
 Download:
Download:




-
The global mpox outbreak, starting in May 2022, has spread rapidly across non-endemic regions (1). In this wave of the epidemic, 38% to 50% of mpox patients are also human immunodeficiency virus (HIV)-infected individuals, which face a higher risk of mpox infection, more severe clinical symptoms, and higher mortality rates due to their compromised immune system (2). The spread of mpox is particularly insidious (3), and the absence of smallpox vaccination among individuals born after 1980 has resulted in their lack of resistance to mpox (4). Furthermore, there is currently a lack of effective treatment measures for mpox, with symptomatic supportive therapy being the primary approach in clinical practice. Consequently, preventing and controlling mpox heavily relies on individuals’ self-regulation and responsible behavior. The Knowledge, Attitude, and Practice (KAP) theory, frequently used in health education for HIV-infected individuals and men who have sex with men (MSMs), addresses this need. Establishing beliefs in individuals requires both knowledge and a strong sense of responsibility. Behavior changes positively only when knowledge transforms into belief. Given these circumstances, the objective of this study is to evaluate the current level of mpox KAP among HIV-infected individuals and identify potential influencing factors.
This cross-sectional study was conducted at the Beijing Ditan Hospital of Capital Medical University from July 18 to August 9, 2023, using convenience sampling through a combination of online and field surveys. The study included participants who were 18 years or older, without any gender restrictions, while those who had previously experienced mpox infection or participated in mpox-related programs were excluded. The field survey involved on-site data verification, while the online survey utilized the Questionnaire Star platform to implement logical jumps and limit responses to one per WeChat account, thus ensuring the questionnaire’s data quality.
The questionnaire surveyed sociodemographic characteristics, HIV infection status, and mpox KAP. The 25-question knowledge section, based on the study by Jairoun AA et al. (5), scored 1 point per correct answer, with ≥16 points (≥60% accuracy) indicating mpox awareness. The attitude section included 16 questions and utilized a 5-point Likert scale. Higher scores indicated a more favorable attitude, with 5 points for strongly agree and 1 point for strongly disagree (and vice versa for negative statements). The total attitude score ranged from 16 to 80. Participants scoring ≥48 points (representing more than 60% of the total score) were considered to have a positive attitude towards mpox. To obtain the standardized attitude score, the dimension score was divided by the number of dimension entries. The practice section consisted of 7 questions. The highest score for each question was 3 points, while the lowest score was 1 point. The total practice score ranged from 7 to 21. Participants scoring ≥17 points (representing more than 80% of the total score) were considered to have a positive practice towards mpox. A collinearity test was conducted on the independent variables (
Supplementary Table S1 ). The mpox knowledge, attitude, practice, and KAP scores were converted into binary variables for binary logistic regression analysis.Subject duplication was prevented by cross-verifying paper and electronic questionnaires using a unique identification code referred to as the ART (antiretroviral therapy) number. Statistical analysis was performed using SPSS software (web version 26.0; IBM, New York, USA) and RStudio software (version 4.2.1; R Foundation for Statistical Computing, Vienna, Austria). A significance level of P<0.05 (two-tailed) was employed to determine statistical significance. The Ethics Committee of Ditan Hospital granted approval.
A total of 1,235 individuals with HIV infection were included, with 486 from field surveys and 749 from online surveys. Among the participants, 48.3% (597/1,235) were aged between 35 and 55, 91.5% (1,130/1,235) were male, 61.5% (760/1,235) identified as homosexual, and 61.7% (762/1,235) reported a monthly income over 5,000 Chinese Yuan (CNY). The majority of participants had not received influenza vaccination (72.5%, 895/1,235), had not experienced other sexually transmitted diseases (85.9%, 1,061/1,235), and did not have any chronic diseases (68.9%, 851/1,235). In addition, most respondents reported being infected with HIV for more than 3 years (75.7%, 935/1,235), had a latest CD4 cell count greater than 500/mm3 (55.3%, 683/1,235), and had a latest viral load test result of less than 20 copies/mL (76.2%, 941/1,235) (Table 1).
Variable n Constituent ratio (%) Awareness
rate (%)Knowledge score* Mann-Whitney U test/Kruskal-Wallis test Attitude score* Mann-Whitney U test/Kruskal-Wallis test Practice score* Mann-Whitney U test/Kruskal-Wallis test KAP score* Mann-Whitney U test/Kruskal-Wallis test U value/H value P value U value/H value P value U value/H value P value U value/H value P value Age, years <35 551 44.6 52.3 15 (10, 19) 43.8 <0.001 62 (57, 68) 31.4 <0.001 20 (19, 21) 1.8 0.398 97 (88, 105) 43.6 <0.001 35–55 597 48.3 43.0 14 (8, 18) 60 (55, 65) 20 (19, 21) 93 (83, 101) >55 87 7.1 26.4 9 (0, 15) 59 (52, 64) 20 (19, 21) 85 (77, 98) Gender Male 1,130 91.5 48.6 14 (9, 18) 64.0 <0.001 61 (56, 67) 10.9 0.004 20 (19, 21) 9.1 0.011 95 (85, 103) 37.1 <0.001 Female 103 8.3 16.5 7 (0, 13) 59 (53, 64) 21 (19, 21) 86 (76, 96) Transgender 2 0.2 100.0 22 (22, 22) 65 (57, 72) 21 (21, 21) 108 (100, 115) Registered residence Urban area 645 52.2 55.0 15 (11, 19) 142,773.5† <0.001 62 (57, 67) 165,406.5† <0.001 20 (19, 21) 142,449.0† 0.191 97 (88, 104) 149,673.5† <0.001 Rural area 590 47.8 36.1 12 (6, 17) 60 (54, 65) 20 (19, 21) 92 (80, 100) Sexual orientation Homosexual 760 61.5 54.7 15 (10, 19) 109.6 <0.001 62 (57, 67) 40.6 <0.001 20 (19, 21) 11.2 0.011 97 (88, 104) 78.1 <0.001 Heterosexual 188 15.2 23.4 9 (2, 14) 58 (53, 64) 21 (19, 21) 87 (76, 97) Bisexual 208 16.9 41.8 13 (9, 17) 60 (55, 66) 20 (19, 21) 93 (85, 102) Uncertain 79 6.4 26.6 11 (1, 15) 57 (52, 64) 20 (18, 21) 83 (74, 99) Marital status Unmarried 774 62.7 54.5 15 (10, 19) 97.6 <0.001 62 (57, 68) 46.4 <0.001 20 (19, 21) 6.0 0.114 97 (89, 104) 83.4 <0.001 Married 291 23.6 28.9 11 (3, 15) 59 (53, 64) 20 (19, 21) 89 (79, 98) Divorced
/widowed144 11.6 34.0 13 (5, 17) 59 (54, 64) 20 (19, 21) 91 (81, 99) Cohabitation 26 2.1 50.0 15 (6, 18) 60 (57, 65) 20 (19, 21) 93 (80, 99) Education Master’s degree or above 96 7.8 78.1 18 (15, 20) 209.9 <0.001 63 (58,69) 82.6 <0.001 20 (19, 21) 3.7 0.299 100 (95, 107) 179.2 <0.001 University or technical college 678 54.9 55.0 15 (11, 19) 63 (57, 68) 20 (19, 21) 97 (90, 104) High school or technical secondary 293 23.7 30.4 11 (6, 15) 60 (54, 64) 20 (19, 21) 90 (80, 98) Junior high school or below 168 13.6 18.5 6 (0, 13) 56 (52, 62) 20 (18, 21) 82 (73, 94) Occupation Students 22 1.8 63.6 16 (12, 19) 52.86 <0.001 65 (60, 69) 39.4 <0.001 20 (20, 21) 4.1 0.664 101 (93, 108) 58.5 <0.001 Official staffs/Personnel of enterprises and institutions 144 11.7 55.6 16 (9, 19) 62 (58, 67) 20 (19, 21) 98 (88, 103) Commercial service providers 321 26.0 43.9 14 (9, 17) 60 (56, 66) 20 (18, 21) 94 (84, 101) Workers/Farmers 207 16.8 28.5 11 (3, 15) 58 (52, 64) 20 (19, 21) 88 (79, 97) Retired people 109 8.8 45.9 13 (9, 18) 61 (56, 66) 20 (19, 21) 93 (85, 103) Housekeeping and unemployment 14 1.1 57.1 18 (12, 21) 62 (57, 64) 21 (19, 21) 98 (91, 105) Others 418 33.8 51.7 15 (9, 19) 62 (56, 68) 20 (19, 21) 96 (87, 104) Monthly income <2,000 CNY 199 16.1 34.2 10 (3, 16) 69.6 <0.001 59 (53, 65) 35.2 <0.001 20 (19, 21) 4.0 0.259 88 (78, 101) 70.3 <0.001 2,000–4,999 CNY 274 22.2 34.3 12 (6, 17) 59 (54, 64) 20 (19, 21) 91 (80, 98) 5,000–9,999 CNY 449 36.4 45.4 14 (9, 18) 62 (56, 68) 20 (19, 21) 95 (87, 103) >10,000 CNY 313 25.3 64.5 17 (13, 19) 62 (57, 67) 20 (19, 21) 98 (91, 105) Have you been vaccinated against flu? Yes 340 27.5 47.1 14 (8, 18) 154,652.0† 0.654 60 (54, 65) 137,693.0† 0.010 20 (19, 21) 147,120.0† 0.348 94 (84, 102) 143,029† 0.103 No 895 72.5 45.6 14 (9, 18) 61 (56, 67) 20 (19, 21) 95 (85, 103) Have any other sexually transmitted diseases? Yes 174 14.1 37.9 13 (7, 17) 85,787.5† 0.134 60 (53, 65) 82,192.0† 0.020 20 (18, 21) 76,434.5† <0.001 92 (81, 100) 860,817.5† 0.008 No 1061 85.9 47.3 14 (9, 18) 61 (56, 67) 20 (19, 21) 95 (85, 103) Have any other chronic diseases? Yes 215 17.4 46.0 14 (10, 18) 29.5 <0.001 61 (55, 66) 16.0 <0.001 20 (19, 21) 9.2 0.010 94 (85, 102) 27.9 <0.001 No 851 68.9 48.4 14 (9, 19) 61 (56, 67) 20 (19, 21) 95 (86, 103) Uncertain 169 13.7 33.7 10 (5, 16) 58 (53, 64) 20 (18, 21) 88 (78, 99) Time of confirmed HIV infection <1 year 90 7.3 38.9 13 (5, 17) 4.0 0.137 61 (56, 66) 2.9 0.231 20 (19, 21) 4.6 0.101 94 (83, 101) 4.2 0.120 1–3 years 210 17.0 48.1 14 (9, 18) 62 (56, 67) 20 (19, 21) 95 (87, 104) >3 years 935 75.7 46.2 14 (8, 18) 61 (55, 66) 20 (19, 21) 94 (84, 102) Latest CD4 test results <350/mm3 181 14.6 45.3 14 (9, 17) 48.9 <0.001 60 (55, 65) 25.1 <0.001 20 (19, 21) 5.9 0.052 95 (84, 102) 46.2 <0.001 350–500/mm3 280 22.7 39.6 13 (7, 17) 62 (57, 67) 20 (19, 21) 94 (83, 102) >500/mm3 683 55.3 52.1 15 (10, 19) 61 (56, 67) 20 (19, 21) 96 (87, 104) Uncertain 91 7.4 20.9 8 (1, 13) 57 (52, 63) 20 (18, 21) 83 (74, 97) Latest varial copies test results <20 cps/mL (undetectable) 941 76.2 52.7 15 (10, 19) 127.6 <0.001 62 (57, 67) 58.0 <0.001 20 (19, 21) 2.2 0.329 96 (88, 104) 119.5 <0.001 <105 cps/mL 107 8.6 31.8 11 (4, 15) 58 (53, 64) 20 (19, 21) 89 (80, 98) >105 cps/mL 17 1.4 29.4 10 (4, 15) 59 (52, 64) 21 (17, 21) 90 (78, 97) Uncertain 170 13.8 19.4 8 (0, 13) 57 (52, 63) 20 (18, 21) 83 (73, 95) Abbreviation: HIV=human immunodeficiency virus; CNY=Chinese Yuan; KPA=Knowledge, Attitude, and Practice.
* The normality test results for mpox knowledge, attitude, practice, and KAP scores and scores in all dimensions indicated that the data did not follow a normal distribution (P<0.05) (Supplementary Table S2 ). Consequently, the median and interquartile intervals were utilized to describe the scores.
† Calculations were conducted using the Mann-Whitney U test.Table 1. Sociodemographic characteristics and infection status of HIV-infected individuals (N=1,235).
The mean knowledge score for mpox was 14 (interquartile range: 8–18, range: 0–25), with an awareness rate of 46.0%. Out of the 25 questions, two had a correct answer rate of over 80% (Q1 and Q8), while the other three questions had a correct answer rate over 70% but not exceeding 80% (Q7, Q18, and Q19). The lowest correct answer rate was observed for the two questions related to “rash” (Q12 and Q20). The dimension of epidemiologic characteristics had a relatively high correct answer rate (mean: 62.8%), while the treatment dimension had a low correct answer rate (mean: 37.4%). Three questions in the treatment dimension had a correct answer rate of less than 30.0% (Q22, Q23, and Q24) (
Supplementary Table S3 ). The results of the binary logistic regression analysis indicated that residing in an urban area, homosexual orientation, having a master’s degree or above, and having undetectable viral copies (<20 cps/mL) were all positively associated with knowledge of mpox (Figure 1).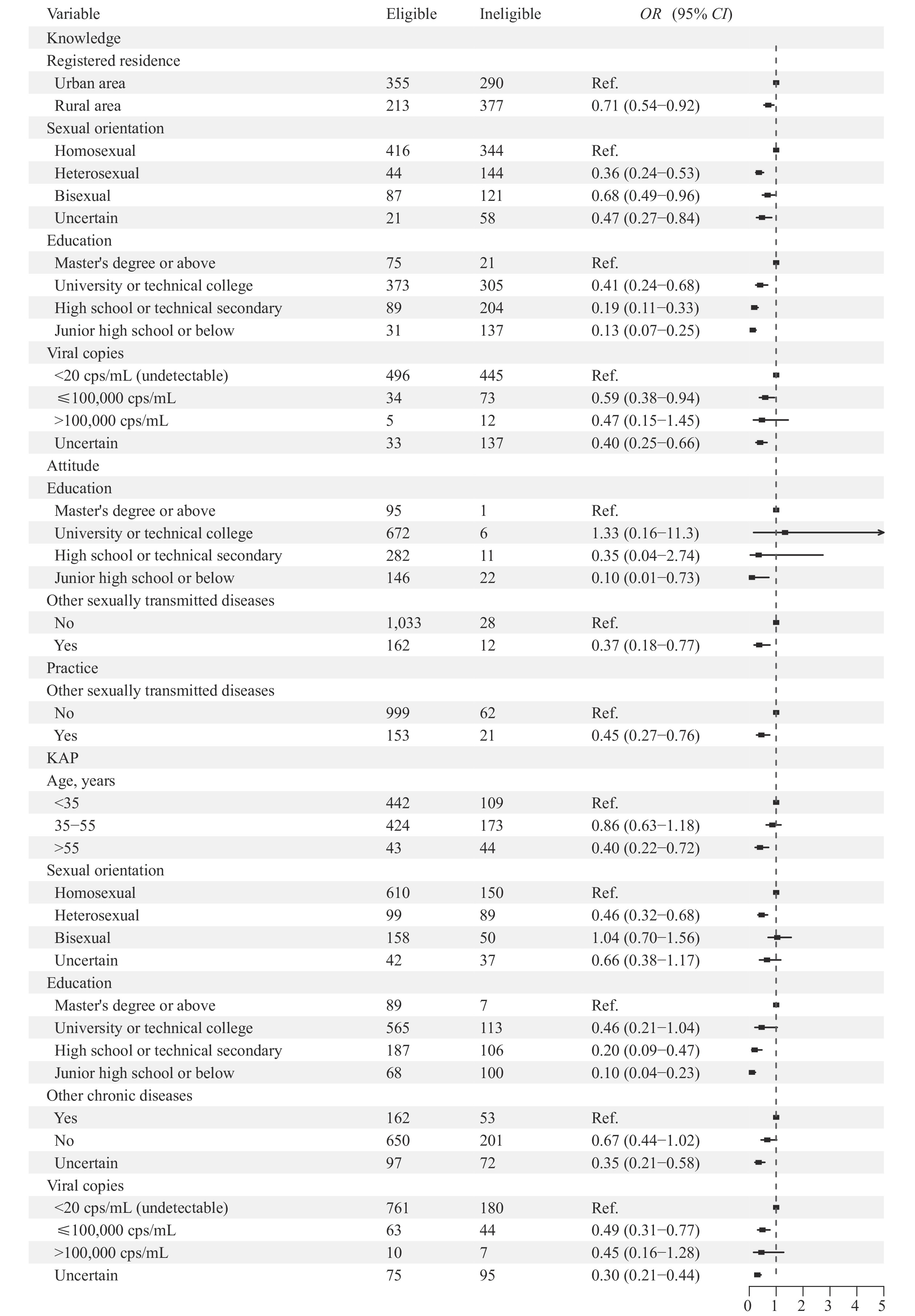 Figure 1.
Figure 1.Binary logistic regression analysis of Knowledge, Attitude, and Practice of mpox.
Abbreviation: OR=odds ratio; CI=confidence interval; KAP=Knowledge, Attitude, and Practice.After accounting for standardization, the total score for mpox attitude was 3.81 (interquartile range: 3.50, 4.12). The barrier dimension had the lowest score, 3.25 (interquartile range: 2.50, 4.00) points (
Supplementary Table S4 ). The results of the binary logistic regression analysis showed that having a master’s degree or higher education and not having any other sexually transmitted diseases (STDs) were positively associated with a favorable attitude towards mpox (Figure 1).The score for mpox practice was 20 (interquartile range: 19, 21). Among the 1,235 individuals infected with HIV, a majority of them (87.3%, 1,078/1,235) sought medical advice upon experiencing unexplained lymphadenopathy and voluntarily disclosed recent exposure to mpox. Furthermore, 78.9% (975/1,235) of individuals expressed willingness to receive the mpox vaccine. With the exception of 27 individuals who had not initiated ART, the majority (87.0% 1,075/1,235) demonstrated good adherence to their daily ART medication. In the past six months, almost 30% (325/1,235) reported having two or more sexual partners, with 107 individuals engaging in male-to-male group sex. When experiencing mpox-related symptoms, the most common actions taken were seeking medical treatment at an infectious disease hospital (96.8%, 1,195/1,235), practicing home quarantine (30.8%, 380/1,235), and notifying the local CDC in their community of residence (29.4%, 363/1,235) (Table 2). The results of the binary logistic regression analysis indicated that not suffering from other STDs was a positive factor associated with the practice of mpox (Figure 1).
Variable n Constituent ratio/percent (%) When you have unexplained lymphadenopathy, will you seek medical advice and inform yourself of mpox-related exposure voluntarily? Yes, I will seek medical advice and inform myself of mpox-related exposure voluntarily. 1,078 87.3 No, I will not seek medical advice and inform myself of mpox-related exposure voluntarily. 96 7.8 Yes, I will seek medical advice, but not inform myself of mpox-related exposure voluntarily. 30 2.4 Not seek medical advice 31 2.5 If the mpox vaccine is available, would you like to get it? Yes 975 78.9 Normal 202 16.4 No 58 4.7 What would you do if you had mpox-related symptoms? (Multiple choices) Go to an infectious disease hospital 1,195 96.8 Informing the CDC in the community of residence 363 29.4 Seek help from social organizations 238 19.3 Ask friends for help 76 6.2 Buy medicine by yourself 57 4.6 Home quarantine 380 30.8 Nothing was done 4 0.3 Whether you can take ART drugs regularly every day? Yes 1,075 87.0 Forget to take it occasionally every month (1 or 2 times) 126 10.2 No, I often forget. 7 0.6 ART is not initiated. 27 2.2 Number of sexual partners engaged in anal sex between men in the past six months. One 325 26.3 Two 173 14.0 Three and above 179 14.5 No same-sex sexual activity has occurred 558 45.2 Has there been any male-to-male group sexual activity in the past six months? Yes 107 8.7 No 1,128 91.3 Abbreviation: HIV=human immunodeficiency virus; ART=antiretroviral therapy. Table 2. Behavioral characteristics of mpox in HIV-infected individuals.
The total KAP score is calculated by summing the scores of mpox KAP. The score range is from 23 to 126, with the highest score being 124 points and the lowest score being 30 points. The majority of research subjects fall within the range of 90 to 106 points. Binary logistic regression analysis revealed that individuals below the age of 35, with homosexual orientation, holding a master’s degree or higher, and having undetectable viral copies (<20 cps/mL) were all positive factors associated with higher mpox KAP scores. The relationship between suffering from chronic diseases and mpox KAP remains uncertain (Figure 1).
-
The survey revealed that the level of knowledge regarding mpox among 1,235 investigated HIV-infected individuals was low (46.0%). This aligns with the awareness rate (47.2%, 1,781/3,563) of mpox among MSM reported by Zheng Min et al. in July 2022 (6) and is significantly lower than the knowledge of other infectious diseases such as acquired immunodeficiency syndrome (AIDS, 91.0%) (7) and syphilis (70.9%) (8). A low level of awareness regarding typical features of mpox, like rash, among HIV-infected individuals was found. It suggests that individuals with HIV do not associate rash with prevention measures or seek medical advice, which hinders self-monitoring of symptoms in key populations. The attitude score towards mpox among HIV-infected individuals was moderate, similar to the findings of an analysis of AIDS health beliefs in newly infected individuals conducted by Yang Rongrong et al. (7.27/10) (9). A lower score in the dimension of the barrier indicates that HIV-infected individuals perceive more obstacles in preventing mpox.The practice scores for mpox were high, as most HIV-infected individuals proactively sought medical advice when experiencing mpox-related symptoms. However, more than 20% of respondents displayed hesitancy towards receiving the mpox vaccine, which was lower than in other studies (78.9% vs. 90.2%) (10).
Approximately 10% of participants engaged in male-to-male group sex in the past six months, increasing mpox infection risks. Despite higher mpox awareness in the homosexual population, behavior changes remain limited, indicating that high awareness rates do not necessarily translate into positives attitudes or behavioral changes. Studies have shown significant knowledge-behavior separation in MSM groups (11). Factors such as social discrimination and traditional culture contribute to the challenge of changing behaviors, with having multiple sexual partners being a common and difficult-to-change behavior in the community.
The absence of other STDs in the past six months positively influenced attitudes and practices related to mpox prevention measures among HIV-infected individuals. HIV-infected individuals with STDs were more likely to engage in sexual activity with multiple partners compared to those without STDs (39.5% vs. 26.6%). This indicates that individuals who are HIV-infected but do not have other STDs are more knowledgeable about safe sexual behavior and are more concerned about their own health in relation to diseases, prompting them to actively seek information about mpox prevention measures. Therefore, implementing interventions targeting HIV-infected individuals with STDs is essential for enhancing their KAP towards mpox.
Viral load significantly influences mpox KAP among individuals living with HIV. Those with undetectable viral load exhibited better medication adherence (89.4% vs. 79.2%). Improving ART effectiveness can enhance mpox KAP, subsequently reducing mpox infection risk. Therefore, targeted interventions and improved adherence to medication should be implemented for HIV-infected individuals with high viral load in order to enhance mpox prevention and control efforts.
This study has certain limitations. First, a convenience sampling method was used, which may affect the representativeness of the results. However, the large size of the cohort helps to mitigate this potential selection bias. Future research should aim to include studies from different regions to obtain a more comprehensive understanding. Second, the inclusion of sensitive questions, such as the number of sexual partners, might introduce information bias. To minimize this issue, questions were placed at the end of the questionnaire, and participants were provided with a private and quiet environment during the survey to encourage honest responses.
This study is the first to investigate mpox KAP among individuals living with HIV. The findings serve as a reference for preventing and managing mpox in this population. The survey results indicate that the level of mpox KAP among HIV-infected individuals is suboptimal. Age, registered residence, sexual orientation, education level, viral load, and co-infection with other STDs are factors that influence mpox KAP. Therefore, targeted mpox health education programs should be prioritized for HIV-infected individuals who have STDs and high viral load.
-
No conflicts of interest.
-
The authors would like to thank the Infection and Immunodeficiency Clinic of Ditan Hospital for supporting the field investigation of this study, and the staff of Red Ribbon House for assisting in the collection of questionnaires. Meanwhile, we would like to express our sincere gratitude to all the HIV-infected individuals who enrolled in this study for their time and efforts.
HTML
| Citation: |

|