
 Download:
Download:




-
On September 3, 2023, a presumed mass poisoning incident occurred in Xingtai City, Hebei Province, China. There were five patients affected, all experiencing different levels of liver damage. Fortunately, there were no reported fatalities. In response, the local CDC formed a dedicated task force to investigate the incident. Through comprehensive epidemiological investigation, laboratory toxin analysis, and biological examination of toxic samples, it was determined that the consumption of wild mushrooms containing α-amanitin was the cause of the poisoning event.
The use of official and self-media channels has been effective in raising awareness and providing education on the risks associated with wild mushroom poisoning. Additionally, a ban has been enforced on the collection and consumption of wild mushrooms. As a result of these measures, no new cases of mushroom poisoning have been reported in Hebei Province.
-
For this study, we defined cases as residents of Xindu District who consumed self-harvested mushrooms and subsequently experienced symptoms such as nausea, vomiting, abdominal pain, or bloating between September 3–4, 2023. We identified cases through the examination of outpatient emergency room registration records at medical establishments in Xindu District, along with physician consultations. On September 4, 2023, the Xindu District Health Commission in Xingtai, received a report from a city hospital about five consecutive suspected cases of food poisoning that morning. The patients, all members of the same family, presented with symptoms including nausea, vomiting, abdominal pain, and diarrhea. They had a history of consuming self-foraged wild mushrooms before the onset of symptoms, leading to the initial hypothesis of mushroom poisoning. To investigate the exact cause, the Xindu District Health Commission requested assistance from the Xindu District CDC.
The incident involved a group of five individuals who were connected by family ties. The group consisted of three males and two females, with ages ranging from 34 to 45 years. Specifically, on September 3, Case A, Case B, Case C, and Case D visited the Zhougong Mountain Scenic Area, where they collected approximately 500 grams of wild mushrooms. Case C, who had previous experience identifying and consuming wild mushrooms in Guizhou, confirmed that the collected mushrooms were edible. Later, Case E joined the group at Case B’s home. At 6:50 p.m., they had dinner, which included the stir-fried collected mushrooms (Figure 1A), along with stir-fried meat with potatoes, stir-fried meat with beans, and rice. It should be noted that the group frequently drank tap water from the municipal supply, which was boiled before consumption. There were no similar cases reported in the neighboring villages or medical facilities at the same time, indicating that contamination from an external source was unlikely.
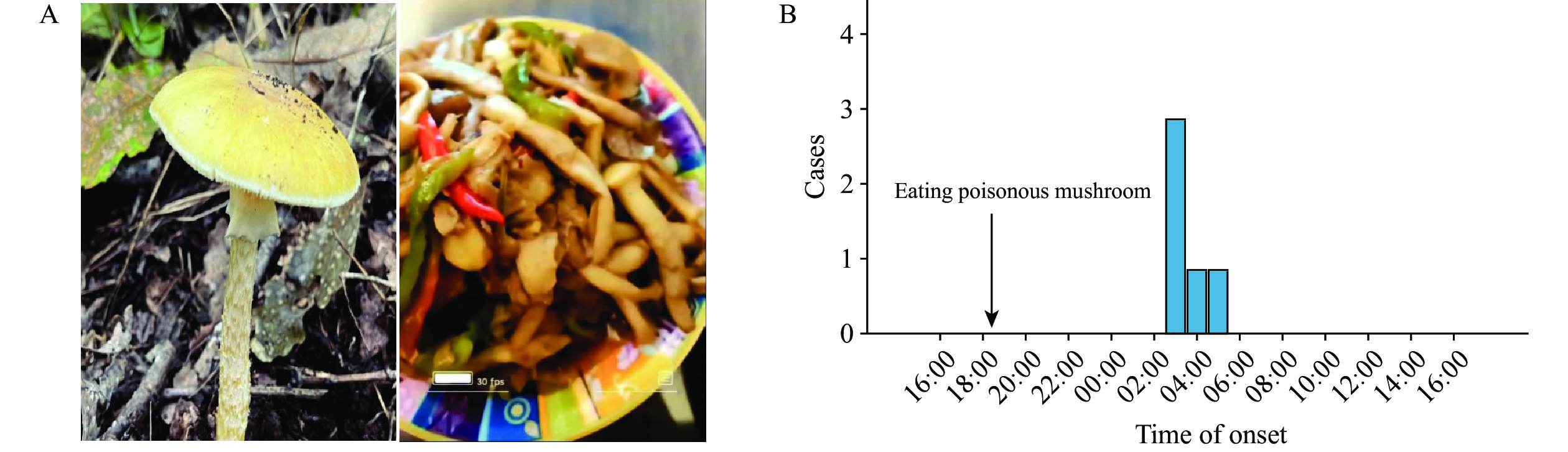 Figure 1.
Figure 1.Amanita subjunquillea 's general appearance and time distribution of onset of accidental mushroom poisoning in Xingtai City, Hebei Province, 2023. (A) Amanita subjunquillea 's general appearance; (B) Time distribution of onset.
Note: The left part of panel A is Amanita subjunquillea collected from a case in A and the right part of panel A is cooked Amanita subjunquillea.Symptoms appeared early the next day, starting with Case A and followed by the other cases within a 2-hour period. Based on this pattern, it was tentatively concluded that the cause was toxin poisoning. The common factor among the patients was the consumption of self-harvested mushrooms during the evening meal on September 3. Therefore, it is highly likely that the mushrooms were the source of the incident.
The results of the epidemiological survey showed that all 5 individuals who consumed fried mushrooms had a 100% incidence rate, but there were no deaths. Among this group, four individuals had eaten a larger quantity of mushrooms, while one individual consumed a smaller amount. The initial clinical symptoms mainly included gastrointestinal issues such as nausea, vomiting, diarrhea, and abdominal pain. Case A exhibited symptoms at 03:06 a.m. on September 4, while the remaining cases developed symptoms within 2 hours thereafter (Figure 1B). The incubation period ranged from 8.5 to 11 hours (Table 1), with the frequency of vomiting and diarrhea being 6 or more times and 8 or more times, respectively, resulting in watery stools. The four individuals who consumed larger quantities of mushrooms also experienced fatigue and depression, whereas the individual who consumed a smaller amount did not exhibit these symptoms, indicating a correlation between symptom severity and mushroom consumption quantity.
Case Gender Age Quantity of food consumed α-amanita toxin (ng/mL)* Early clinical symptoms Course of disease Outcome Vomiting Diarrhea Nausea Abdominal pain Mental depression Pseudo-recovery period Date of consumption Incubation period (hours) Date of damaged liver function A m 34 + 0.23 Yes Yes Yes Yes No No Sep 3 8.5 Sep 4 Survival B f 45 ++++ 1.28 Yes Yes Yes Yes Yes No Sep 3 9 Sep 4 Survival C m 43 ++ 0.45 Yes Yes Yes Yes Yes Yes† Sep 3 9.5 Sep 11 Survival D f 41 +++ 0.71 Yes Yes Yes Yes Yes No Sep 3 10.6 Sep 4 Survival E m 35 ++ 0.46 Yes Yes Yes Yes Yes No Sep 3 11 Sep 4 Survival Abbreviation: Sep=September; m=male; f=female.
* Blood sample sampling time: 6:32 p.m., September 4, 2023.
† Pseudo-recovery period: Case C showed false healing 35–155 hours after exposure.Table 1. Symptoms and course of aggregated cases of poisoning due to accidental ingestion of poisonous mushrooms in Xingtai City, Hebei Province, China, 2023.
Five cases arrived at the emergency department of a hospital in Xingtai City at approximately 6:00 a.m. on September 4th. Blood tests were conducted on these cases at 6:32 a.m. the same day. The blood samples were sent to the Institute of Microbiology of Zhejiang Province for analysis using online solid-phase extraction liquid chromatography-tandem mass spectrometry to detect and trace toxins. α-Amanita was found in all blood samples at levels ranging from 0.23–1.28 ng/mL. Other toxins were not detected in the samples (1). The laboratory results showed elevated levels of aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin (TBIL), direct bilirubin (DBIL), and lactate dehydrogenase (LDH), indicating liver dysfunction, with values predominantly within the ranges of 28.3–2,294.4 U/L, 26.3–2,902.1 U/L, 8.9–51.6 μmol/L, 2.8–19.0 μmol/L, and 202.8–2,305.0 U/L, respectively (Table 2). The treatment consisted of gastric lavage, catharsis, plasma exchange, blood purification, rehydration, and hepatoprotective measures aimed at removing toxins and providing symptomatic relief.
Case Course of disease AST (U/L) ALT (U/L) TBIL (μmol/L) DBIL (μmol/L) LDH (U/L) Hemoperfusion, CRRT,
and plasma exchangeA Onset* 63.0 ↑ 103.0 ↑ 25.4 ↑ 6.3 218.4 Yes Maximun† 65.9 ↑ 135.0 ↑ 51.6 ↑ 12.3 ↑ 213.0 B Onset* 51.3 ↑ 42.0 ↑ 8.9 2.8 228.3 Yes Maximun† 626.5 ↑ 491.2 ↑ 29.3 ↑ 19.0 ↑ 717.0 ↑ C Onset* 33.7 33.7 10.6 3.2 388.0 ↑ Yes Maximun† 41.2 ↑ 67.9 ↑ 15.9 4.9 259.0 ↑ D Onset* 208.7 ↑ 266.9 ↑ 15.7 6.1 545.3 ↑ Yes Maximun† 2,294.4 ↑ 2,902.1 ↑ 29.5 11.6 ↑ 2,305.0 ↑ E Onset* 28.3 26.3 21.1 ↑ 6.5 202.8 Yes Maximum† 412.5 ↑ 343.6 ↑ 45.8 ↑ 17.0 ↑ 328.0 ↑ Abbreviation: AST=aspartate aminotransferase; ALT=alanine aminotransferase; TBIL=total bilirubin; DBIL=direct bilirubin; LDH=lactate dehydrogenase; CRRT=continuous renal replacement therapy.
* Blood sample sampling time: 6:32 a.m., September 4, 2023; AST normal range: 13–35 U/L, ALT normal range: 7–40 U/L, TBIL normal range: 0–21 μmol/L, DBIL normal range: 0–7 μmol/L, LDH normal range: 120–250 U/L, ↑ indicates higher than normal.
† Maximum: The maximum in the course of disease. AST normal range: 13–35 U /L, AST normal range: 7–40 U/L,TBIL normal range: 0–23 μmol/L, DBIL normal range: 0–8 μmol/L, LDH normal range: 120–250U/L, ↑ indicates higher than normal.Table 2. Damaged liver function in aggregated cases of poisoning from accidental consumption of poisonous mushrooms in Xingtai City, Hebei Province, China, 2023.
Epidemiological investigations, laboratory testing, and morphological identification were conducted to determine the cause of the incident. The National Institute of Occupational Health and Poison Control, China CDC, identified wild mushroom ingestion as the cause. The patients had harvested these mushrooms themselves from a pine forest at the summit of the Zhougong Mountain Scenic Area. The mushrooms were identified as Amanita subjunquillea.
-
An investigation was conducted on September 4 by the Hebei Province Field Epidemiology Training Program trainees and CDC professionals from the Xindu District to determine the source and nature of the poisoning, implement containment measures, and prevent future incidents. The investigation team revisited the location of the mushrooms and collected identical specimens. Patients were asked to identify the consistency of the mushrooms they had consumed, which were confirmed to be Amanita subjunquillea. Local authorities promptly initiated public education programs to raise awareness of the risks associated with consuming wild mushrooms and prohibited residents from foraging for and eating them. There have been no subsequent poisoning incidents in the area. The Hebei Provincial CDC recommends conducting educational campaigns on mushroom poisoning before and after the rainy season and installing warning signage in montane areas to discourage collection and consumption of wild mushrooms.
-
Wild poisonous mushrooms are more common in the southern region of China but are less frequently found in the north (2–4). Recent cases of food-borne poisoning in Hebei Province, linked to the consumption of wild mushrooms containing α-amanitin, suggest the presence of such mushrooms in certain northern areas. Interestingly, one affected individual (Case C) had a history of residing in the southern Guizhou region where mushroom foraging is common. While Case C expressed confidence in distinguishing between toxic and non-toxic mushrooms, the majority of local residents reported difficulty in differentiating them based on appearance alone. Factors like climate variation between the northern and southern regions can lead to subtle differences in the appearance of the same mushroom species, increasing the risk of misidentification (5). It is therefore necessary to enhance education on identifying wild poisonous mushrooms, implement stricter policies on mushroom foraging, and increase the visibility of cautionary signage in specific areas. The low incidence of mushroom poisoning in certain areas should also serve as a reminder for the public to remain vigilant about this issue.
In China, more than 90% of all mushroom poisoning deaths are caused by amanitin-containing mushrooms (6). Due to the short half-life of amanitin in the bloodstream, it is essential to promptly initiate blood purification procedures in well-equipped healthcare institutions (7). Early sample collection is critical for rapid identification, accurate diagnosis, and appropriate treatment (8).
HTML
| Citation: |

|