
 Download:
Download:




-
Human papillomavirus (HPV) infections and reproductive tract infections (RTIs) are significant public health concerns that primarily spread through sexual activity, affecting women’s health. Co-infection of HPV and RTIs can increase the risk of female reproductive tract infections and cervical cancer. This cross-sectional study, conducted in six tertiary hospitals in China from June 2021 to December 2022, aims to investigate the associations between various RTIs pathogens and HPV infections among women aged 18–49 years. The analysis included 3,133 women attending gynecology outpatient clinics. The overall rate of co-infection with HPV and RTIs was 13.2%. After adjusting for demographic factors, both the single-RTI-positive group [odds ratio (OR)=1.97, 95% confidence interval (CI): 1.59, 2.45] and the multiple-RTI-positive group (OR=4.85, 95% CI: 3.59, 6.56) showed significantly higher infection rates of HPV in general, as well as high-risk HPV (HR-HPV) and HPV 16/18. The study also found significant associations between RTI pathogens, including Neisseria gonorrhoeae (NG), Chlamydia trachomatis (CT), Ureaplasma species (UU), Mycoplasma genitalium (MG), Mycoplasma hominis (MH), and Herpes Simplex Virus Type II (HSV-2) infections, and HPV infections (general HPV, HR-HPV, and HPV 16/18). This research highlights the importance of understanding the relationship between RTIs and HPV infection, especially HR-HPV infection, in order to raise awareness of RTIs and HPV co-infection and facilitate early detection of disease-free latent infections.
RTIs can cause a range of symptoms and complications in the female reproductive tract, with potential long-term effects (1). Main pathogens include NG, CT, MG, and HSV-2, which are associated with conditions such as gonorrhea, chlamydial infections, and genital herpes. MH and UU, including Ureaplasma urealyticum (Uu) and Ureaplasma parvum (Up), are the most common Mycoplasma species in the reproductive tract and are also classified as RTIs in this study. In 2016, the World Health Organization (WHO) estimated 376.4 million new cases of chlamydia, gonorrhea, syphilis, and trichomoniasis globally (2). HPV is a significant sexually transmitted infectious pathogen, and persistent HR-HPV infection is a leading cause of cervical cancer. HPV types 16 and 18 are responsible for approximately 70% of all cervical cancer cases (3). The increasing prevalence of co-infections between HPV and other RTIs, coupled with changing modern lifestyles and sexual attitudes, highlights the need for heightened attention in public health and medicine. RTI pathogens, such as NG, CT, and Mycoplasma species, have been found to potentially enhance HPV replication and persistence, leading to accelerated cervical neoplasia development (4). Therefore, it is crucial to detect and treat HPV and RTIs co-infections to develop targeted testing and screening programs, facilitate treatment and management strategies, and ultimately improve disease outcomes. Nevertheless, research on the association between RTI pathogens and HPV, as well as the prevalence of HPV-RTIs co-infections, is limited. Hence, this study aims to investigate the prevalence and association between various RTI pathogens and HPV to provide evidence and recommendations for the clinical diagnosis and management of vaginal and cervical infections.
This multicenter, cross-sectional study was conducted from June 2021 to December 2022 at six tertiary hospitals in China: Peking University First Hospital, Beijing Obstetrics and Gynecology Hospital, Shengjing Hospital of China Medical University, Tianjin Medical University General Hospital, Northwest Women’s and Children’s Hospital, and the Third Affiliated Hospital of Zhengzhou University. We recruited women of reproductive age (18–49 years) who attended the gynecology outpatient clinics at each hospital for either reproductive tract infection treatment or opportunistic screening for cervical cancer. Inclusion criteria included previous sexual history, pre-menopausal status, absence of menstruation at the time of sampling, and no sexual activity, vaginal medication, or douching within 3 days prior to sample collection. Exclusion criteria included pregnancy or within 8 weeks postpartum, vaginal bleeding, history of genital tract tumors, recent treatment for HPV infection or sexually transmitted diseases associated with pathogens, history of hysterectomy, cervical surgery, or pelvic radiotherapy, cervical ablation or excision treatment within the past 12 months, and antibiotic or probiotic use within the past month.
Based on previous studies, the estimated prevalence of co-infection between HPV and other RTIs in gynecology outpatients was approximately 15%. Therefore, we aimed to recruit a sample size of 2,242 participants for this cross-sectional study. Ultimately, cervical samples were collected from a total of 3,281 participants for HPV and RTI pathogens detection. After excluding samples that did not meet the qualification criteria or had missing results, 3,133 samples were included in the final analysis. HPV genotyping was performed using the 21 HPV GenoArray Diagnostic Kit (HBGA-21PKG; HybriBio Ltd., Chaozhou, China), which detects 14 HR-HPV types (HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68), 1 suspected HR-HPV type (HPV 53), and 6 low-risk HPV (LR-HPV) types (HPV 6, 11, 42, 43, 44, and CP8304). The STD6 GenoArray Diagnostic Kit (HBGA-STD6; HybriBio Ltd.) was used to detect 6 common RTI pathogens, including NG, CT, UU (Uu, Up1, Up3, Up6, Up14), MG, MH, and HSV-2.
Categorical variables were presented as numbers (n) and percentages (%), and the chi-square test was used to compare the co-infection of HPV and other RTI pathogens. Univariate and multivariate logistic regression models were used to analyze the association between common RTI pathogens and HPV infection, with calculation of ORs and 95% confidence intervals CIs. Statistical analyses were performed using STATA (version 14.0; Stata Corporation, College Station, TX, USA) and R (version 4.2.3; R Foundation for Statistical Computing, Vienna, Austria). Statistical significance was determined using two-tailed tests with a significance level of 0.05. The study design underwent review and approval by the Biomedical Research Ethics Committee of Peking University First Hospital (2021KY069), and sample collection received authorization from the Human Genetics Resources Administration of China ([2022]CJ0124).
A total of 3,133 subjects were included in the study, with 13.2% having co-infections of both HPV and RTI pathogens. The co-infection rates varied across different demographic characteristics (
Supplementary Table S1 ). The overall RTIs positive rate was 46.0%, with UU (42.1%), CT (4.9%), and MH (4.7%) being the most prevalent RTI pathogens. Of the 109 women (3.5%) with multiple RTIs co-infections, the most common combinations were MH+UU (43.1%), CT+UU (36.7%), and CT+MH (4.6%) (Figure 1C). The co-infection rates were 13.2% for HPV-positive, 11.4% for HR-HPV-positive, and 3.0% for HPV 16/18-positive (Table 1). HPV and RTI pathogens co-infections were found in 413 women (13.2%), with the most common combinations being HPV+UU (65.9%), HPV+MH+UU (9.9%), and HPV+CT+UU (9.2%) (Figure 1D). After adjusting for age group, ethnicity, education level, family monthly income, marital status, and parity, both the single-RTI-positive group (OR=1.97, 95% CI: 1.59, 2.45) and multiple-RTI-positive group (OR=4.85, 95% CI: 3.59, 6.56) had higher rates of HPV infection compared to the RTI-negative group. Furthermore, individuals infected with NG, CT, Uu, Up1, Up3, Up6, any UU, MG, MH, or HSV-2 also had a significantly higher risk of HPV infection. Similar results were observed for HR-HPV and HPV 16/18 infections (Table 2). Significant correlations were also found between different HPV genotypes and RTI pathogens (Supplementary Figure S1 ).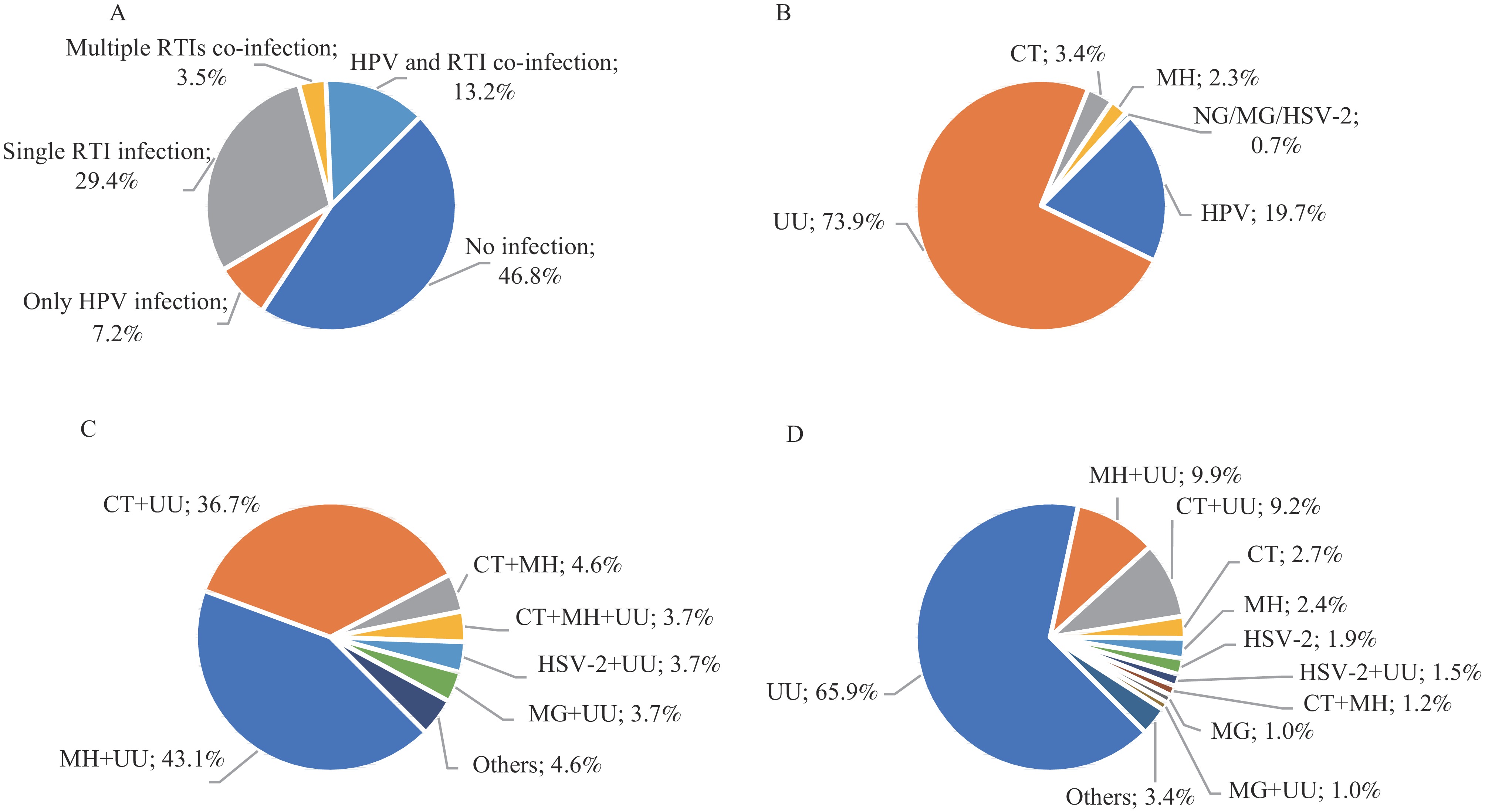 Figure 1.
Figure 1.Patterns of RTI pathogens and HPV infection among reproductive-age women in six tertiary hospitals in China from June 2021 to December 2022. (A) Pattern of infection (n=3,133) (B) Pattern of single infection (n=1,146) (C) Multiple RTI co-infections (n=109); (D) HPV and RTI co-infection (n=413).
Note: RTI pathogens in our study included NG, CT, UU, MG, MH, and HSV-2.
Abbreviation: HPV=human papillomavirus; RTI=reproductive tract infection; NG=Neisseria gonorrhoeae; CT=Chlamydia trachomatis; UU=Ureaplasma species; MG=Mycoplasma genitalium; MH=Mycoplasma hominis; HSV-2=Herpes Simplex Virus Type II.
RTI pathogens Total (n=3,133) Co-infection with HPV Co-infection with HR-HPV Co-infection with HPV 16/18 NG-positive 10 (0.3) 6 (0.2) 5 (0.2) 2 (0.1) CT-positive 152 (4.9) 61 (1.9) 49 (1.6) 12 (0.4) UU-positive 1,320 (42.1) 371 (11.8) 322 (10.3) 79 (2.5) Uu-positive 319 (10.2) 100 (3.2) 84 (2.7) 23 (0.7) Up1-positive 169 (5.4) 48 (1.5) 44 (1.4) 9 (0.3) Up3-positive 556 (17.7) 142 (4.5) 121 (3.9) 31 (1.0) Up6-positive 424 (13.5) 137 (4.4) 122 (3.9) 30 (1.0) Up14-positive 11 (0.4) 4 (0.1) 3 (0.1) 0 (0) MG-positive 21 (0.7) 12 (0.4) 11 (0.4) 4 (0.1) MH-positive 147 (4.7) 62 (2.0) 54 (1.7) 13 (0.4) HSV-2-positive 27 (0.9) 18 (0.6) 18 (0.6) 3 (0.1) Any RTIs-positive 1,442 (46.0) 413 (13.2) 357 (11.4) 93 (3.0) Abbreviation: HPV=human papillomavirus; HR-HPV=high risk HPV; RTI=reproductive tract infection; NG=Neisseria gonorrhoeae; CT=Chlamydia trachomatis; UU=Ureaplasma species; Uu=Ureaplasma urealyticum; Up=Ureaplasma parvum; MG=Mycoplasma genitalium; MH=Mycoplasma hominis; HSV-2=Herpes Simplex Virus Type II. Table 1. Detection rate of different RTI pathogens and HPV co-infection among reproductive-age women in six tertiary hospitals in China from June 2021 to December 2022 [n (%)].
RTI pathogens Total HPV-positive HR-HPV- positive HPV 16/18-positive n (%) Crude OR
(95% CI)Adjusted OR
(95% CI)*n (%) Crude OR
(95% CI)Adjusted OR
(95% CI)*n (%) Crude OR
(95% CI)Adjusted OR
(95% CI)*Neisseria gonorrhoeae Negative 3,123 633 (20.3) Ref. Ref. 558 (17.9) Ref. Ref. 137 (4.4) Ref. Ref. Positive 10 6 (60.0) 5.90 (1.66, 20.97) 10.82 (2.04, 57.4) 5 (50.0) 4.60 (1.33, 15.93) 6.86 (1.49, 31.72) 2 (20.0) 5.45 (1.15, 25.9) 9.31 (1.70, 51.08) Chlamydia trachomatis Negative 2,981 578 (19.4) Ref. Ref. 514 (17.2) Ref. Ref. 127 (4.3) Ref. Ref. Positive 152 61 (40.1) 2.79 (1.99, 3.90) 2.64 (1.80, 3.86) 49 (32.2) 2.28 (1.60, 3.25) 2.18 (1.47, 3.24) 12 (7.9) 1.93 (1.04, 3.57) 2.14 (1.13, 4.05) Ureaplasma species Negative 1,813 268 (14.8) Ref. Ref. 241 (13.3) Ref. Ref. 60 (3.3) Ref. Ref. Positive 1,320 371 (28.1) 2.25 (1.89, 2.69) 2.13 (1.75, 2.59) 322 (24.4) 2.10 (1.75, 2.53) 1.96 (1.60, 2.41) 79 (6.0) 1.86 (1.32, 2.62) 1.73 (1.18, 2.54) Ureaplasma urealyticum Negative 2,814 539 (19.2) Ref. Ref. 479 (17.0) Ref. Ref. 116 (4.1) Ref. Ref. Positive 319 100 (31.3) 1.93 (1.49, 2.49) 1.97 (1.46, 2.65) 84 (26.3) 1.74 (1.33, 2.28) 1.67 (1.22, 2.29) 23 (7.2) 1.81 (1.14, 2.87) 1.59 (0.92, 2.72) Ureaplasma parvum 1 Negative 2,964 591 (19.9) Ref. Ref. 519 (17.5) Ref. Ref. 130 (4.4) Ref. Ref. Positive 169 48 (28.4) 1.59 (1.13, 2.25) 1.45 (1.00, 2.12) 44 (26.0) 1.66 (1.16, 2.37) 1.58 (1.07, 2.32) 9 (5.3) 1.23 (0.61, 2.45) 1.01 (0.46, 2.24) Ureaplasma parvum 3 Negative 2,577 497 (19.3) Ref. Ref. 442 (17.2) Ref. Ref. 108 (4.2) Ref. Ref. Positive 556 142 (25.5) 1.44 (1.16, 1.78) 1.36 (1.07, 1.73) 121 (21.8) 1.34 (1.07, 1.68) 1.23 (0.95, 1.58) 31 (5.6) 1.35 (0.90, 2.03) 1.16 (0.73, 1.85) Ureaplasma parvum 6 Negative 2,709 502 (18.5) Ref. Ref. 441 (16.3) Ref. Ref. 109 (4.0) Ref. Ref. Positive 424 137 (32.3) 2.10 (1.68, 2.63) 1.93 (1.51, 2.48) 122 (28.8) 2.08 (1.64, 2.62) 1.97 (1.52, 2.54) 30 (7.1) 1.82 (1.20, 2.76) 1.76 (1.12, 2.78) Ureaplasma parvum 14 Negative 3,122 635 (20.3) Ref. Ref. 560 (17.9) Ref. Ref. 139 (4.5) Positive 11 4 (36.4) 2.24 (0.65, 7.67) 2.86 (0.80, 10.3) 3 (27.3) 1.72 (0.45, 6.49) 2.22 (0.57, 8.69) 0 (0) –† –† Mycoplasma genitalium Negative 3,112 627 (20.1) Ref. Ref. 552 (17.7) Ref. Ref. 135 (4.3) Ref. Ref. Positive 21 12 (57.1) 5.28 (2.22, 12.6) 3.17 (1.22, 8.22) 11 (52.4) 5.1 (2.16, 12.07) 3.06 (1.17, 7.99) 4 (19.0) 5.19 (1.72, 15.63) 6.09 (1.91, 19.49) Mycoplasma hominis Negative 2,986 577 (19.3) Ref. Ref. 509 (17.0) Ref. Ref. 126 (4.2) Ref. Ref. Positive 147 62 (42.2) 3.05 (2.17, 4.28) 2.76 (1.87, 4.08) 54 (36.7) 2.83 (1.99, 4.00) 2.48 (1.66, 3.71) 13 (8.8) 2.20 (1.21, 4.00) 2.23 (1.15, 4.30) Herpes simple virus type Ⅱ Negative 3,106 621 (20.0) Ref. Ref. 545 (17.5) Ref. Ref. 136 (4.4) Ref. Ref. Positive 27 18 (66.7) 8.00 (3.58, 17.90) 6.67 (2.89, 15.36) 18 (66.7) 9.40 (4.20, 21.03) 7.94 (3.44, 18.29) 3 (11.1) 2.73 (0.81, 9.18) 2.38 (0.69, 8.25) Any RTIs Negative 1,691 226 (13.4) Ref. Ref. 206 (12.2) Ref. Ref. 46 (2.7) Ref. Ref. Single-RTI-positive 1,125 273 (24.3) 2.08 (1.71, 2.53) 1.97 (1.59, 2.45) 235 (20.9) 1.90 (1.55, 2.34) 1.82 (1.45, 2.28) 63 (5.6) 2.12 (1.44, 3.13) 2.17 (1.41, 3.34) Multiple-RTI-positive 317 140 (44.2) 5.13 (3.94, 6.66) 4.85 (3.59, 6.56) 122 (38.5) 4.51 (3.45, 5.90) 4.17 (3.06, 5.68) 30 (9.5) 3.74 (2.32, 6.02) 3.47 (2.01, 6.00) Abbreviation: HPV=human papillomavirus; HR-HPV=high risk HPV; RTI=reproductive tract infection; OR=odds ratio; CI=confidence interval.
* Adjusted for age group, ethnic group, education level, family monthly income, marital status, and parity.
† Regression was not possible because the sample size of the positive group was 0.Table 2. Association between HPV infection and other RTI pathogens infection among reproductive-age women in six tertiary hospitals in China from June 2021 to December 2022.
-
The co-infection rate of HPV and RTI pathogens in this study was found to be 13.2%, emphasizing the importance of recognizing clinical co-infection of HPV and RTIs. Notably, the rates of general HPV infection, HR-HPV infection, and HPV 16/18 infection were significantly higher among women who tested positive for either single or multiple RTIs, compared to those who tested negative for RTIs. These findings indicate a positive association between HPV and RTIs, underscoring the need for prevention, detection, and proper management of RTIs. Preventing and treating reproductive tract infections may help reduce the prevalence of HPV infection, particularly HR-HPV infection.
The findings of this study provide support for the potential link between RTIs and HPV infection, which is consistent with recent research. However, previous studies have primarily focused on the presence of a single RTI pathogen. CT, a primary pathogen associated with HPV, has been extensively investigated. CT promotes HPV penetration into epithelial cells by inducing inflammation and altering the cervical microenvironment. In turn, HPV can facilitate the spread and multiplication of CT (4). This study also found a positive association between these two infections. Our current understanding of the relationships between NG, MG, HSV-2, and HPV remains limited. A meta-analysis revealed that MG was significantly associated with an increased risk of HR-HPV infection (OR=1.50, 95% CI: 1.11, 2.02) (5). Another cross-sectional study reported that individuals positive for HR-HPV had higher rates of HSV-2 seroprevalence and active infection compared to those who were negative. This may be attributed to co-infection of HSV-2 and HR-HPV, which disrupts local immune responses and promotes HPV-related disease progression (6). The findings of this study are consistent with the aforementioned positive associations.
Additionally, this study identified associations between UU and MH infections with both HPV and HR-HPV infections. UU, a common pathogen causing urinary tract infections, had controversial impact due to a lack of differentiation between Uu and Up subtypes. Previous studies have reported significant associations between UU and HPV, including HR-HPV (5,7), although Zhong et al. found no significant association (8). Despite these significant findings, the high rate of UU positivity in clinical practice limits its clinical diagnostic and treatment significance. Research has also shown a significant association between persistent MH infection and persistent HR-HPV infection (P<0.05), but no significant correlation between prevalent MH and prevalent HR-HPV infection (9). Overall, the associations between MH, UU, and HPV infections remain understudied. Further research is needed to investigate the impacts of UU and MH infection, specifically high-risk UU subtypes, on vaginal microecological balance, persistence and recurrence of HPV infection, and their contribution to cervical cancer development.
There are several limitations worth noting in this study. First, the cross-sectional design prevents us from establishing causal relationships between RTI pathogens and HPV infection, as well as determining their impact on persistent HPV infection. Second, the data collected for this study was limited to 6 hospitals in China, which may not be representative of the overall prevalence of HPV-RTI co-infection. However, this limitation does not affect the results pertaining to the relationship between HPV infection and RTIs. To gain a better understanding of the impact of specific subtypes of MH and UU on health, while excluding other traditional RTIs, further well-designed studies are needed. These studies will provide valuable information to guide routine testing and treatment recommendations.
In conclusion, this study found that the rates of general HPV, HR-HPV, and HPV 16/18 infections were significantly higher in both single-RTI-positive and multiple-RTI-positive groups. Additionally, specific RTI pathogens (NG, CT, UU, MG, MH, and HSV-2) were also associated with higher infection rates. These findings highlight the importance of standardizing the detection and treatment of RTI. By doing so, it may be possible to reduce the risk of high-risk and persistent HPV infection, providing a new approach to preventing cervical cancer and contributing to the goal of eliminating cervical cancer (10).
-
No conflicts of interest.
-
All the participants and investigators from six tertiary hospitals: Peking University First Hospital, Beijing Obstetrics and Gynecology Hospital, Shengjing Hospital of China Medical University, Tianjin Medical University General Hospital, Northwest Women’s and Children’s Hospital, and the Third Affiliated Hospital of Zhengzhou University.
HTML
| Citation: |

|