
 Download:
Download:




-
In the current era of antiretroviral therapy (ART), effective management of patients coinfected with human immunodeficiency virus (HIV)/hepatitis C virus (HCV) is increasingly critical in reducing mortality rates (1). Attrition, defined as loss to patient follow-up or discontinuation of ART, is not merely an indicator for evaluating treatment adherence but also a pivotal factor for effectively managing patients on long-term ART (2). However, the influence of HIV/HCV coinfection on mortality and attrition is still a matter of ongoing debate (3).
In the Guangxi Zhuang Autonomous Region, an estimated 6.6% of individuals undergoing ART were identified as coinfected with HCV (4). This sizeable percentage of HIV/HCV coinfected patients presents unprecedented challenges to the implementation of ART in Guangxi. Prior non-matching studies indicated that most individuals contracted HIV/HCV coinfections through intravenous drug use, while HIV mono-infections were primarily acquired through heterosexual contacts (3–4). However, differences in population composition between these groups might introduce a selection bias. Thus, establishing a recent basis for evaluation is vital for planning effective management strategies.
Findings from the analysis of the propensity score-matched (PSM) cohort, abstracted from China’s National Free Antiretroviral Treatment Program database, showed that HIV/HCV coinfected individuals faced an enhanced risk of all-cause mortality and ART attrition compared to those exclusively infected with HIV. These insights may provide crucial inputs in constructing personalized testing and follow-up protocols for HIV/HCV coinfected patients undergoing ART.
We amassed clinical data from individuals who commenced ART across all 109 allocated hospitals within the 14 prefectures of Guangxi from December 2003 to December 2022. To be qualified for inclusion in the study, participants must have been aged 15 years or older at the time of commencing ART, have had no prior ART experience, and have initiated a standard three-drug regimen in China. Exclusions were made for individuals without the necessary baseline characteristics and initial testing records required for this study, those lacking any follow-up records or drug supply records at the first follow-up appointment, individuals who tested positive for hepatitis B virus (HBV) surface antigen at ART’s initiation, and those lacking CD4+ T-lymphocyte (CD4) count and HIV viral load records in the first and second follow-up years.
Eligible individuals were categorized into two groups according to PSM, specifically those co-infected with HIV/HCV and those solely infected with HIV (
Supplementary Figure S1 ). Those testing negative for HCV antibody and HBV surface antigen were classified as HIV mono-infections, and those testing positive for HCV antibody and negative for HBV surface antigen are categorized as HIV/HCV co-infections. Sex, age, CD4 count, route of HIV infection, primary regimen, and extent of liver damage were chosen as the determining variables. This study employed nearest neighbor matching methods, a seed of 1,234, and a caliper of 0.0001 to match propensity scores.The initial testing was identified as the last test within three months prior to the ART commencement. Survival time was interpreted as the period from the commencement of ART to death from any cause. Individuals were considered censored when their fate was unknown due to either loss to follow-up or discontinuation of ART, or by December 31, 2022. After ART’s initiation, HIV viral load and CD4 count were closely monitored once every 12 months. For mortality analysis, we used a survival curve to indicate the discrepancy in survival probabilities between the two groups, and a Cox proportional hazard model to compute the adjusted hazard ratio (aHR). For attrition analysis, a bee-swarm plot visualized the years from the ART initiation to the first recorded attrition, and the adjusted incidence rate ratio (aIRR) was calculated using a Poisson regression model.
Considering that group matching with PSM is not unique and one individual may be matched to others without significantly altering the association, pair analysis was excluded from this study. In order to pinpoint risk within different subsets of the population, multivariable analyses were broken down by initial liver impairment grade. All statistical analyses were conducted on R (version 4.2.0; R Foundation for Statistical Computing), with tests being 2-sided, and P values of less than 0.05 deemed statistically significant.
Our analyses included 1,191 individuals mono-infected with HIV and an equal number of individuals co-infected with HIV/HCV. There were no significant differences in baseline characteristics between the two groups, as demonstrated in Table 1.
Characteristics Overall HIV HIV/HCV Test statistic P (N=2,382) (N=1,191) (N=1,191) Sex, n (%) 0 (χ2) 1.000 Male 1,624 (68.2) 812 (68.2) 812 (68.2) Female 758 (31.8) 379 (31.8) 379 (31.8) Age [years, mean (standard deviation)] 41.1 (12.0) 41.3 (11.1) 41.2 (11.5) −0.486 (t) 0.627 CD4 count [cells/μL, median (interquartile range)] 174 (46–302) 170 (38–309) 178 (56–293) 692,032 (w) 0.305 Route of HIV infection, n (%) 0 (χ2) 1.000 Injecting drug use 98 (4.1) 49 (4.1) 49 (4.1) Heterosexual contact 2,240 (94.0) 1,120 (94.0) 1,120 (94.0) Homosexual contact with men 44 (1.8) 22 (1.8) 22 (1.8) Primary regimen, n (%) 0.940 (χ2) 0.332 NNRTI backbone 2,186 (91.8) 1,100 (92.4) 1,086 (91.2) PI or INSTI backbone 196 (8.2) 91 (7.6) 105 (8.8) Hepatic impairment, n (%) 0.817 (χ2) 0.665 Normal 488 (20.5) 252 (21.2) 236 (19.8) Grade 1/2 1,216 (51.0) 607 (51.0) 609 (51.1) Grade 3/4 678 (28.5) 332 (27.9) 346 (29.1) Note: HIV refers to individuals mono-infected with HIV, while HIV/HCV denotes individuals co-infected with both HIV and HCV. The NNRTI backbone regimen incorporates two nucleoside reverse transcriptase inhibitors and one non-nucleoside reverse transcriptase inhibitor. The PI backbone regimen includes two nucleoside reverse transcriptase inhibitors and one protease inhibitor, while the INSTI backbone regimen contains two nucleoside reverse transcriptase inhibitors and one integrase strand transfer inhibitor. As per the China Free Antiretroviral Therapy Manual, the upper limit of normal (ULN) for aspartate transaminase (AST), alanine aminotransferase (ALT), and total bilirubin (TBIL) is set at 40 U/L, 40 U/L, and 23 μmol/L respectively. Hepatic impairment is graded as 1 (AST and/or ALT > 1-time ULN, TBIL > 1-time ULN), 2 (AST and/or ALT > 2.5-time ULN, TBIL > 1.5-time ULN), 3 (AST and/or ALT > 5-time ULN, TBIL > 2.5-time ULN), and 4 (AST and/or ALT > 10-time ULN, TBIL > 5-time ULN). Chi-squared test, T-test, and Wilcoxon test were respectively used to calculate the test statistics, denoted as χ2, t, and w.
Abbreviation: CD4=CD4+ T-lymphocyte; NNRTI=non-nucleoside reverse transcriptase inhibitor; PI=protease inhibitor; INSTI=integrase strand transfer inhibitor.Table 1. Baseline characteristics of individuals co-infected with HIV/HCV and mono-infected with HIV in antiretroviral therapy in Guangxi, China, 2003–2022.
In our analysis of all-cause mortality, we observed that of the individuals solely infected with HIV, 68 were deceased. They collectively contributed to a person-time at risk of 8,717.11 person-years (PY), resulting in a mortality rate of 0.78/100 PY [95% confidence interval (CI): 0.62–0.99]. In contrast, among those co-infected with HIV/HCV, 135 individuals were deceased. They amounted to a person-time at risk of 8,767.24 PY, leading to an increased mortality rate of 1.54/100 PY (95% CI: 1.30–1.82). The survival probability notably declined more rapidly for both groups (Figure 1).
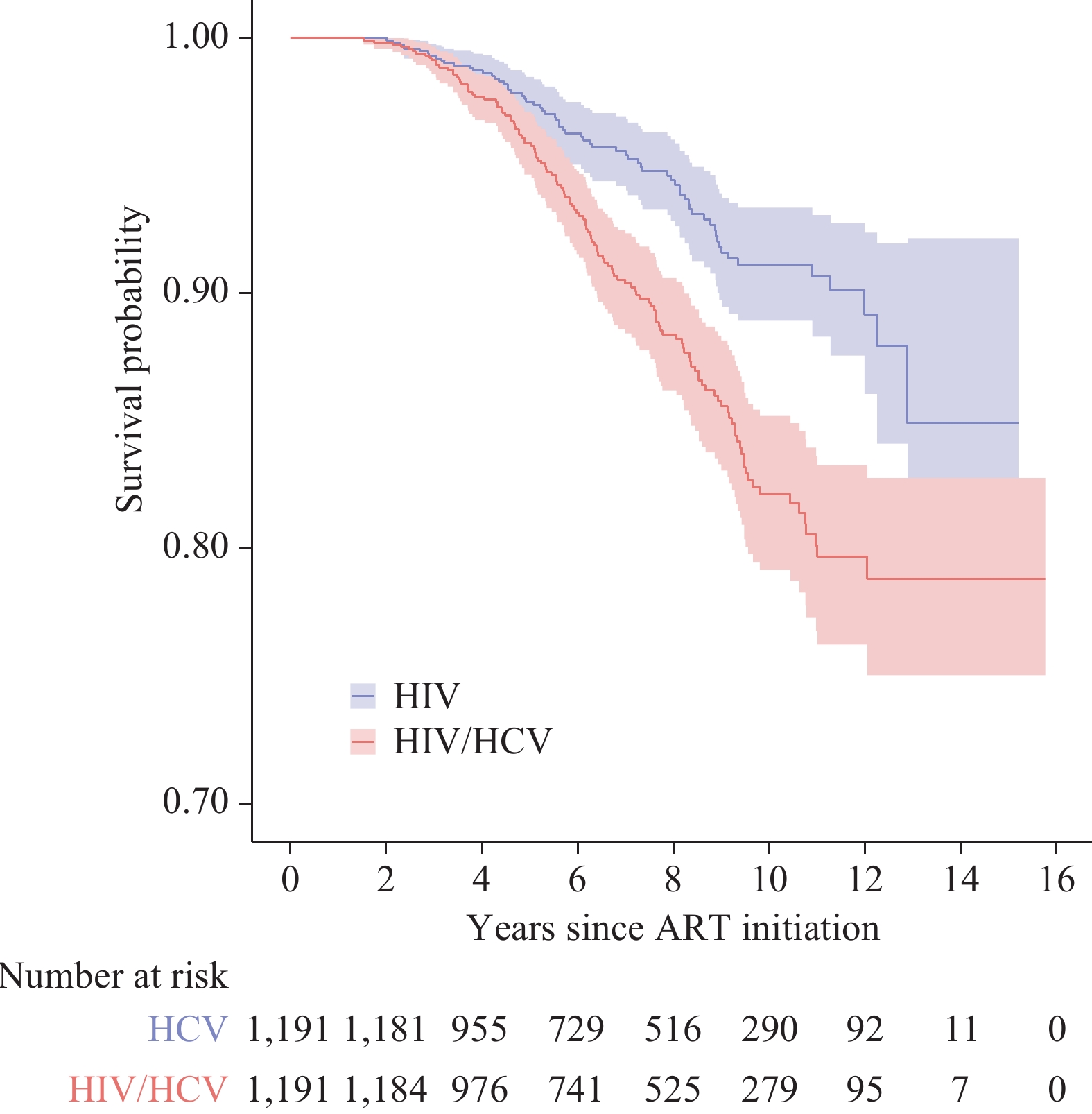 Figure 1.
Figure 1.Comparison of survival probability at given years after antiretroviral therapy initiation between individuals co-infected with HIV/HCV and those mono-infected with HIV in Guangxi, China, 2003–2022.
Note: HIV denotes individuals mono-infected with human immunodeficiency virus, and HIV/HCV represents individuals co-infected with both human immunodeficiency virus and hepatitis C virus.
Abbreviation: ART=antiretroviral therapy.
Comparing infection scenarios, co-infection with HIV/HCV consequently led to an augmented all-cause mortality risk by 104.8%, compared to individuals solely infected with HIV (aHR: 2.048, 95% CI: 1.526–2.749, P<0.001).
Within the cohort devoid of initial hepatic impairment, the risk of all-cause mortality remained similar for HIV/HCV co-infected individuals and those exclusively infected with HIV (aHR: 1.544, 95% CI: 0.748–3.188, P=0.240). However, when evaluating subgroups with initial grade 1/2 and grade 3/4 hepatic impairment, the disparity in all-cause mortality risk between HIV/HCV co-infected individuals and those only infected with HIV was pronounced (Grade 1/2: aHR: 2.008, 95% CI: 1.345–3.000, P=0.001; Grade 3/4: aHR: 2.511, 95% CI: 1.432–4.403, P=0.001) as presented in Table 2.
Characteristics All-cause mortality aHR P Attrition aIRR P Group* HIV 1 1 HIV/HCV 2.048 (1.526–2.749) <0.001 1.659 (1.408–1.961) <0.001 Stratified by hepatic impairment† Normal HIV 1 1 HIV/HCV 1.544 (0.748–3.188) 0.240 1.372 (0.938–2.018) 0.105 Grade 1/2 HIV 1 1 HIV/HCV 2.008 (1.345–3.000) 0.001 1.806 (1.427–2.298) <0.001 Grade 3/4 HIV 1 1 HIV/HCV 2.511 (1.432–4.403) 0.001 1.860 (1.375–2.514) <0.001 Note: HIV represents individuals mono-infected with HIV, whereas HIV/HCV refers to individuals co-infected with both HIV and HCV. aHR stands for the adjusted hazard ratio, determined by the Cox proportional hazard model. Meanwhile, aIRR denotes the adjusted incidence rate ratio obtained through the Poisson regression model. The attrition factor incorporates losses to follow-up along with discontinuation of antiretroviral therapy. Per the prescripts in the China Free Antiretroviral Therapy Manual, the upper limit of normality (ULN) for aspartate transaminase (AST), alanine aminotransferase (ALT), and total bilirubin (TBIL) are set at 40 U/L, 40 U/L, and 23 μmol/L, respectively. Hepatic impairment is categorized into four grades: grade 1 (AST and/or ALT > 1-time ULN, TBIL > 1-time ULN), grade 2 (AST and/or ALT > 2.5-time ULN, TBIL > 1.5-time ULN), grade 3 (AST and/or ALT > 5-time ULN, TBIL > 2.5-time ULN), and grade 4 (AST and/or ALT > 10-time ULN, TBIL > 5-time ULN).
* The models were adjusted for sex, age, initial CD4 count, route of HIV infection, the primary regimen type, and hepatic impairment grade.
† The models were adjusted for sex, age, initial CD4 count, route of HIV infection, and the primary regimen.Table 2. The associations between HIV/HCV co-infection with all-cause mortality and attrition in antiretroviral therapy in Guangxi, China, 2003–2022.
Higher attrition rates were found in individuals co-infected with HIV/HCV compared to individuals only infected with HIV (Figure 2). Despite this, the HIV/HCV co-infection group presented with a significantly extended median time from ART initiation to the first instance of attrition, as compared to the HIV-only group (Figure 2). Those co-infected with HIV/HCV were generally more prone to attrition (aIRR: 1.659, 95% CI: 1.408–1.961, P<0.001) when compared to those only infected with HIV. Similarly, those co-infected with HIV/HCV had an equivalent risk of attrition to the individuals only infected with HIV within subgroups without initial hepatic impairment (aIRR: 1.372, 95% CI: 0.938–2.018, P=0.105), and heightened attrition risk in subgroups exhibiting initial hepatic impairment grade 1/2 (aIRR: 1.806, 95% CI: 1.427–2.298, P<0.001) and grade 3/4 (aIRR: 1.860, 95% CI: 1.375–2.514, P<0.001) (Table 2).
 Figure 2.
Figure 2.Comparison of attrition of antiretroviral therapy between individuals co-infected with HIV/HCV and those mono-infected with HIV.
Note: HIV column means individuals mono-infected with human immunodeficiency virus; HIV/HCV column means individuals co-infected with both human immunodeficiency virus and hepatitis C virus. The points represent years from ART initiation to the first attrition. The notches, upper edges, and lower edges of the boxes represent the median, first quartile, and third quartile of years from ART initiation to the first attrition, respectively.
Abbreviation: ART=antiretroviral therapy.
-
The results of this study underscore that individuals co-infected with HIV/HCV in Guangxi face an elevated risk of all-cause mortality and ART attrition in comparison to their counterparts with only HIV mono-infection. These observations underscore earlier findings detailing shorter survival times in HIV/HCV co-infected individuals, even subsequent to ART (3–5). Further, initial hepatic impairment in individuals simultaneously infected with HIV/HCV corresponded with an increased risk of all-cause mortality.
While individuals co-infected with HIV/HCV exhibited higher attrition rates compared to their HIV mono-infected counterparts, the median duration from ART initiation to the first instance of attrition was notably extended in the co-infected group. This unexpected observation suggests the possible early implementation of intervention strategies for the co-infected population. However, these measures fail to prevent long-term ART interruption in individuals with concurrent HIV/HCV infection. Prior research has documented a correlative high risk of both mortality and attrition amongst this demographic, particularly those who contract HIV/HCV through injecting drug use (6–7). Efforts to counteract this trend include the development of extended-release regimens and non-pharmacological interventions aimed at enhancing adherence (8–9). However, our research indicates that despite controlling for the HIV infection route and other initial characteristics, co-infected individuals consistently demonstrated a higher attrition propensity compared to those only afflicted with HIV. Moreover, stratified analyses highlighted hepatic impairment as a significant contributing factor for attrition within co-infected subgroups. This outcome suggests that prospective testing and follow-up protocols for co-infected patients need to incorporate baseline hepatic impairment assessment.
The present findings are not without their limitations. First, the high specificity of the matching criteria constrains the number of individuals included in the study, which could influence the results. Notwithstanding, attempts to enlarge the sample size by employing a 1∶2 and 1∶3 matching ratio posed further challenges. An increase in the count of individuals with HIV/HCV co-infection could not be proportionally matched with individuals presenting only HIV, thereby upsetting the equilibrium of baseline characteristics between the groups and augmenting the confounding effects. Given these constraints, a 1∶1 matching strategy might constitute an effective compromise. Second, the unavailability of data on HCV RNA and other variants of hepatitis viruses could potentially exaggerate the estimated impacts of chronic HCV infections, while downplaying the effects of concealed hepatitis virus infection. Third, we could not explore HIV- or HCV-related deaths due to the absence of data regarding the cause of death. Despite this, investigating the consequences of HIV/HCV co-infection on all-cause mortality in individuals on long-term ART can provide valuable insights for devising intervention strategies.
To our knowledge, this study is the first to explore the impact of HIV/HCV co-infection on prognostic outcomes in individuals receiving ART derived from a PSM cohort. The outcomes underscore the immediate necessity for tailored testing and follow-up plans for those co-infected with HIV/HCV, contingent upon their initial hepatic impairment classification (10).
-
No conflicts of interest.
HTML
| Citation: |

|