

 Download:
Download:




-
A recent retrospective study utilizing data from the China National Mortality Surveillance System has shed light on the mortality rates associated with pulmonary heart disease (PHD) in China. The study found that the age-standardized mortality rate of PHD has significantly decreased from 61.68 per 100,000 in 2014 to 28.53 per 100,000 in 2021. The analysis also revealed that PHD-related deaths primarily occur in older individuals, with those aged over 80 being the most affected. Chronic obstructive pulmonary disease (COPD) was identified as the main underlying cause of death in the majority of PHD cases. Despite the declining trend in mortality rates, the study emphasized the need for continued attention to PHD due to the high prevalence of COPD and the rapid population aging in China. This study provides valuable insights into the current status and trends of PHD-associated mortality, helping healthcare professionals and policymakers understand the impact of PHD on public health in China.
PHD, also referred to as cor pulmonale, is characterized by pulmonary arterial hypertension stemming from conditions, including chronic respiratory disease, chronic thromboembolic pulmonary hypertension, and other diseases impacting the lung’s structure or function. This condition can result in right ventricular enlargement, potentially leading over time to right heart failure (1). PHD was a significant heart disease in China during the latter half of the previous century. From the 1990s, advancements in technology and methodologies have enhanced the treatment and survival rate of this condition. According to the third national retrospective survey on causes of death, the PHD mortality rate was 4.74 per 100,000 (2). However, this mortality rate was based on the underlying cause of death (UCoD) and did not accurately reflect the actual number of PHD related deaths, as many such instances were classified with chronic obstructive pulmonary disease (COPD) as the UCoD. The proportion of PHD deaths attributed to COPD in the Chinese population remains uncertain. Thus, this analysis was conducted using data from the China National Mortality Surveillance System (NMSS) to provide a comprehensive update on PHD related mortality in recent years in China and to investigate the fundamental causes of PHD-related deaths.
-
This research is a retrospective, population-based study of multiple causes of death (MCoD), utilizing mortality data extracted from the NMSS. This system encompasses 24.3% of China’s overall population via 605 disease surveillance points (DSPs), providing representative data on both national and provincial levels. For further details on the NMSS, readers are referred to previously published descriptions (3). To maintain the validity and reliability of the mortality data, the following measures were implemented: workforce training, annual quality control engagements, on-site quality assessments, and the establishment of death registration regulations (3).
To address potential under-reporting, a retrospective survey was conducted triennially, which would then allow for adjustment of the mortality rate. In this present study, the mortality rates from 2014 through 2017 were adjusted using the underreporting rates from the same years, and the rates from 2018 through 2021 were adjusted using the 2017 under-reporting rate. The formula used for adjustment was: “adjusted mortality rate = crude mortality rate / (1 – under-reporting rate)”.
For age-standardized mortality rates, each age group’s crude mortality rates were first adjusted, after which direct standardization was applied. Data about the population of the disease surveillance points was obtained from the National Bureau of Statistics.
In this study, deaths associated with PHD were characterized as those having the International Classification of Disease-10th Version (ICD-10) codes I27.8 or I27.9 in either part of the medical certification section of the death certificate, irrespective of whether they were the UCoD or the associated (non-underlying) cause. Among the total PHD-associated deaths, the UCoD was categorized as follows: tumors (C00‒C97, D00‒D48); ischemic heart disease (I20‒I25); cerebrovascular disease (I60‒I69); COPD (J40‒J44); and other primary causes of PHD including asthma (J45), bronchiectasis (J47), pneumoconiosis (J60–J66), tuberculosis sequelae (B90.9), obesity-hypoventilation syndrome (E66.2), cystic fibrosis (E84.0), sleep apnea syndrome (G47.3), idiopathic interstitial pulmonary fibrosis (J84.1), idiopathic pulmonary arterial hypertension (I27.0), kyphoscoliosis (M41), chronic thromboembolic pulmonary hypertension (I26.9); pulmonary heart disease (I27.8, I27.9); and other diseases. The selection of other primary PHD causes was guided by the 2018 PHD diagnosis and treatment guidelines (4). It should be noted that PHD, being an end-stage disease, is rarely classified as the UCoD. However, in some instances, it may be challenging to trace the primary disease leaving PHD as the only plausible UCoD, hence its inclusion as a separate category here.
The adjusted mortality rate (AMR) and age-standardized mortality rate (ASMR) were evaluated for the years 2014–2021. The demographic data from the 2020 census was utilized as a reference population to directly standardize the population structure throughout the study. The average annual percent changes (AAPCs) were computed using the Joinpoint regression, which facilitated a trend analysis of the ASMR, thereby enabling an exploration into alterations over time according to sex, urban-rural locations, and various regions. All these analyses were executed using the SAS software (version 9.4, SAS Institute Inc., Cary, NC, USA) and the Joinpoint Regression Program (version 4.9.0.1; National Cancer Institute, Rockville, MD, US).
-
In 2021, the total number of PHD associated death was 103,586 (61,634 males, and 41,952 females) across 605 DSPs, leading to an estimated 430,205 PHD deaths nationwide. The ASMR showed a decrease, falling from 61.68 per 100,000 in 2014 to 28.53 per 100,000 in 2021 (AAPC= −10.40 , 95% confidence interval (CI): −12.03 to −8.75), with a reduction of 53.74% (Table 1).
Category 2014 2021 AAPC for ASMR Number AMR ASMR Number AMR ASMR Total 156,418 47.93 61.68 103,586 30.46 28.53 −10.40* (−12.03, −8.75) Gender Male 87,784 52.54 76.14 61,634 35.51 38.14 −9.31* (−11.15, −7.44) Female 68,634 43.10 49.26 41,952 25.20 20.38 −11.80* (−13.24, −10.33) Urban-Rural Urban 39,456 30.39 41.10 25,720 16.94 16.68 −12.26* (−13.82, −10.67) Rural 116,962 59.53 73.93 77,866 41.36 37.08 −9.17* (−10.95, −7.73) Region East 53,685 37.47 44.69 28,223 17.88 16.28 −13.46* (−14.79, −12.11) Central 44,398 45.07 60.42 29,230 30.35 27.50 −10.46* (−13.38, −7.43) West 58,335 69.00 96.62 46,133 53.69 53.84 −7.95* (−11.09, −4.70) Abbreviation: AAPC=average annual percent change; AMR=adjusted mortality rate; ASMR=age-standardized mortality rate; PHD=pulmonary heart disease; DSPs=disease surveillance points.
* P<0.01.Table 1. Number of deaths, ASMR and AMR (per 100,000) of PHD by gender, urban-rural divide, and region in 605 DSPs in 2014 and 2021.
The ASMR exhibited a significant decline in males from 76.14 per 100,000 in 2014 to 38.14 per 100,000 in 2021 (AAPC=−9.31, 95% CI: −11.15 to −7.44). Similarly, in females, ASMR decreased from 49.26 per 100,000 in 2014 to 20.38 per 100,000 in 2021 (AAPC=−11.80, 95% CI: −13.24 to −10.33). The ASMR was reduced by 49.91% in males and 58.63% in females (Table 1).
Significant variations in the ASMR were reported across different regions. Over the study period, the highest ASMR was observed in the west region, higher than that in the central and east regions (Table 1). From 2014 to 2021, there was a decrease in ASMR from 44.69 to 16.28 per 100,000 in the east region (AAPC=−13.46, 95% CI: −14.79 to −12.11). In the central region, it decreased from 60.42 to 27.50 per 100,000 (AAPC=−10.46, 95% CI: −13.38 to −7.43). The west region reported a decrease in ASMR from 96.62 to 53.84 per 100,000 (AAPC=−7.95, 95% CI: −11.09 to −4.70). The decrease of the ASMR corresponded to 63.57%, 54.49%, and 44.28%, respectively.
The ASMR exhibited a significant decrease in both urban and rural areas during the study period. Specifically, the ASMR in urban areas dropped from 41.10 per 100,000 to 16.68 per 100,000 (AAPC=−12.26, 95% CI: −13.82 to −10.67), representing a 59.42% decrease. Meanwhile, in rural areas, the ASMR descended from 73.93 per 100,000 to 37.08 per 100,000 (AAPC=−9.17, 95% CI: −10.95 to −7.37), reflecting a 49.84% reduction (Table 1).
Mortality rates associated with PHD escalated with age, demonstrating a sharp increase after 60–65 age group across all categories (Figure 1). The highest mortality rate was observed in individuals aged over 80. Throughout the study period, a decreasing trend was evident in the mortality rates across all age groups.
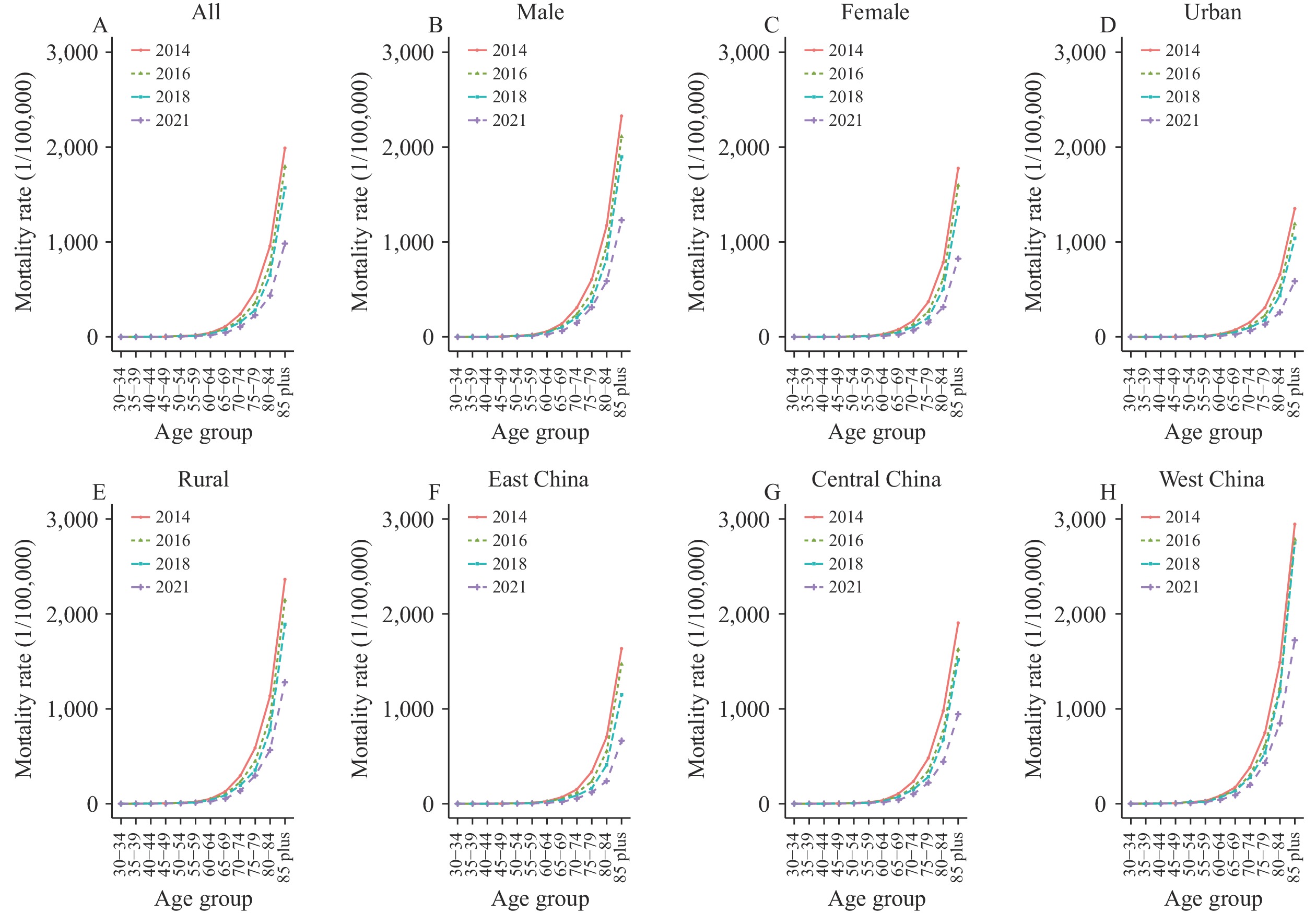 Figure 1.
Figure 1.Trends in age-specific mortality rates for pulmonary heart disease in China in 2014, 2016, 2018, and 2021. Among age groups based on (A) all population, (B–C) sex (male and female), (D–E) residential area (urban or rural), and (F–H) region (East, Central or West China).
Table 2 presents a summary of the underlying causes of PHD-associated deaths from 2014 to 2021. Notably, COPD is identified as the leading underlying cause of these PHD-associated deaths, comprising the majority of total cases.
Underlying cause of death 2014, n (%) 2015, n (%) 2016, n (%) 2017, n (%) 2018, n (%) 2019, n (%) 2020, n (%) 2021, n (%) N*=156,418 N=142,733 N=144,424 N=140,379 N=133,047 N=126,552 N=108,196 N=103,586 Chronic obstructive pulmonary disease 136,725
(87.41)131,343
(92.02)134,324
(93.01)130,864
(93.22)123,830
(93.07)117,280
(92.67)99,918
(92.35)93,928
(90.68)Pulmonary heart disease 14,161
(9.05)5,918
(4.15)4,221
(2.92)3,767
(2.68)3,651
(2.74)3,638
(2.87)3,423
(3.16)5,051
(4.88)Other primary disease of pulmonary heart disease 1,353
(0.86)1,543
(1.08)1,782
(1.23)1,867
(1.33)1,830
(1.38)2,004
(1.58)1,643
(1.52)1,564
(1.51)Ischemic heart disease 937
(0.60)802
(0.56)845
(0.59)770
(0.55)851
(0.64)727
(0.57)647
(0.60)702
(0.68)Tumors 605
(0.39)593
(0.42)612
(0.42)604
(0.43)592
(0.44)530
(0.42)519
(0.48)441
(0.43)Cerebrovascular disease 245
(0.16)198
(0.14)227
(0.16)236
(0.17)239
(0.18)286
(0.23)236
(0.22)241
(0.23)Other disease 2,392
(1.53)2,336
(1.64)2,413
(1.67)2,271
(1.62)2,054
(1.54)2,087
(1.65)1,810
(1.67)1659
(1.60)Abbreviation: PHD=pulmonary heart disease; DSPs=disease surveillance points.
* Total number of PHD-associated deaths.Table 2. Underlying causes of PHD-associated deaths among 605 DSPs in China from 2014 to 2021.
-
Our study’s findings indicate a significant decrease in PHD-associated mortality rates across different genders, urban and rural locales, all regions from 2014 to 2021. This observable decrease could primarily be attributed to advancements in medical conditions, improvements in socioeconomic status, and awakening in health awareness. Moreover, with the expansion of basic health insurance coverage, more individuals are inclined to seek hospital services for their health-related concerns (5). Notably, the western region recorded the highest PHD mortality rate, surpassing the central and eastern regions. Contributing factors to this phenomenon include the slower developmental pace, relative scarcity of healthcare resources, and lower affordability in the western region. Additionally, the higher prevalence of risk factors such as smoking, household air pollution, high altitude, and COPD exacerbate the situation (6–7). Gender disparity in PHD mortality rates was also observed, with males exhibiting higher numbers than females. Such differences could possibly be linked to varying occupational exposures and smoking patterns among Chinese males. The ASMR was shown to be higher in rural areas as compared to urban locations; this discrepancy may be due to varying distribution of risk factors and disparities in medical conditions. Furthermore, the elevated PHD mortality rate among the elderly population can largely be attributed to aging and advancements in PHD treatment.
During the 1970s, PHD featured heavily in overall mortality rates in China, frequently ranking first or second among all causes of death in many areas (8). The first national retrospective survey of causes of death indicated that PHD represented 61.08% of all heart disease cases, with a national ASMR of 63.72 per 100,000 in 1973–1975 (9). From 1990, the DSP system, an antecedent of the NMSS, initiated the collection of death data, releasing crude mortality rates based on the UCoD. Our study diverges from the conventional approach of employing a single underlying cause of death database, preferring instead to use a multiple-cause death database to ascertain the mortality rate for PHD. Despite the challenges inherent in juxtaposing mortality rates from studies with differing definitions of the cause of death, an overall downward trend in PHD mortality was noted (crude mortality rate, 78.86 per 100,000 in 1973–1975 vs. 30.46 per 100,000 in 2021) considering that the mortality rate based on MCoD is higher than that based on UCoD for the same disease.
In the Global Burden of Disease Study 2010 (GBD2010), the entirety of PHD was reassigned to COPD prior to the year 2004. However, in the GBD2013 study, approximately 45% of PHD was reassigned to COPD before the same year. The primary disparity between these two GBD studies pertains to the methods of redistribution of what’s known as “garbage codes.” Wan et al. have commented on the redistribution of PHD and suggested that the proportional redistribution for COPD in GBD2010 seems somewhat more rational (10). Still, given that diseases such as asthma, pneumoconiosis, tuberculosis, and others have also partly accounted for PHD cases, the method in GBD2010 could potentially overestimate the redistribution proportion for COPD. Within our study, we noted that COPD contributed to over 90% of the total PHD cases, which might be somewhat higher than the estimated proportion of 80%–90% presented in earlier literature (1). This discrepancy could be attributed to the high prevalence and the significantly low early diagnosis and treatment rates for COPD patients observed in China (11).
This research delivers the latest PHD mortality statistics within the Chinese population, leveraging nationwide surveillance data. The scope of this analysis encapsulates all reported PHD-associated deaths, thus capturing a holistic picture of the PHD burden. It must be highlighted that commonly used UCoD analyses often omit other comorbidities. Limitations intrinsic to our study need acknowledgement as well. First, under-reporting, particularly in the western region, might lead to an underestimation of the PHD mortality rate. Second, the completeness of a deceased individual’s prior disease history on the death certificate can also influence the calculation of mortality rates. For instance, when PHD patients directly die from acute myocardial infarction and the coder does not include PHD as a contributing cause of death listing in the part two of the medical certification section of the death certificate, PHD-associated mortality will be underestimated. Lastly, the diagnosis rate of PHD in rural areas may be sub-par, further leading to potential underestimation of mortality rates.
In conclusion, a decreasing trend in PHD mortality rate was observed in China from 2014 to 2021, with a substantial number of these fatalities attributed to COPD. Nonetheless, the high prevalence of COPD, coupled with the rising phenomenon of an aging populace, could pose some uncertainty towards future PHD mortality rates. Therefore, it is imperative for clinicians to closely monitor changes in cardiac structure and functionality, particularly in poorly controlled or treated COPD patients, thus mitigating the potential progression of COPD to PHD. Moreover, consistent surveillance and prompt updating of PHD mortality data is vital for enhancing preventive strategies and control measures.
-
The provincial and local Centers for Disease Control and Prevention across China.
HTML
| Citation: |

|