have been reported in Tianjin Municipality, Guangdong Province, Zhejiang Province, and Ningxia Hui Autonomous Region from 2015 to 2019 (3,5,7), highlighting a delayed emergence of serogroup Y meningococcal meningitis in China. In contrast, serogroup Y was already prevalent worldwide by 2011 and has been reported in 23 countries, emerging as a predominant epidemic serotype in North and South America and Northern Europe (8–9).
Presently, the principal clonal complexes (CCs) of the six major highly pathogenic serogroups causing global epidemics are A (CC-5, CC-7), B (CC-41/44, CC-32, CC-18, CC-269, CC-8, CC-35), C (CC-11), Y (CC-23, CC-167), W-135 (CC-11), and X (CC-181) (10). In China, all serogroup Y cases reported belong to CC-23, consistent with the epidemic clonal complex of serogroup Y (CC-23, CC-167). With an increasing number of reported cases and affected regions of serogroup Nm, ongoing etiological surveillance and population carrier monitoring are imperative for effective prevention and control of meningococcal meningitis.
Immunization rates with Men-A-C-containing vaccines (MPV-A and MPV-AC) are notably high due to their inclusion in the NIP. Conversely, MenY-containing vaccines (MPV-ACYW135 and MPCV-ACYW135) are not part of the routine immunization schedule and were only granted approval in China in 2008 and 2021, respectively. Seroprevalence studies conducted across various Chinese regions have shown relatively low levels of immunity against serogroup Y Nm, ranging from 10% to 60%. An unpublished investigation conducted in Guangdong revealed a 35% Nm IgG seroprevalence rate, suggesting suboptimal population immunity.
Based on the findings of this investigation, we propose the reinforcement of etiological surveillance and population carrier surveillance for Nm. Notably, Nm serogroups in China are undergoing continuous change and diversification. However, the current NIP vaccines only target serogroups A and C, omitting serogroups B, Y, and W. Therefore, the research and development of multivalent meningococcal vaccines and the refinement of immunization strategies are crucial for effective prevention and control of Nm infections in China.
-
No conflicts of interest.
-
Dr. Lance Rodewald for refining the language of this manuscript.
HTML
| Citation: |

|