
 Download:
Download:




-
Carbapenem-resistant Enterobacteriaceae (CRE) infections, specifically those involving New Delhi metallo-beta-lactamase (NDM) drug-resistant bacteria, continue to pose challenges for healthcare institutions. High-risk coronavirus disease 2019 (COVID-19) patients are susceptible to developing secondary bacterial coinfections, with CRE coinfections reportedly having significant implications for COVID-19 prognosis. In this report, we present a unique case of a NDM-producing bacterial coinfection following COVID-19 infection.
In late December 2022, a hospital in Beijing admitted an elderly female patient who had been infected with COVID-19 for three weeks. Subsequent laboratory tests revealed a persistent urinary tract infection (UTI) lasting over 45 days, caused by community-acquired NDM-5 Escherichia coli. Genomic analyses demonstrated that the infection was not the result of a single strain but rather a group of clonally related, chromosomally indistinguishable E. coli strains with varying acquisitions or losses of drug-resistance plasmids. During the course of the infection, a novel drug-resistance plasmid recombined within the patient.
This case highlights the continuous evolution of drug-resistant bacterial strains during infections and suggests that the intestinal tract may serve as a source for the gene pool.
A unique case was identified in a hospital in Beijing involving a patient admitted from December 29, 2022, to January 13, 2023. CRE E. coli was isolated from both the patient’s sputum and urine on December 31, 2022. Medical records and clinical test results were collected for analysis. The patient was followed up twice to isolate the multidrug-resistant organisms (MDRO): urine and feces samples were collected on January 26, 2023, and additional urine, feces, and sputum samples were obtained on February 17, 2023. A urine routine test was also conducted on February 17, 2023. Concurrently, control samples were collected from the patient’s live-in nanny on February 17, 2023.
The antibiotic sensitivity of the strains was evaluated using minimum inhibitory concentrations (MICs) testing using VITEK® 2 COMPACT (bioMérieux, Marcy-l'Étoile, France), and blaNDM genes were detected and sequenced in positive samples (1). All strains underwent molecular typing with MLST (2), and whole-genome sequencing was carried out using PacBio Sequel (Pacific Biosciences, Menlo Park, USA) and Illumina NovaSeq (Illumina, San Diego, USA) technologies. Antibiotic resistance genes were predicted using ResFinder 4.1 (Technical University of Denmark, Kongens Lyngby, Denmark) (3).
Genomic synteny between two plasmids was visualized using ACT release 13.0.0 (Wellcome Trust Sanger Institute, Cambridge, UK). Primers were designed and amplified for all assembled plasmids identified through whole-genome analysis (
Supplementary Table S1 ). A phylogenetic tree based on the core chromosomal genome was constructed using the neighbor-joining method (4–6). Additionally, a NJ tree for plasmids and associated megaBLAST hits was developed based on pairwise alignments.The patient, a 93-year-old woman with a smoking history of over 75 years, tested positive for COVID-19 antigen three weeks prior. In early and mid-December 2022, she experienced a fever that peaked at 38.7 ℃, accompanied by mild chills. At that time, she was severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) antigen-positive. Subsequently, her body temperature returned to normal without the use of antipyretics. She self-medicated with a second-generation cephalosporin antibiotic for three weeks without medical consultation. Around December 20, 2022, she sustained burns to her neck, face, and auricle due to smoking while inhaling oxygen at home. Approximately two days later, she developed a low-grade fever, exhibited a decreased appetite, and showed signs of mental fatigue.
On December 29, 2022, the patient was admitted to the hospital for persistent discomfort following the COVID-19 infection and neck and facial burns. She did not report any urinary tract discomfort during admission or hospitalization and denied any abnormal discharge. On the day of admission, PCR tests for SARS-CoV-2, influenza A, influenza A (H1N1), seasonal influenza A (H3), and influenza B were all negative, and antibody testing for Mycoplasma pneumoniae was also negative. As the SARS-CoV-2 infection had resolved at least two weeks prior, Paxlovid was not indicated. The treatment focused on maintaining oxygenation status, managing water and electrolyte balance, and addressing the skin burns.
Due to elevated blood neutrophil levels on admission (Table 1), a bacterial infection was suspected. Consequently, moxifloxacin was added to the treatment regimen at a dosage of 0.4 g intravenously per day, commencing on December 31, 2022, and ceasing on January 6, 2023. The patient was discharged on January 13, 2023, due to improvement in her condition.
Clinical tests December 29, 2022 December 31, 2022 January 5, 2023 January 9, 2023 February 17, 2023 Blood White blood cell 8.95×109 9.85×109 5.6×109 5.81×109 − Neutrophil count 7.03×109 8.49×109 3.71×109 3.85×109 − Neutrophil (%) 78.50 86.20 66.10 66.20 − Lymphocyte count 1.03×109 0.79×109 1.2×109 1.15×109 − Lymphocyte (%) 11.50 8.00 21.40 19.80 − Monocytes count 0.82×109 0.53×109 0.58×109 0.62×109 − Monocytes (%) 9.20 5.44 10.30 10.70 − ESR (mm/h) 65 − 74 − − CK (U/L) 102.6 280.8 74.3 − − CRP (mg/L) 56.3 94.0 8.8 6.4 − SAA (mg/L) 311.8 392.2 66.9 23.6 − PCT (ng/L) <0.05 <0.05 <0.05 <0.05 − D-Dimer (mg/L) 3.10 − 1.21 1.07 − Urine Leukocytes in the urine (p/HPF) − 128.77 104.03 14.48 168.83 Red blood cells in the urine (p/HPF) − 1.40 3.56 5.19 0.96 Bacteria count in the urine (p/HPF) − 3177.32 912.81 729.26 1002.55 Note: “–” means data not available.
Abbreviation: ESR=erythrocyte sedimentation rate; CK=creatine kinase; CRP=C reactive protein; SAA=serum amyloid A; PCT=procalcitonin.Table 1. Significant clinical test results for the patient following COVID-19 infection — Beijing, China, 2023.
CRE was isolated from the patient’s urine and sputum on December 31, 2022, from her urine on January 5, 2023, and from her urine and feces on January 26, 2023, and February 17, 2023. No CRE was isolated from the patient’s live-in nanny at any time point. All strains isolated from the patient carried the blaNDM-5 gene (accession numbers OQ357728, OQ357729, OQ442328, OQ442329, OQ442330, OQ851640, and OQ851641). The antimicrobial resistance spectra of NDM-5-producing E. coli indicated two types, which differed between the strains isolated from urine and sputum on December 31, 2022, with respect to gentamicin, tobramycin, and trimethoprim/sulfamethoxazole (Table 2). To exclude non-CRE E. coli infection, the blaNDM gene positivity rate among 95 E. coli isolates acquired from urine on February 17, 2023, was determined to be 88.42%. The antimicrobial resistance results for gentamicin, tobramycin, and trimethoprim/sulfamethoxazole of these NDM-producing E. coli isolates were identical (Table 2). The patient was admitted to a new ward that opened on December 21, 2022. No MDRO had been detected in the ward’s environment or among other patients from the ward’s opening until four weeks after the patient with NDM-5-producing E. coli was discharged (December 21, 2022 to February 10, 2023). The patient had not been hospitalized in the past three years, suggesting that the NDM-5-producing E. coli was community-acquired.
Antibiotic December 31, 2022 January 5, 2023 January 26, 2023 February 17, 2023 Urine Sputum Urine Urine Feces Urine Feces MIC (μg/mL) Interpretation MIC (μg/mL) Interpretation MIC (μg/mL) Interpretation MIC (μg/mL) Interpretation MIC (μg/mL) Interpretation MIC (μg/mL) Interpretation MIC (μg/mL) Interpretation Ampicillin ≥32 R ≥32 R ≥32 R ≥32 R ≥32 R ≥32 R ≥32 R Ampicillin/sulbactam ≥32 R ≥32 R ≥32 R ≥32 R ≥32 R ≥32 R ≥32 R Piperacillin/tazobactam ≥128 R ≥128 R ≥128 R ≥128 R ≥128 R ≥128 R ≥128 R Cefazolin ≥64 R ≥64 R ≥64 R ≥64 R ≥64 R ≥64 R ≥64 R Cefotetan ≥64 R ≥64 R ≥64 R ≥64 R ≥64 R ≥64 R ≥64 R Ceftazidime ≥64 R ≥64 R ≥64 R ≥64 R ≥64 R ≥64 R ≥64 R Ceftriaxone ≥64 R ≥64 R ≥64 R ≥64 R ≥64 R ≥64 R ≥64 R Cefepime ≥64 R ≥64 R ≥64 R ≥64 R ≥64 R ≥64 R ≥64 R Aztreonam ≥64 R 16 R ≥64 R 16 R 16 R 16 R 16 R Ertapenem ≥8 R ≥8 R ≥8 R ≥8 R ≥8 R ≥8 R ≥8 R Imipenem ≥16 R ≥16 R ≥16 R ≥16 R ≥16 R ≥16 R ≥16 R Amikacin ≤2 S ≤2 S ≤2 S ≤2 S ≤2 S ≤2 S ≤2 S Gentamicin ≥16 R ≤1 S ≥16 R ≤1 S ≤1 S ≤1 S ≤1 S Tobramycin ≥16 R ≤1 S ≥16 R ≤1 S ≤1 S ≤1 S ≤1 S Ciprofloxacin ≥4 R ≥4 R ≥4 R ≥4 R ≥4 R ≥4 R ≥4 R Levofloxacin ≥8 R ≥8 R ≥8 R ≥8 R ≥8 R ≥8 R ≥8 R Nitrofurantoin ≤16 S ≤16 S ≤16 S ≤16 S ≤16 S ≤16 S ≤16 S Trimethoprim/ Sulfamethoxazole ≥320 R ≤20 S ≥320 R ≤20 S ≤20 S ≤20 S ≤20 S Note: S=sensitive; R=resistant; MIC=minimum inhibitory concentration. Table 2. Spectrum of antibiotic resistance among blaNDM-5 strains isolated from the patient following COVID-19 infection — Beijing, China, 2023.
A group of NDM-5-producing E. coli strains were isolated four times from a patient, and they shared the same chromosomes (CP123592, CP123593). Each of these strains carried four plasmids, three of which were identical: pDJH_Plas_NDM-5 (CP123590), pDJH_Plas3 (CP123589), and pDJH_Plas4 (CP123594). The distinct plasmids were pDJH_137urine_Plas1 (CP123591) and pDJH_183sputum_Plas2 (CP123595) (
Supplementary Table S2 ). Figure 1 displays the timeline of strain isolation, genomic composition, and homology analysis.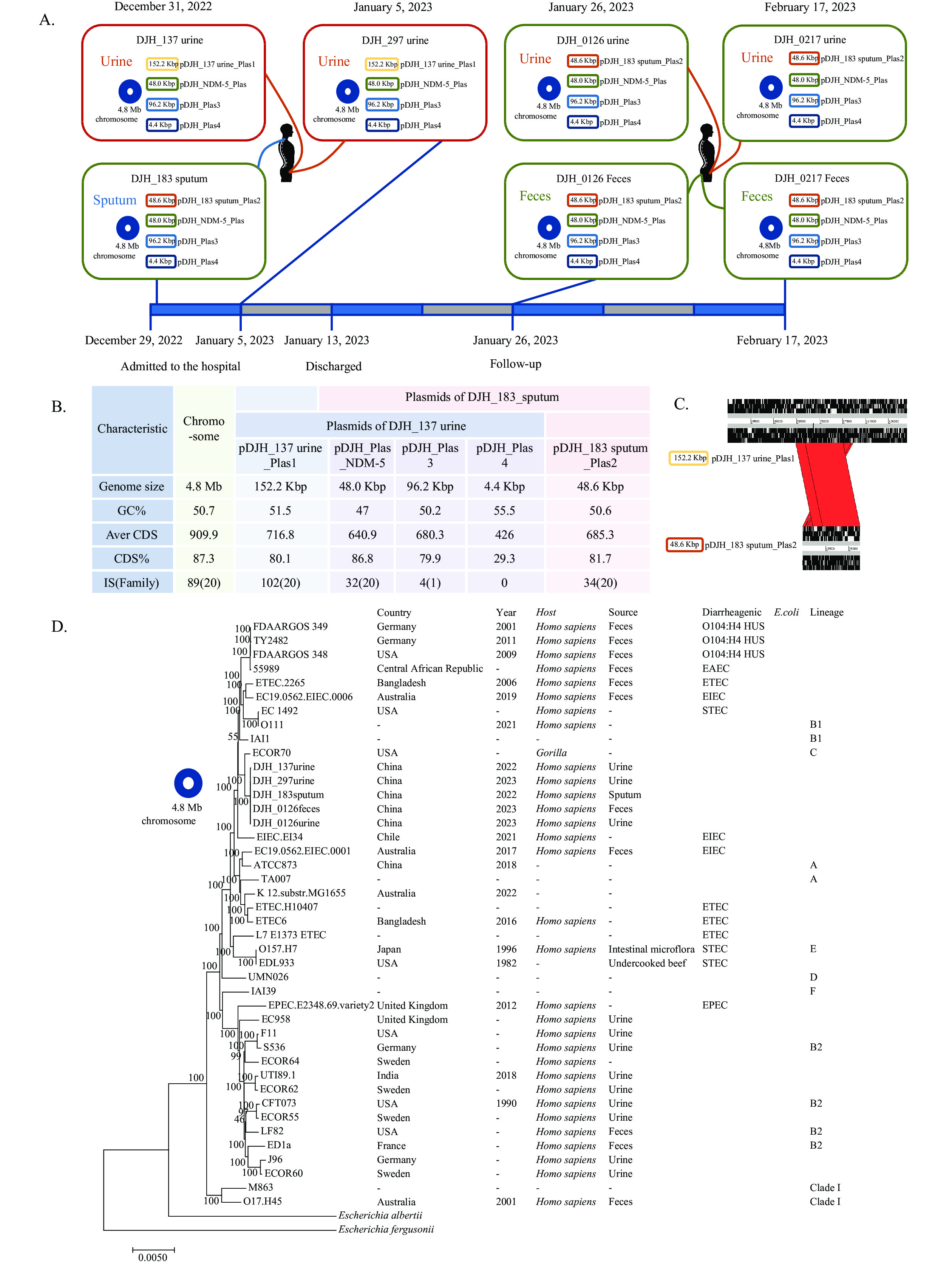
All NDM-5 E. coli strain sequence types were identified as ST 410, which is distinct from the common uropathogenic E. coli (UPEC) strains. The chromosome size was 4.8 Mb, with a G+C content of 50.67 mol%. A NJ tree, including the five sequenced strains and representative strains from each lineage, was divided into two branches. The E. coli chromosome in this study was part of branch C, which was relatively distant from most UPEC strains. The nearest human strain was enteroinvasive E. coli (EIEC) with a chromosome size of 4.8 Mb and G+C content of 50.7 mol%.
Common virulence factors of UPEC such as fimH, afa, fyuA, hlyA, iucABCD, kpsF, and sfa were found within the chromosome. Notably, type I fimbriae (fimH) plays a crucial role in UPEC’s ability to colonize the urethral epithelium and migrate to the bladder. Additionally, the chromosome encodes for the locus of enterocyte effacement (LEE) (7-8).
The pDJH_Plas_NDM-5 is a 48Kbp IncX3 plasmid that carries the blaNDM-5 gene. It has a similar backbone to blaNDM-5 plasmids of various sources, which range from 46,155 to 53,056 bp in size, with 84% (42/50) of them being 46,161 bp. None of the top 50 megaBlast hits was the same size as Plas_NDM-5 of 48,020 bp. The extra sequences in this case encoded IS91 family transposase and a putative protein of unknown function. pDJH_Plas_NDM-5 plasmid remained stable after 70 passages in vitro.
The pDJH_183sputum_Plas2 plasmid (48.6 Kbp) exhibited 31.87% coverage and 99.78% identity when compared with pDJH_137urine_Plas1 (152.2 Kbp), suggesting their homology. The top megaBLAST hit demonstrated 96% coverage and 99.87% identity with pDJH_183sputum_Plas2. In contrast, the top hit for pDJH_137urine_Plas1 revealed only 67% coverage, implying that it was not a pre-existing plasmid but rather a newly emerged plasmid. The pDJH_183sputum_Plas2 plasmid encodes the blaTEM-1B gene, which mediates resistance to ampicillin, cephalothin, piperacillin, and ticarcillin. The pDJH_137urine_Plas1 plasmid encodes 11 resistance genes that mediate resistance to 30 types of antibiotics across seven categories: sulfonamides, aminoglycosides, phosphomycin, macrolides, tetracyclines, β-lactams, and acyl alcohol.
The differences in drug resistance between strains DJH_183sputum and DJH_137urine (Table 2), specifically concerning compound sulfonamides, gentamicin, and tobramycin, were attributed to the presence of dfrA12, sul2, and aac(3)-IV, which were exclusively found in the pDJH_137urine_Plas1 plasmid. Therefore, it was deduced that pDJH_137urine_Plas1 originated from recombination with pDJH_183sputum_Plas2 and acquired new resistance genes within the patient’s body. Initially, on December 31, 2022, the patient’s urine and sputum strains carried these two plasmids, respectively. On January 5, 2023, the urine strain (JARVKQ000000000) harbored pDJH_137urine_Plas1. However, after January 26, 2023, only pDJH_183sputum_Plas2 was detected in isolated strains (JARVKR000000000, JARVKS000000000), indicating that pDJH_137urine_Plas1 was not stably maintained, while pDJH_183sputum_Plas2 was (Figure 1A).
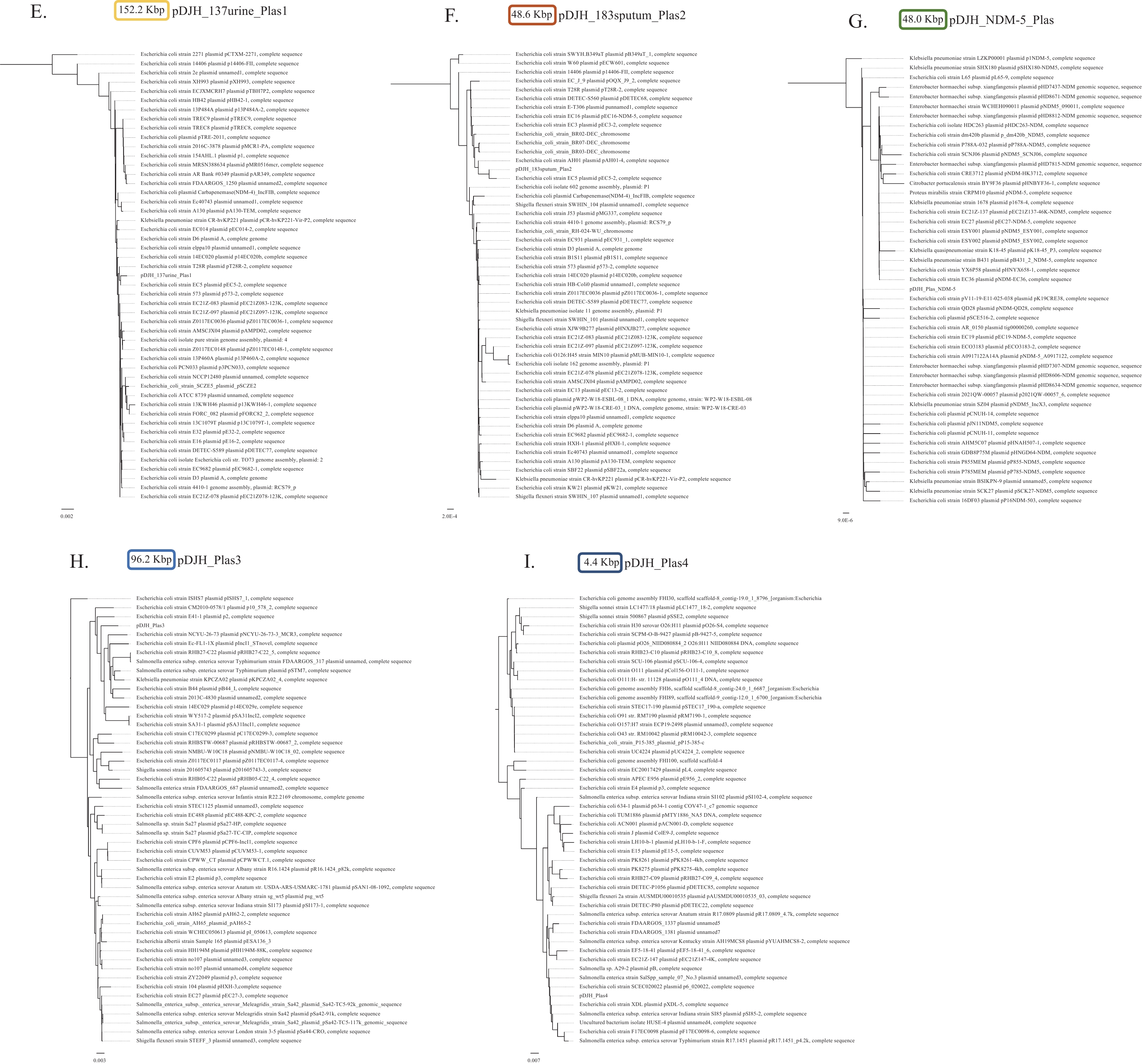 Figure 1.
Figure 1.Comparative genome analysis and timeline of the isolation of blaNDM-5 E. coli strains from the patient following COVID-19 infection — Beijing, China, 2023. (A) Isolation source and genomic composition of the strains. (B) Genomic properties of the chromosome and plasmids of the strains isolated on December 31, 2022. (C) Genomic synteny between pDJH_137urine_Plas1 and pDJH_183sputum_Plas2 plasmids. (D) Neighbor-joining tree based on the core genome of the E. coli strains isolated on December 31, 2022, January 5, 2023, and January 26, 2023, and E. coli representatives from each phylogroup. (E) Neighbor-joining tree of pDJH_137urine_Plas1 and the top 50 megaBLAST hits using BLAST pairwise alignments. (F) Neighbor-joining tree of pDJH_183sputum_Plas2 and the top 50 megaBLAST hits using BLAST pairwise alignments. (G) Neighbor-joining tree of pDJH_Plas_NDM-5 and the top 50 megaBLAST hits using BLAST pairwise alignments. (H) Neighbor-joining tree of pDJH_Plas3 and the top 50 megaBLAST hits using BLAST pairwise alignments. (I) Neighbor-joining tree of pDJH_Plas4 and the top 50 megaBLAST hits using BLAST pairwise alignments.
Abbreviation: IS=Insertion Sequence; EAEC=Enteroaggregative Escherichia coli; ETEC=Enterotoxigenic Escherichia coli; EIEC=Enteroinvasive Escherichia coli; STEC=Shiga toxin-producing Escherichia coli.The other two plasmids, pDJH_Plas3 (96.2 Kbp) and pDJH_Plas4 (4.4 Kbp), do not carry any resistance genes.
-
The diagnostic criteria for a UTI include clinical symptoms and the presence of a pathogen. Pyuria, or the presence of white blood cells or pus in the urine, serves as a significant indicator (9). Although the patient in this study did not report any subjective UTI symptoms, NDM-5 E. coli was isolated from her urine four times over a period of 45 days, accompanied by noticeable bacteriuria and pyuria (Table 1). Consequently, a diagnosis of persistent UTI was made. The NDM-5 E. coli infection in this case was likely community-acquired, with the bacteria being selectively eliminated in vivo due to the patient’s at-home use of a second-generation cephalosporin. The spread of the bacterial strains appeared to be limited, as the patient’s nanny did not contract the infection.
Interestingly, the NDM-5 E. coli was not a single clone but rather a group of homologous E. coli strains. These strains possessed the same chromosome but carried different plasmids and were present concurrently in multiple systems (e.g., the urethra and the respiratory tract, the urethra and the intestinal tract). Following the cessation of antibiotics, the pDJH_137urine_Plas1 plasmid, which conferred a broader drug resistance spectrum, gradually disappeared. In contrast, the less-drug-resistant plasmid pDJH_183sputum_plasmid2 remained within the NDM-5 E. coli population (Figure 1A).
The source of the patient’s infection was investigated by collecting and analyzing their fecal samples twice after their discharge from the facility. In both instances, NDM-5 E. coli strains were isolated. Previous research has identified the intestinal tract as a reservoir for antibiotic-resistance genes (1,10). The patient also reported habitually wiping her perineal area from back to front after bowel movements. It was hypothesized that the E. coli strains’ plasmids underwent recombination within the gastrointestinal tract and were subsequently transferred to the urinary tract due to the patient’s wiping habit. Virulence genes, such as fimH, facilitated the strains’ colonization along the epithelial cells of the urinary tract. Coincidentally, the bacterial strain carrying the NDM-5 plasmid, which conferred extensive antibiotic resistance, led to a persistent UTI.
In the present case, a rare occurrence of community-acquired NDM-5 E. coli UTI persisted for over 45 days. Two NDM-5 strains were identified, both having the same chromosome but with homologous and recombined plasmids. This finding suggests that multidrug-resistant bacteria were not stable throughout the infection. While new plasmids can be acquired, the plasmids themselves may also undergo constant recombination, leading to variations in antibiotic resistance profiles. This case implies that a diverse range of resistance genes may be intrinsic to the human body, and the CRE could undergo recombination as a consequence of environmental pressures, such as those imposed by antibiotic usage. The intestinal tract might serve as the source of the gene pool. Therefore, in contrast to exogenous infection, more attention should be given to endogenous factors contributing to the development of CRE.
-
No conflicts of interest.
-
Charlesworth Author Services (Paper no.117766) for their critical editing and helpful comments regarding our manuscript.
HTML
| Citation: |

|