
 Download:
Download:





-
Hand, foot, and mouth disease (HFMD) — predominantly associated with enterovirus infection — is a widespread disease adversely affecting children below the age of five (1). Since HFMD’s designation as a notifiable infectious disease in 2008, its prevalence has consistently topped the charts in China, evolving into the leading cause of disease-related morbidity (2).
However, despite this official classification, a comprehensive understanding of the magnitude of HFMD infections and the economic burden they bear remains elusive. This is largely due to the “iceberg” phenomenon unique to infectious diseases — where the vast majority of HFMD infections exhibit no symptoms, and symptomatic cases might opt against seeking medical treatment at sentinel hospitals, either owing to mild symptoms or financial constraints. This subset constitutes “unconsulted” cases (3). Moreover, due to HFMD symptoms’ similarity to other medical conditions, misdiagnoses are likely (4).
To accurately gauge the economic burden of HFMD in Beijing, our study employs both prospective and retrospective methods to quantify the prevalence and per-person economic strain tied to misdiagnosed and hospital-consulted infections across a range of severity categories. We deployed a Monte Carlo multiplier model to approximate true infection rates.
Our analysis determines that each officially confirmed case of HFMD correlates to 9.1 actual infections [95% confidence interval (CI): 4.6–31.5]. The economic burden per person was as follows: 25.58 United States dollars (USD) for unconsulted cases, 265.75 USD for misdiagnosed cases, 366.50 USD for mild cases, and 2355.89 USD for severe cases. The cumulative annual economic loss attributable to HFMD fluctuates between 7.03 million USD and 13.31 million USD.
In April 2017, we undertook a prospective study in Fengtai District to gauge the morbidity and economic impact of HFMD (Figure 1A). Participants included children aged from 6 to 35 months who had resided in the district for a minimum of 6 months, and the observation period extended from April 2017 to October 2018. Seasoned general practitioners recorded symptoms resembling HFMD, medical consultations, clinical diagnoses, and associated costs and collected pharyngeal samples for testing for Enterovirus (EV).
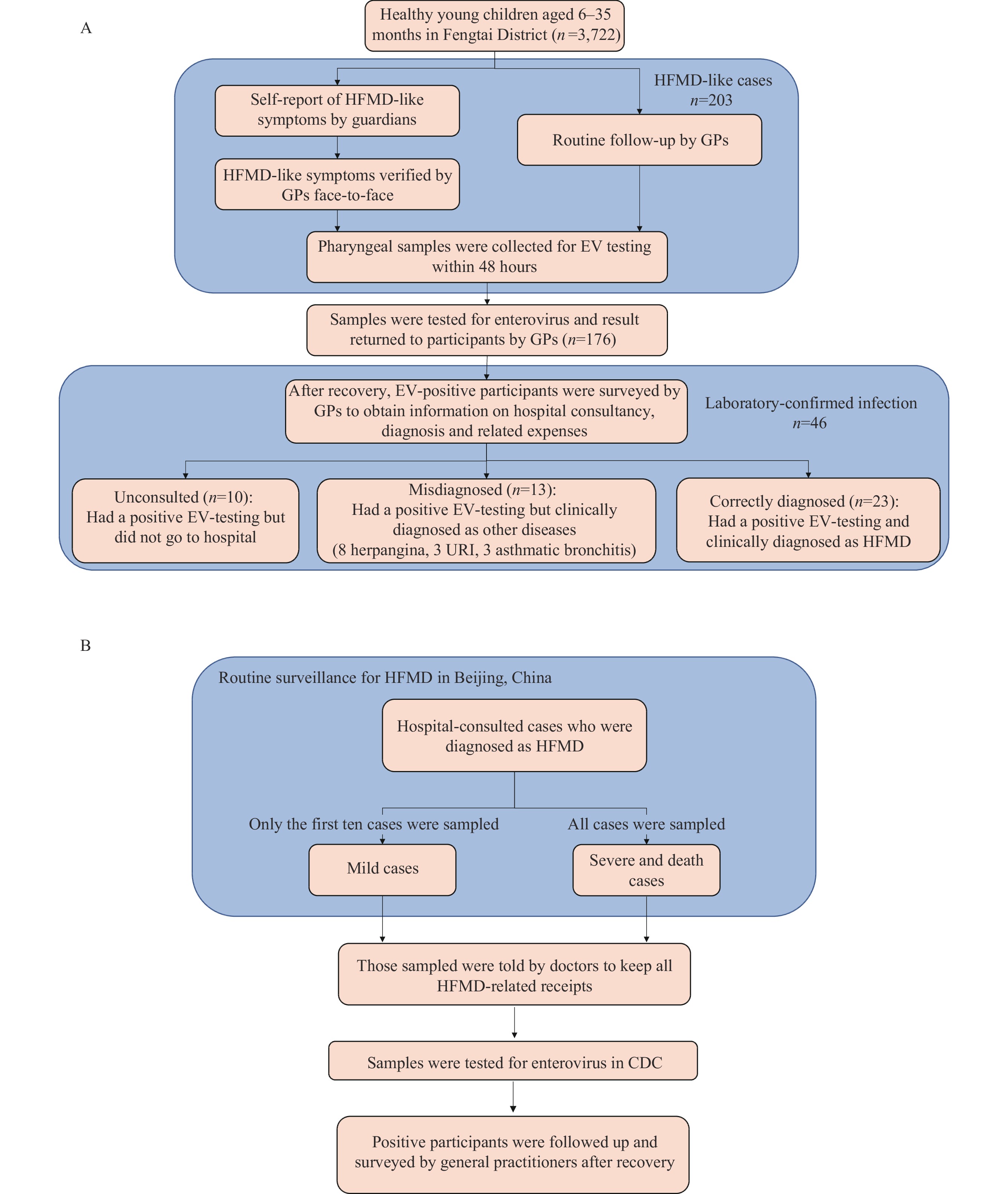 Figure 1.
Figure 1.Flowchart Illustrating the prospective and retrospective study design. (A) Flowchart for the prospective on the actual prevalence of HFMD; (B) Flowchart for retrospective studies on the unit cost of HFMD.
Note: Figure 1A: In April 2017, a prospective study was conducted in Beijing’s Fengtai District, enrolling 3,722 healthy children aged 6 to 35 months, residing in the district for at least six months. Follow-up occurred from April 2017 to October 2018. HFMD-like cases (203) were identified through self-reporting and confirmation by GPs or routine follow-ups. Pharyngeal samples (n=176) were collected within 48 hours of symptom reporting, with 46 testing positive for EV. Post-recovery, GPs surveyed these cases for hospital consultations, diagnoses, and associated costs. Among them, 23 were accurately diagnosed, 13 were misdiagnosed, and 10 did not seek consultation. Figure 1B: This study considered HFMD cases from six sentinel hospitals in Beijing, China. These hospitals collected samples from the initial ten mild HFMD cases each month, or all cases if fewer than ten were reported. Severe and fatal cases were also included. Patients were advised to retain expense receipts for cost calculation. Following positive enterovirus confirmation, patients were monitored and surveyed by community GPs post-recovery to avoid recall bias.
Abbreviation: HFMD=hand, foot, and mouth disease; GPs=General Practitioners; EV=enterovirus.
A parallel retrospective study was also initiated in April 2017 to estimate the economic burden of hospitalized cases, incorporating patients from 6 administrative regions within Beijing (Figure 1B). To circumvent recall bias when calculating the expenses related to HFMD, medical practitioners instructed study participants to retain all documentation relating to HFMD-related expenditures.
We employed the Monte Carlo multiplier model to estimate the actual infection levels of HFMD. We considered parameters such as the symptomatic infection rate, consultation rate, diagnosis rate, and EV-positive rate to deduce the actual infections (
Supplementary Table S1 andSupplementary Figure S1 ). The direct economic burden incorporated personal and reimbursement costs, which included direct medical expenses associated with case treatments, as well as direct non-medical costs such as nutritional and transportation expenses incurred by patients during diagnosis and treatment.Indirect costs factoring in lost labor due to patient care were quantified by multiplying the average daily wage per capita by the average number of days lost. We also considered the economic burden of death cases, accounting for illness-related costs and the loss of societal productivity due to premature death. Cost estimations were performed separately for different infection types.
All statistical analyses were carried out using R software (version 4.2.0, R Foundation for Statistical Computing, Vienna, Austria), and all statistical tests were two-sided with an α value of 0.05.
In April 2017, a prospective study was undertaken in Fengtai District of Beijing. Between September 2017 and August 2018, we recruited 3,722 healthy children into the study. Of this group, 1,965 (53.8%) were male and 1,757 (47.2%) were female. The average age was 1.5 years [standard deviation (SD): 0.6]. After a one-year follow-up period, 203 children presented with symptoms resembling those of HFMD. A total of 176 pharyngeal samples were collected and examined for EV, resulting in 46 (26.1%) positive outcomes. The EV-positive cases consisted of 1 case of EV-A71 (2.2%), 7 cases of coxsackievirus type 16 (CV-A16) (15.2%), 22 cases of CV-A6 (47.9%), and 16 cases of other EV serotypes (34.8%). Of the 46 confirmed infections, 36 (78.3%, 95% CI: 65.9%–90.7%) sought medical care at hospitals. Among these, 23 cases (63.9%, 95% CI: 47.4%–80.4%) were diagnosed with HFMD. The remaining 13 cases were misdiagnosed: 8 with herpangina, 3 with upper respiratory infection, and 2 with asthmatic bronchitis. Consequently, we estimated a hospital consultation rate of 78.3% and a misdiagnosis rate of 36.1% (Figure 1).
A retrospective study was conducted in six districts in Beijing from April 2017 to October 2018. The study encompassed 697 HFMD cases in children aged five years and younger, including 410 males and 287 females. Of these cases, 547 (78.5%) tested positive for EV; CV-A6 had the highest positivity rate at 46.2%, followed by other EV types at 17.5%, CV-A16 at 11.9%, and EV-A71 at 2.9%. Notably, 88 cases (12.6%) were reported in vaccinated individuals, and none of those vaccinated were infected with EV-A71. The overwhelming majority of cases were mild, accounting for 97.7%, while severe cases represented 2.3%. No fatalities were recorded during the study period.
Based on Monte-Carlo multiplier calculations (4–6), each confirmed case corresponds to an estimated 9.1 actual infections (95% CI: 4.6–31.5). Furthermore, one confirmed case is representative of 2.5 (95% CI: 1.9–3.7) actual cases and 2.0 (95% CI: 1.5–2.9) consulting cases.
In the prospective study, each of the 10 untreated HFMD infections represented an economic burden of 25.58 USD per person, with the direct economic burden contributing 22.3% and the indirect economic burden contributing 77.7% (Table 1). The economic burden of the 13 misdiagnosed infections was higher, at 265.75 USD per person, with direct economic costs accounting for 36.7% and indirect economic costs making up the remaining 63.3% (Table 1). In terms of the retrospective study, the economic burden for mild cases averaged 366.50 USD per person, of which the largest portion was for indirect costs (65.5%), followed by direct medical costs (20.7%) and direct non-medical costs (13.8%). For the 16 severe cases, the average economic burden was significantly higher at 2355.89 USD per person, with direct medical costs contributing 60.1%, direct non-medical costs adding 11.1%, and indirect costs accounting for 28.8%. Median and IQR data are detailed in
Supplementary Table S2 .Infection classification† Direct burden Indirect burden Total Medical burden Non-medical burden (95% CI) Unconsulted (n=10) 3.26±2.12 2.44±2.77 19.88±44.67 25.58 (7.83, 43.37) Diagnosed as HFMD Mild (n=681) 75.73±124.64 50.74±99.44 240.03±322.46 366.50 (337.16, 395.86) Severe (n=16) 1415.16±1284.57 261.51±229.88 679.21±405.96 2355.89 (1570.70, 3140.75) Death 2885.43±3302.65 620.68±754.70 280.75±840.46 3786.87 (2777.97, 4796.97) Diagnosed as others (n=13) 62.61±43.53 34.89±19.07 168.25±88.20 265.75 (212.60, 318.90) Abbreviation: SD=standard deviation; USD=United States dollars; CI=confidence interval; HFMD=hand, foot and mouth disease; CNY=Chinese Yuan; CPI=consumer price index.
* The average exchange rate for USD to CNY was noted as 6.4515 in the year 2021. We adjusted all associated costs in accordance with the 2021 CPI.
† Cost estimates for both unconsulted and misdiagnosed cases were derived from our prospective study. Meanwhile, the cost data associated with both mild and severe cases were ascertained through our retrospective study. As for the cost implications of fatal outcomes, these were referenced to Zheng et al., 2013 (10).Table 1. Summary of economic burden per case in Beijing (
$\bar{{x}} $ ±SD in USD*).Annual economic losses attributable to HFMD in Beijing are estimated to range between 7.03 million USD and 13.31 million USD. A mere 2.1% of these losses arise from unconsulted infections. Mild infections consistently account for the largest proportion of these losses, having increased gradually from 65.8% in 2016 to 66.3% in 2018. The contribution of severe infections to the total economic burden varies significantly year by year. Importantly, no deaths were reported in connection with the disease from 2016 to 2019 (Table 2). If calculations are based solely on reported HFMD cases, the 2019 total economic burden would be projected at 0.49 million Chinese Yuan (CNY), thereby underestimating the actual burden by 30%.
Year Unconsulted (%) Hospital Diagnosed Misdiagnosed (%) Total Mild (%) Severe (%) Death (%) 2016 26.6 (2.1) 816.3 (65.8) 12.2 (1) 0 (0) 386.2 (31.1) 1241.4 2017 16.2 (2.1) 498.1 (65.8) 7.3 (1) 0 (0) 235.7 (31.1) 757.2 2018 28.6 (2.1) 877.7 (65.9) 9.9 (0.7) 0 (0) 415.3 (31.2) 1331.5 2019 15.2 (2.2) 466.4 (66.3) 1.2 (0.2) 0 (0) 220.7 (31.4) 703.4 Abbreviation: USD=United States dollars; HFMD=hand, foot and mouth disease; CNY=Chinese Yuan; CPI=consumer price index.
* All costs have been adjusted in accordance with the 2021 CPI. The average exchange rate from USD to CNY in 2021 was 6.4515.Table 2. The estimated morbidity and overall economic burden of HFMD cases in Beijing (10,000 USD*)
-
This study conducted a systematic investigation into the actual morbidity and economic impact of HFMD, revealing an annual economic loss between 7.0 million USD and 13.3 million USD in Beijing, which represents 0.1% of the overall health expenditure. The economic burden attributed to unconsulted cases, mild and severe cases, as well as misdiagnosed cases, remained fairly consistent over the years. The prospective study results indicated that expenditure for each unconsulted HFMD infection averaged 25.58 USD per person, resulting in an anticipated average economic burden of 0.15–0.29 USD million per annum in Beijing. Despite severe HFMD cases resulting in the highest per-person costs among those consulted, they constituted only a minor portion of the overall burden due to their limited prevalence. The research found the economic impact of severe infections to be in line with findings from other regions (7-8). Although the financial loss per mild infection is only one-seventh of that of a severe case, given their high frequency, mild cases contribute significantly to the overall economic impact of HFMD. The study found that only 64% of cases were correctly diagnosed as HFMD upon hospital visits. The resulting costs of treatment for those misdiagnosed aligned with those of correctly diagnosed cases. It is therefore crucial to recognize that overlooking the economic burden born of approximately 35% of misdiagnosed cases would lead to a considerable underestimation of the financial impact of the HFMD disease.
In milder cases, indirect costs predominated — a pattern that diverged notably from the cost distributions seen in other countries (9) and from the nationwide average in China (10), where direct medical costs typically held sway. However, economic disparities between different study areas, including patient demographics and the spectrum of disease severity, might contribute to differences in economic costs. When equated with Shanghai, which had a comparable economic status to Beijing (11), the proportion of indirect costs was alike. Furthermore, in both our study and in Shanghai, a significant portion of the indirect cost was attributed to parental work loss, indicating a strong influence by the average income of citizens.
This study is subject to certain limitations. First, despite efforts to minimize recall bias — such as the retention of all HFMD-related receipts by participants for the calculation of HFMD-linked expenses — the potential for recall bias may still endure. Second, the HFMD severity spectrum in Beijing may vary significantly in comparison to other cities. Hence, the extrapolation of economic burden findings from this study to cities exhibiting radically dissimilar economic statuses and disease spectra should be undertaken with considerable caution.
In conclusion, this study elucidates the true morbidity rate of HFMD cases in Beijing and establishes critical parameters for future estimates of HFMD infections. The evaluation of the economic burden per case and by case category could facilitate cost-effectiveness analyses for HFMD prevention and control strategies.
-
No conflicts of interest.
HTML
| Citation: |

|