
 Download:
Download:




-
Globally, female genital organ cancers (vulva, vagina, cervix, corpus uteri, ovary) accounted for approximately 15% of all female cancer cases and fatalities (1-2). In February 2024, the International Agency for Research on Cancer (IARC) published the most recent data on cancer incidence globally across 185 countries. It was estimated that there were 1,472,801 new cases and 680,041 deaths attributed to female genital organ cancers worldwide in 2022 (3).
The World Health Organization (WHO) Global Cervical Cancer Elimination Initiative, launched in 2020, underscored the importance of ongoing surveillance and monitoring of female-specific cancers as a critical component of effective intervention strategies against these diseases. Yet, in China, there is a notable scarcity of recent surveillance data regarding cancers of the female genital tract, particularly those affecting less common sites such as the vulva and vagina. Addressing this deficiency, our study aimed to present the latest incidence and mortality figures for cancers of the female genital organs in 2022, as well as their epidemiological trends spanning from 2010 to 2018 within China. These findings were consistent with the data published in GLOBOCAN 2022. The insights garnered from this research are intended to assess the impact of existing cancer prevention and control measures for women and to guide future health policy decisions in China.
-
A total of 700 population-based cancer registries in China provided high-quality cancer surveillance data in 2018, which were aggregated to estimate cancer incidence and mortality rates based on sex (male/female), age groups (0–84 in 5-year increments, and ≥85 years), and geographical regions (urban/rural). Out of these registries, 106 provided consistent high-quality data from 2010 to 2018, which were combined to analyze rate trends over this period using an age-period-cohort model. Detailed information on quality control and calculations can be found in a previous publication (4). Projections for cancer incidence and mortality rates in 2022 were made using baseline data from 2018 and the rate trends estimated from 2010 to 2018. For this study, we specifically focused on datasets related to female genital cancers (C51–54 and C56, ICD-10).
The National Bureau of Statistics of China supplied the total population numbers of China for 2022 categorized by region and sex. Based on the demographic distribution from the Seventh National Census of China in 2020, we calculated the population estimates by age group for 2022. Subsequently, the incidences and mortalities of cancer were determined by applying rates to the respective population groups.
-
The age-standardized incidence rate (ASIR) and age-standardized mortality rate (ASMR) were calculated using Segi’s world standard population. The proportion of cases or deaths from specific cancer sites among total cancer cases or deaths was determined. Trend analysis was conducted through Joinpoint regression analysis, and results included annual percent changes (APC) and average annual percent change (AAPC). Statistical analyses were performed using Stata (version 13.0, Stata Corporation, College Station, Texas, USA) and Joinpoint software (version 4.6.0.0, Applications Branch, National Cancer Institute, Bethesda, USA).
-
In 2022, there were approximately 296,300 new cases of female genital cancer in China, representing 12.93% of all new cancer cases in females. The ASIR was 26.90 per 100,000, with a higher rate in rural areas compared to urban areas.
Cervical cancer showed the highest incidence with 150,700 cases and an ASIR of 13.83 per 100,000, followed by corpus uteri cancer, ovarian cancer, vulvar cancer and vaginal cancer. The ASIRs for corpus uteri and ovarian cancers were higher in urban areas than in rural areas, while the ASIRs for vulvar, vaginal, and cervical cancers were higher in rural areas compared to urban areas (Table 1).
Area Site ICD-10 Incidence Mortality Cases
(×10,000)Ratio Crude rate
(1/105)ASIR
(1/105)Deaths
(×10,000)Ratio Crude rate
(1/105)ASMR
(1/105)All All C51–54, C56 29.63 12.94 42.89 26.90 10.49 11.10 15.18 8.44 Vulva C51 0.41 0.18 0.60 0.32 0.20 0.21 0.28 0.14 Vagina C52 0.27 0.12 0.39 0.23 0.11 0.11 0.15 0.08 Cervix C53 15.07 6.58 21.81 13.83 5.57 5.89 8.06 4.54 Corpus uteri C54 7.77 3.39 11.25 6.84 1.35 1.43 1.96 1.05 Ovary C56 6.11 2.67 8.84 5.68 3.26 3.46 4.73 2.64 Urban All C51–54, C56 17.84 12.43 39.38 25.94 5.98 11.54 13.20 8.05 Vulva C51 0.23 0.16 0.51 0.30 0.11 0.21 0.24 0.13 Vagina C52 0.14 0.10 0.32 0.21 0.06 0.13 0.14 0.08 Cervix C53 8.55 5.96 18.87 12.49 3.02 5.82 6.66 4.11 Corpus uteri C54 5.01 3.49 11.06 7.10 0.79 1.52 1.74 1.03 Ovary C56 3.91 2.72 8.62 5.84 2.00 3.86 4.42 2.70 Rural All C51–54, C56 11.78 13.77 49.60 28.73 4.50 10.57 18.98 9.04 Vulva C51 0.18 0.21 0.76 0.36 0.09 0.21 0.37 0.15 Vagina C52 0.12 0.15 0.53 0.26 0.04 0.10 0.17 0.08 Cervix C53 6.52 7.61 27.42 16.23 2.55 5.98 10.74 5.16 Corpus uteri C54 2.76 3.23 11.63 6.45 0.56 1.32 2.38 1.07 Ovary C56 2.20 2.57 9.26 5.43 1.26 2.96 5.32 2.58 Note: Ratio means the proportion of the cases/deaths of the cancer site in the total cancer cases/deaths.
Abbreviation: ASIR=age-standardized incidence rate; ASMR=age-standardized mortality rate.Table 1. The incidence and mortality of female genital cancers in China by cancer site and area, 2022.
The incidence rate of vulvar cancer increased with age, reaching its peak in the 80–84 age group. Vaginal cancer peaked at ages 70–74 in urban areas and 75–80 in rural areas. Both cervical and corpus uteri cancers peaked in the 50–54 age group. Ovarian cancer had high incidence rates in the 60–74 age groups (Figure 1).
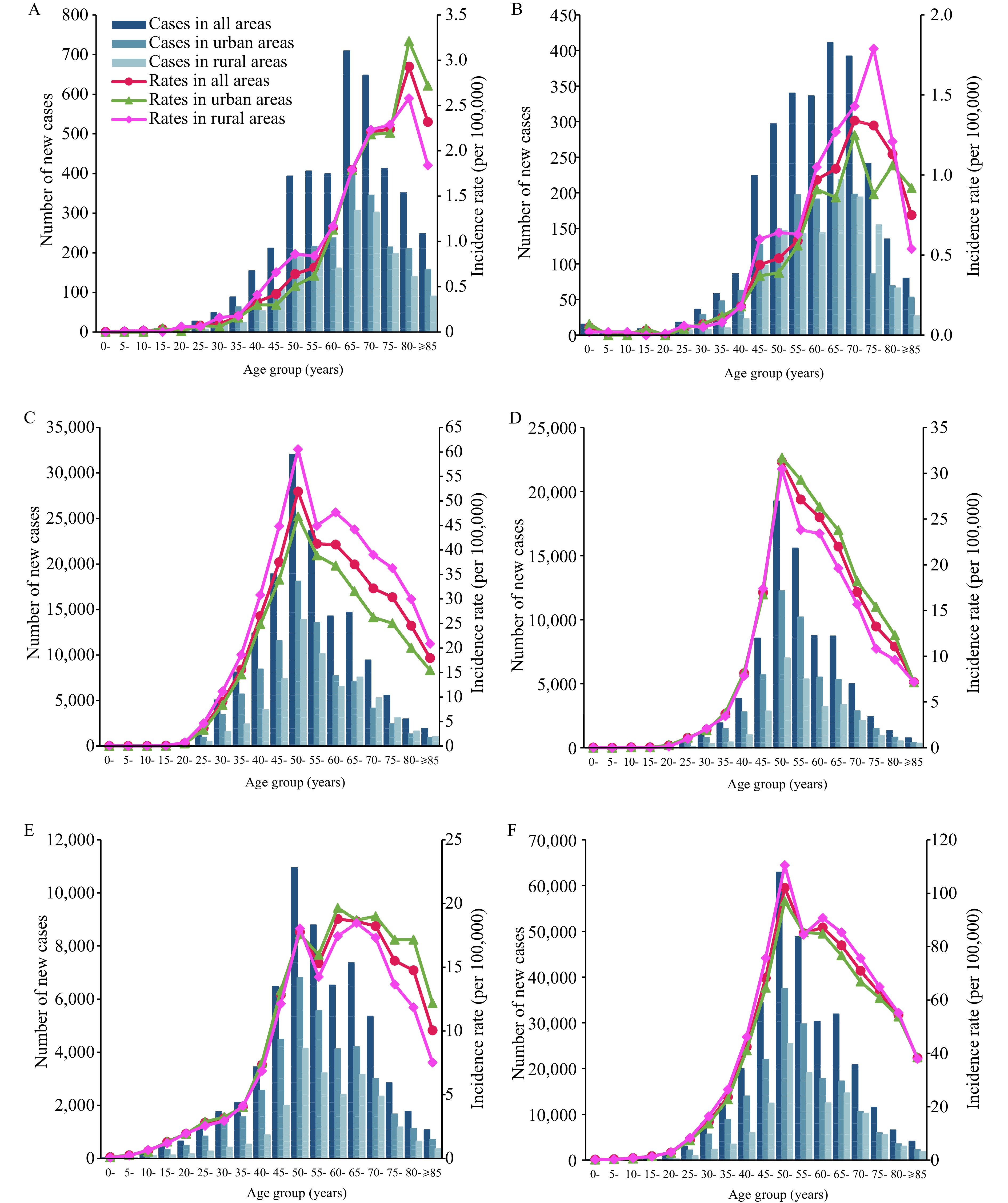 Figure 1.
Figure 1.The incidence cases and rates of female genital cancers in China by cancer site, age group and area, 2022. (A) Vulva (C5l); (B) Vagina (C52); (C) Cervix (C53); (D) Corpus uteri (C54); (E) Ovary (C56); (F) AIl (C51–54, 56).
-
In 2022, there were an estimated 104,900 deaths from female genital cancers in China, representing 11.10% of all cancer-related deaths in females. The ASMR was 8.44 per 100,000, with higher rates observed in rural areas compared to urban areas.
Cervical cancer had the highest mortality with 55,700 cases and an ASMR of 4.54 per 100,000. This was followed by ovarian corpus uteri, vulvar and vaginal cancer. Ovarian cancer had a higher ASMR in urban areas, whereas other cancers in female genital organs showed higher ASMRs in rural areas compared to urban areas (Table 1).
Mortality rates for cancer generally rise with age, except for ovarian cancer in rural areas, where the rates peak among individuals aged 70–74. Minor increases were noted in the 50–54 age group for cervical cancer across all regions, as well as for cancers affecting the vagina and ovary in rural areas. (Figure 2).
 Figure 2.
Figure 2.The deaths and mortality rates of female genital cancers in China by cancer site, age group and area, 2022. (A) Vulva (C5l); (B) Vagina (C52); (C) Cervix (C53); (D) Corpus uteri (C54); (E) Ovary (C56); (E) AIl (C51–54, 56).
-
The ASIR for female genital cancers showed a notable increase from 2010 to 2016 [APC=2.6%, 95% confidence interval (CI): 2.1%, 3.1%, P<0.001], followed by a stabilization between 2016 and 2018. Analyzing by region, urban areas displayed a significant and consistent increase in ASIR throughout 2010 to 2018. In contrast, rural areas witnessed a steep rise from 2010 to 2014, then leveling off from 2014 to 2018.
The ASIRs for vulvar, vaginal, and ovarian cancers remained stable in urban areas from 2010 to 2018. However, there was a significant increase in the ASIRs of cervical cancer and corpus uteri cancer over the same period.
In rural areas, from 2010 to 2018, there was a significant increase in the ASIRs for vaginal cancer, corpus uteri cancer, and ovarian cancer. The ASIRs for vulvar cancer and cervical cancer initially increased significantly, stabilizing around 2014–2016 (Figure 3,
Supplementary Table S1 ).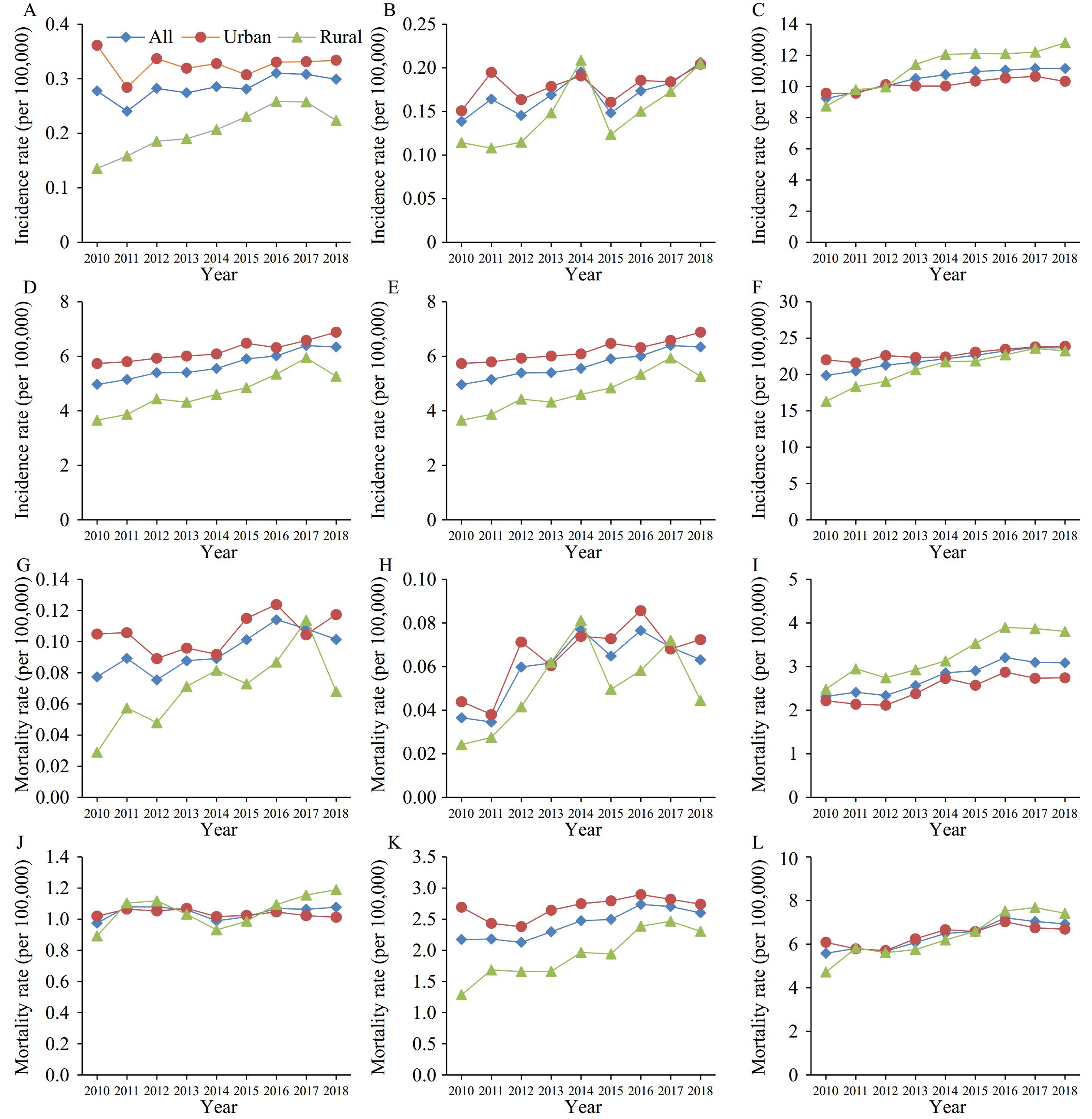 Figure 3.
Figure 3.Trends in incidence and mortality rates of female genital cancers in China by cancer siteand area, 2010−2018, (A) lncidence rates for vulva (C5l); (B) lncidence rates for vagina (C52); (C) lncidence rates for cervix (C53); (D) lncidence rates for Corpus uteri (C54); (E) lncidence rates for ovary (C56); (F) lncidence rates for all (C51–54, 56); (G) Mortality rates for vulva (C5l); (H) Mortality rates for vagina (C52); (I) Mortality rates for cervix (C53); (J) Mortality rates for Corpus uteri (C54); (K) Mortality rates for ovary (C56); (L) Mortality rates for all (C51–54, 56).
-
The ASMRs for female genital cancers showed a significant increase from 2010 to 2018, with an APC of 3.4% (95% CI: 2.3%, 4.5%, P<0.001). This increase was observed in both urban areas and rural areas.
When examining specific cancer sites, there were no notable changes in the ASMRs for vulva, corpus uteri and ovary cancers (P>0.05) in urban areas. Conversely, there was a significant increase in ASMRs for vaginal cancer and cervix cancer over the period 2010 to 2018 in urban areas. In rural regions, most female genital cancers saw notable increases in ASMRs over the same period, except for corpus uteri cancer, which did not show a statistically significant trend in ASMR (Figure 3,
Supplementary Table S2 ). -
Cervical cancer was the most common malignancy and cause of death in female genital organs, accounting for 6.9% of all female cancer cases and 8.1% of all deaths worldwide (3). Globally, the rates of cervical cancer rates decline with higher Human Development Index (HDI) scores (5). China’s figures from GLOBOCAN 2022 show that the country ranks 94th for age-standardized incidence rate and 126th for mortality rate out of 185 countries, both falling below global averages (ASIR of 14.1 per 100,000 and ASMR of 7.1 per 100,000) (3).
Although cervical cancer rates in China have historically been low, a concerning increase in both incidence and mortality was observed across urban and rural areas from 2010 to 2018. This trend poses a potential threat to the national goal of eradicating cervical cancer by 2030. Nonetheless, due to the long-term nature of cancer prevention strategies, it is premature to make definitive judgments at this stage (6). Despite the implementation of a cervical and breast cancer screening program for rural women in 2009, its coverage remained limited when considering the overall population of at-risk females (7). Singh et al. (5) conducted a comparison of age-specific incidence between countries with extensive screening programs and those with limited or no screening, revealing a post-35-year-age stabilization of cervical cancer rates in the former and a dramatic upsurge peaking around 55–64 years in the latter. Our current findings indicate that China’s incidence pattern closely resembles that of countries with insufficient screening coverage, underscoring the need to enhance our national screening efforts. On a more positive note, earlier analyses have shown early signs of the impact of comprehensive cervical cancer prevention and control measures on younger Chinese women (8). The China Women’s Development Guidelines (2021–2030) has set forth clear directives aiming to eradicate cervical cancer (9). Projections suggest that if vaccination and screening outreach are maximized, this goal could be attainable as early as the 2050s (10). Patience is necessary, as the full benefits of these interventions will unfold over time.
Ovarian cancer is a significant type of female genital cancer, representing 3.4% of all female cancer cases and 4.8% of all female cancer-related deaths (3). Research shows a positive association between the incidence of ovarian cancer and the HDI (2). According to GLOBOCAN 2022 data, China’s ASIR and ASMR of ovarian cancer were relatively low, ranking 103rd and 155th out of 185 countries, indicating a lower disease burden compared to other nations (3).
Recent decades have shown a decline in ovarian cancer incidence in Europe and North America (11), partially due to the widespread use of oral contraceptive pills (12) and decreased use of menopausal hormone therapy (13). In contrast, upward trends have been observed in Japan, India, Belarus, and China, potentially linked to obesity and the adoption of a Western lifestyle (14). Notably, China’s rural areas have experienced the most significant increases in both incidence and mortality rates of ovarian cancer, further research is imperative to elucidate the causes of these trends and to inform evidence-based policymaking.
Uterine corpus cancers represented 4.4% of all female cancer cases and 2.3% of global female cancer-related deaths. In the GLOBOCAN 2022 report, the ASIRs and ASMRs of uterine corpus cancer in China were lower than the global averages, ranking 98th and 128th out of 185 countries (3). Endometrial cancer was the primary type of uterine corpus cancer (ICD-10 C54). While the global incidence of endometrial cancer has been rising, particularly in rapidly developing nations (15), we noted a significant increase in incidence rates in both urban and rural areas. However, mortality rates have remained relatively steady over time, suggesting improvements in disease detection, management, and treatment efficiency.
Vulvar and vaginal cancers represented 0.7% and 0.6% of all female cancer cases and deaths globally. According to GLOBOCAN 2022, China’s age-standardized incidence and mortality rates for vulvar/vaginal cancer were ranked 139th/127th and 130th/121st, respectively, among 185 countries, which are below the global average (ASIR of 0.8/0.4 per 100,000 and ASMR of 0.3/0.2 per 100,000) (3). While a global increase in vulvar cancer incidences has been noted, particularly among younger women, the incidence of vaginal cancer has remained fairly stable (16). Despite the relatively low absolute numbers of vulvar and vaginal cancer cases and deaths in China, the country has experienced the fastest rates of increase and significant fluctuations, predominantly in rural areas. The majority of vaginal cancers and a proportion of vulvar cancers are associated with human papillomavirus (HPV), suggesting that HPV-related cancer risks remain high and may continue to escalate. Conversely, the sharp increases in these cancers may also be attributed to their rarity, which renders them more sensitive to changes in diagnostic specificity over time (17).
There were still some limitations. First, the projections of the incidence and mortality from 2018 to 2022 considered the demographic changes, but didn’t take the impact of changes in disease diagnose ability or screening strategies into consideration. However, since the forecast year span was short, the impact of these factors was expected to be negligible. Second, since China is still undergoing a rapid socio-economic transformation, there may be noticeable changes in the population in rural areas, which may lead to possible estimation bias.
In conclusion, this study provides an overview of the current status and trends of female genital organ cancers in China, in alignment with GLOBOCAN 2022. Variations in the epidemiological patterns based on cancer site and geographic location highlight the necessity for tailored cancer prevention and control programs to address the growing disease burden.
-
No conflicts of interest.
-
Staff of 700 population-based cancer registries who provided cancer surveillance data in 2018.
HTML
Data Sources
Statistical Analysis
Incidence in 2022
Mortality in 2022
Trends in Incidence Rates from 2010 to 2018
Trends in Mortality Rates from 2010 to 2018
| Citation: |

|