

 Download:
Download:




-
Injuries pose a significant public health challenge, accounting for 10.6% of the global burden of disease (1). The elderly population, due to their diminished ability to control their surroundings, are particularly vulnerable to injuries. In fact, injuries are the second leading cause of death among the elderly, resulting in substantial burden and economic loss for individuals, families, and society as a whole (2-3). Given the rapid growth of China’s aging population, these burdens are expected to escalate, underscoring the need for research on elderly injuries (4-5). Previous studies have shown a downward trend in injury-related mortality among Chinese elderly individuals (6). However, there is limited documentation on the long-term patterns of urban-rural disparities in injury mortality by age, period, and cohort (7). This study aims to examine the changing patterns of injury mortality among the elderly in China from 1987 to 2021, while also identifying the age-period-cohort effects on mortality changes. The findings of this study will provide valuable data for informing the development of injury intervention policies by relevant national agencies.
The injury mortality rates were derived from the death registration system of the National Health Commission in China, as previously described (8). Age-standardized mortality rates (ASMR) per 100,000 population were calculated using the direct method and the World Standard Population as a reference. To identify temporal trends in injury ASMR, a Joinpoint regression model was employed. Furthermore, the age-period-cohort model was used to assess the individual effects of age, period, and birth cohort on injury mortality rates in China (9).
The present study discovered a gradual decrease in injury-related mortality rates among the elderly population in China over a span of 35 years. It is noteworthy that older age, male gender, and residing in rural areas all contribute to a higher risk of injury-related death among the elderly. Although there is a contrasting trend in injury mortality rates between urban and rural areas for the elderly, the disparities in period effects and cohort effects are minimal.
Figure 1 shows long-term trends in ASMR for injury in China’s urban and rural populations by sex from 1987 to 2021. The ASMR from injuries among the elderly largely maintained a gentle decline from 1987 to 2002, except for a rebound period (1996–1998) in rural males. From 2002 to 2006, the ASMR for urban elderly males and females experienced two significant fluctuations, while the rate for rural elderly declined more rapidly. Subsequently, the ASMR for urban and rural elderly exhibited a slight increase. There was a fluctuation characterized by an initial decrease followed by an increase around 2010, and the rate has since remained broadly stable.
 Figure 1.
Figure 1.Trends in age-specific standardized mortality rates of injury among the elderly in urban and rural China by sex: 1987–2021.
The joinpoint results are presented in Table 1. Overall, there was a slight decrease in injury ASMR in both urban and rural areas, although the substage trends varied. In urban areas, ASMR showed a relatively marked decline from 1987–2008, then a slight rebound from 2008–2021. In contrast, ASMR in rural areas showed a slight decline from 1987–2006, and finally a nearly flat rebound from 2006–2021. In addition, all annual percent changes between sexes indicated a slight urban-rural disparity.
Residence Mortality rate† (per 100,000) Entire range§ Segment 1 Segment 2 1987 2021 AAPC (%) 95% CI Period APC (%) 95% CI Period APC (%) 95% CI Urban Total 22.28 11.84 −1.5* (−2.6, −0.6) 1987−2008 −3.2* (−4.1, −2.3) 2008−2021 1.3 (−0.7, 3.3) Male 22.47 14.06 −1.0* (−1.9, −0.0) 1987−2008 −2.6* (−3.6, −1.6) 2008−2021 1.7 (−0.3, 3.8) Female 22.08 9.77 −1.9* (−2.8, −1.0) 1987−2009 −3.4* (−4.3, −2.6) 2009−2021 1.0 (−1.2, 3.2) Rural Total 21.78 17.32 −0.9* (−1.5, −0.4) 1987−2006 −1.7* (−2.2, −0.9) 2006−2021 −0.1 (−1.1, 0.8) Male 25.08 21.09 −0.7* (−1.2, −0.3) 1987−2005 −1.5* (−2.1, −0.8) 2005−2021 0.1 (−0.7, 0.9) Female 18.76 13.70 −1.2* (−1.6, −0.7) 1987−2006 −1.9* (−2.4, −1.4) 2006−2021 −0.2 (−1.0, 0.5) Abbreviation: APC=annual percent change; AAPC=average annual percent change; CI=confidence interval.
* P<0.05.
† Standardization employed is based on the world standard population from the World Health Organization.
§ The time frame considered ranges from 1987 to 2021.Table 1. Joinpoint analysis of age-standardized mortality rates from injury in urban and rural areas.
Figure 2 depicts the net drift and local drift of mortality rates for injury. Both net drift and local drift were calculated separately in the APC model. Net drift represents the time-trend effect on the entire population, while local drift indicates the log-linear trend specific to each age group. In both rural and urban areas of China, there was a similar net drift pattern, with a significant decrease in injury mortality rates over the study period. The decline in mortality rates was more pronounced for females compared to males, both in urban areas (females: −2.12% vs. males: −1.12%) and rural areas (females: −1.33% vs. males: −0.77%). Notably, the local drift curves in urban and rural areas exhibited contrasting patterns. In urban areas, the decline in injury-related mortality became increasingly pronounced with age among the elderly, whereas in rural areas, the opposite trend was observed.
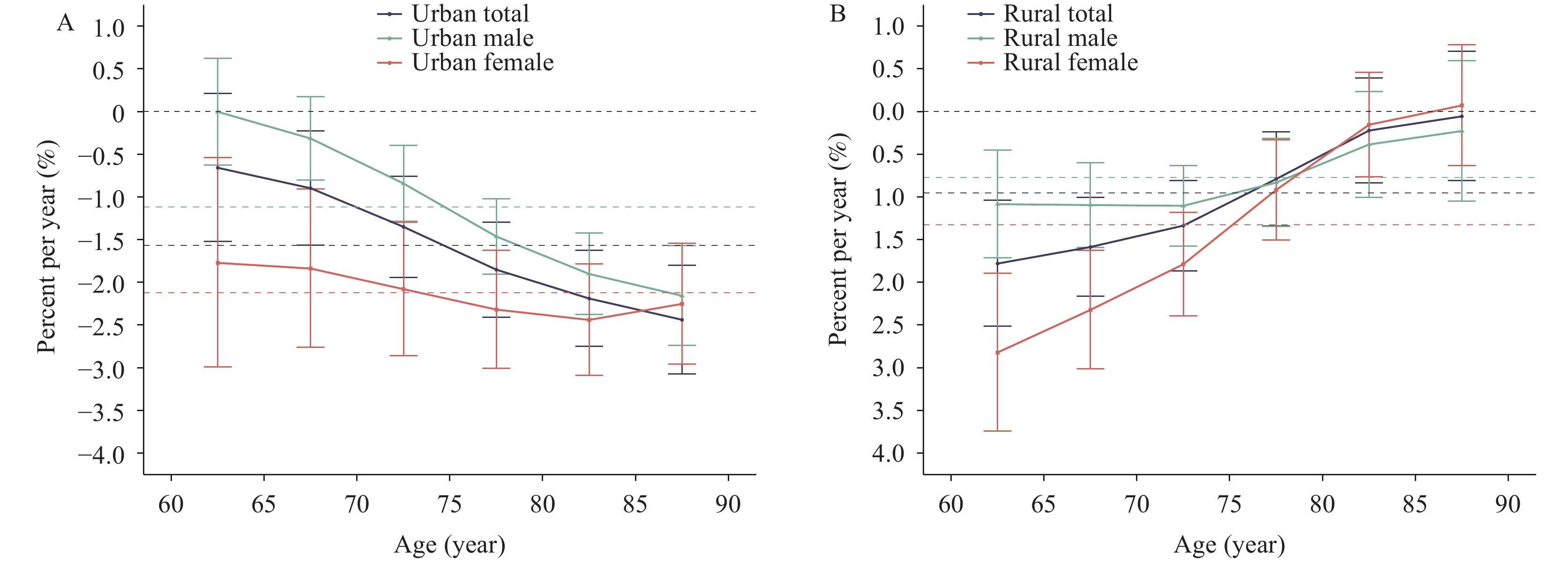 Figure 2.
Figure 2.Local drift with net drift values for injury mortality rates and sex disparity by area in China from 1987 to 2021. (A) Net and local drifts in urban areas; (B) net and local drifts in rural areas.
Figure 3 shows the estimates of age, period, and cohort effects on mortality rates for injuries. Age effect patterns are consistent across sexes, as well as urban and rural areas. The older the age group among the elderly, the higher the mortality. The mortality rate for males is generally higher than that for females, but this sex difference is gradually narrowing. However, the mortality rate for rural elderly individuals is consistently higher than that for the corresponding urban group. Period effects in urban and rural areas are largely consistent, except for the period from 2002–2007. Additionally, the earlier the birth cohort, the higher the mortality rate, whether in urban or rural areas. For the birth cohorts between 1902 and 1927, the urban areas consistently have a higher mortality rate compared to rural areas.
 Figure 3.
Figure 3.The effects of age, period, and cohort on age-standardized mortality rates due to injury among the elderly in China from 1987 to 2021. (A) Age effects in urban areas; (B) age effects in rural areas; (C) period effects in urban areas; (D) period effects in rural areas; (E) cohort effects in urban areas; (F) cohort effects in rural areas.
-
This study examines the long-term trends in injury mortality rates among the elderly population in China over a span of 35 years, with a focus on the urban-rural divide. Our findings reveal several important insights. Firstly, we observed a gradual decrease in elderly injury mortality rates in China over the past 35 years, although there has been a recent minor increase. Secondly, specific high-risk groups for injuries include the older population, males, and rural elderly individuals. Thirdly, the decline in injury mortality rates in urban and rural areas follows opposite patterns: in urban areas, mortality rates decrease more with advancing age, while in rural areas, the trend is reversed. Moreover, both urban and rural settings display similar period and cohort effects. These findings underscore the need for tailored injury prevention programs targeting high-risk elderly groups.
The decrease in mortality rates related to injuries in the elderly population demonstrates improvement in prevention strategies, which can be attributed to various factors. These include enhanced medical access and services resulting from economic growth, making previously fatal injuries treatable. Additionally, expanded public health services and social security have improved healthcare for the elderly, particularly for high-risk groups (6). Moreover, increased health education initiatives have raised awareness and led to a reduction in accidental injuries. However, this declining trend has reached a plateau, evidenced by a recent slight increase, particularly among urban males. This may be attributed to China’s aging population and the ongoing process of urbanization, which exposes elderly males residing in urban areas to greater environmental hazards and an increased risk of injury.
The impact of age on injury-related mortality among the elderly in China has been identified as significant (10). A notable age disparity in injury mortality rates was observed, with rates increasing exponentially with age (6,10). This finding suggests that the older-age elderly are at a higher risk for injuries, potentially due to factors such as declining physical function, pre-existing health conditions, cognitive decline, and sensory impairments. These factors make them more vulnerable to accidents, including falls, traffic accidents, fires, crushing injuries, poisoning, suicide, and other forms of injury (10). Consequently, there is a need for increased attention and targeted efforts towards injury prevention among the older elderly population.
Sex disparity and urban-rural disparity in injury mortality rates are apparent (7,10). Males, particularly in rural areas, face the highest risk of injury, likely due to their participation in outdoor activities that increase exposure to injury hazards (6). Inadequate treatment for injuries among rural elderly can be attributed to limited access to medical resources and lower economic and educational levels. Additionally, the migration of younger, middle-aged workers to cities as a result of urbanization often leaves elderly individuals in rural areas lacking sufficient care. However, the implementation of China’s Healthy Aging initiatives aimed at improving rural healthcare is expected to reduce the urban-rural disparity in injury mortality (4,5,10).
The overall injury mortality rate among the elderly is decreasing, with variations observed across different demographic groups. Females exhibit a more rapid decline in mortality rates compared to males, potentially due to factors such as reduced exposure to high-risk activities and advancements in education and social status over the past three decades. Rural elderly individuals also experience a faster decline in mortality rates compared to their urban counterparts, which can be attributed to notable improvements in rural healthcare services. In urban areas, injury mortality rates decline more rapidly with age, likely due to better access to medical resources, safety facilities, and educational initiatives. Conversely, in rural areas, younger elderly individuals engaged in hazardous activities may face higher risks, but these risks decrease as they age and retire from such tasks. However, due to limited availability of medical resources, particularly those tailored to the elderly population, the decline in injury mortality may be slower for older elderly individuals residing in rural areas.
Period effects demonstrate a decline in injury mortality among the elderly over time (6). Higher mortality rates in earlier birth cohorts suggest that improvements in medical resources and social services have contributed to the reduction in injury mortality. Notably, urban earlier cohorts had higher mortality rates compared to their rural counterparts, possibly due to their exposure to events such as World War II and the Chinese Civil War, which resulted in more conflicts and subsequently increased physical and psychological injuries among urban elderly.
The study has several limitations that must be taken into account. First, the lack of detailed data on specific types of injury hampers the ability to develop more targeted prevention strategies. Second, the dataset used in this study is subject to underreporting, with an estimated underreporting rate of approximately 2%, potentially leading to an underestimation of mortality. Lastly, as with other age-period-cohort studies, there is a possibility of ecological fallacy in our results, which means that findings at the population level may not always be applicable to individuals.
-
No conflicts of interest.
HTML
| Citation: |

|