
 Download:
Download:




-
Suicide constitutes a significant global public health issue, as it accounts for one out of every hundred deaths (1). Although the suicide rate has experienced a decline in China, this decrease has gradually slowed, with certain sub-populations even witnessing a reverse trend and an increase in rates (2). Consequently, suicide remains an area of public health concern. Gaining a comprehensive understanding of the factors correlating with suicidal behaviors among high-risk populations is essential for addressing this issue effectively.
Serious mental disorders (SMD) represent significant public health concerns globally. Official reports indicate that approximately 4.7% of individuals in China experience SMD (3). Individuals with mental disorders exhibit a higher risk for suicidal behaviors compared to the general population. A meta-analysis revealed that the pooled suicide rate among SMD patients was 312.8 per 100,000 (4).
An increasing number of studies have examined the primary causes of suicidal behaviors among psychiatric inpatients; however, limited information is available regarding the prevalence and associated factors of suicidal behaviors among community SMD patients. These community patients are often more exposed to negative reactions and perceptions from their external environment (5). Consequently, there may be a disparity in suicidal behaviors between community patients and inpatients. To effectively prevent suicidal behaviors among community SMD patients in China, public health policymakers need to consider both prevalence and associated factors.
The cross-sectional study was conducted from August 2022 to September 2022 in Shandong Province, China. A randomized multistage stratified cluster sampling technique was employed for the study. Initially, the gross domestic product (GDP) of 16 administrative districts in Shandong Province was utilized to classify high and low economic zones within the province, resulting in the random selection of one city from each category (Jinan and Zaozhuang). Subsequently, one county from each city (Zhangqiu and Taierzhuang) was randomly selected. Following this step, six towns and streets were chosen at random from each county. Registered community SMD patients in the 12 towns and streets were then considered for the study. Ultimately, a total of 486 registered community SMD patients participated in the study.
All interviewers underwent training in communication techniques and received detailed information on the research and questionnaire materials prior to the study. Participants voluntarily provided written, fully informed consent. Patients capable of communicating were interviewed individually (n=37), while those unable to communicate were interviewed through their primary caregivers (n=449) using a proxy-informant-based approach. The differences in patients' characteristics answered between patients themselves and caregivers are shown in the
Supplementary Table S1 . Legal guardians were asked to provide informed consent on behalf of patients who were illiterate, below 18 years of age, or unable to communicate. Questionnaires were administered via face-to-face interviews between the interviewers and respondents, with interviewers completing the questionnaires based on the information received from the interviewees. Following the study, at least two trained postgraduate students checked the content and quality of the questionnaires; those with missing or unclear information were revisited and updated accordingly.Suicidal ideation, suicide plans, and suicide attempts were assessed using three questions “During your lifetime, have you seriously considered committing suicide or taking your own life?”, “During your lifetime, have you ever made a plan to commit suicide or take your own life” and “During your lifetime, have you ever attempted to commit suicide or tried taking your own life?”. Response options included “no” and “yes”. Participants who responded “yes” to the first question were subsequently asked the latter two questions, whereas those who responded “no” were not asked further.
Religious beliefs in the study comprised none, Buddhism, Christianity, Catholicism, and others, with “none” coded as 0 and all other responses coded as 1. The Brief Psychiatric Rating Scale (BPRS), which assesses the severity of psychiatric symptoms, was administered by locally trained psychiatric professionals.
Statistical analyses were conducted using IBM SPSS Statistics (web version 24.0; New York, USA). Descriptive statistics were employed to examine means and standard deviations for continuous variables with normal distributions, as well as numbers and percentages for categorical variables. Additionally, the frequency and percentages of suicidal behaviors were described based on gender and age group. Analysis of variance (ANOVA) and chi-square tests were utilized to compare suicidal behaviors concerning socio-demographic variables, illness information, and unhealthy behaviors. Multivariable logistic regressions were applied to examine variables related to suicidal ideation, suicide plans, and suicide attempts. All tests were two-sided, with P<0.05 indicating statistical significance.
In the study, 210 (43.2%) male and 276 (56.8%) female participants were included, with 25.9% of patients being older than 65 years. The majority of patients were of Han ethnicity, married, had no religious affiliation, resided in rural areas, had children, and were not only child. A small percentage of patients engaged in alcohol use (8.4%) and cigarette smoking (14.2%). Furthermore, 37.0% of patients lived in impoverished families, and 27.8% were in debt. In total, 44.7% of the patients with SMD had other chronic diseases. Each patient lived with an average of 2.84 individuals, including themselves, and the mean BPRS score was 55.47 [standard deviation (SD)=21.19]. The majority of patients were diagnosed with schizophrenia (63.6%), followed by epileptic mental disorder (14.2%) and bipolar disorder (12.1%). Descriptive and single analyses of suicidal behaviors are presented in Table 1.
Variable Overall Suicidal ideation P-value Suicide plan P-value Suicide attempt P-value Yes No Yes No Yes No Numbers (%) 486 (100.0) 179 (36.8) 307 (63.2) 87 (17.9) 399 (82.1) 73 (15.0) 413 (85.0) Age, n (%) 0.034 0.868 0.797 ≤44 years 156 (32.1) 45 (28.8) 111 (71.2) 26 (16.7) 130 (83.3) 23 (14.7) 133 (85.3) 45–64 years 204 (42.0) 80 (39.2) 124 (60.8) 37 (18.1) 167 (81.9) 33 (16.2) 171 (83.8) ≥65 years 126 (25.9) 54 (42.9) 72 (57.1) 24 (19.0) 102 (81.0) 17 (13.5) 109 (86.5) Gender, n (%) 0.039 0.090 0.300 Male 210 (43.2) 66 (31.4) 144 (68.6) 30 (14.3) 180 (85.7) 27 (12.9) 183 (87.1) Female 276 (56.8) 113 (40.9) 163 (59.1) 57 (20.7) 219 (79.3) 46 (16.7) 230 (83.3) BMI, mean (SD) 24.68 (4.34) 25.22 (4.41) 24.36 (4.27) 0.036 25.29 (4.55) 24.55 (4.28) 0.146 25.67 (4.76) 24.50 (4.24) 0.033 Ethnicity, n (%) 0.978 1.000 1.000 Han 482 (99.2) 177 (36.7) 305 (63.3) 86 (17.8) 396 (82.2) 72 (14.9) 410 (85.1) Others 4 (0.8) 2 (50.0) 2 (50.0) 1 (25.0) 3 (75.0) 1 (25.0) 3 (75.0) Religious belief, n (%) Yes 66 (13.6) 36 (54.5) 30 (45.5) 0.002 15 (22.7) 51 (77.3) 0.354 14 (21.2) 52 (78.8) 0.184 No 420 (86.4) 143 (34.0) 277 (66.0) 72 (17.1) 348 (82.9) 59 (14.0) 361 (86.0) Marital status, n (%) <0.001 0.019 0.204 Unmarried 105 (21.6) 20 (19.0) 85 (81.0) 9 (8.6) 96 (91.4) 10 (9.5) 95 (90.5) Married 328 (67.5) 135 (41.2) 193 (58.8) 67 (20.4) 261 (79.6) 54 (16.5) 274 (83.5) Divorced/widowed 53 (10.9) 24 (45.3) 29 (54.7) 11 (20.8) 42 (79.2) 9 (17.0) 44 (83.0) Education, n (%) 0.105 0.619 0.599 Illiterate 163 (33.5) 53 (32.5) 110 (67.5) 26 (16.0) 137 (84.0) 21 (12.9) 142 (87.1) Primary school 138 (28.4) 47 (34.1) 91 (65.9) 28 (20.3) 110 (79.7) 21 (15.2) 117 (84.8) Junior high school or above 185 (38.1) 79 (42.7) 106 (57.3) 33 (17.8) 152 (82.2) 31 (16.8) 154 (83.2) Region, n (%) 1.000 1.000 0.401 Rural 436 (89.7) 161 (36.9) 275 (63.1) 78 (17.9) 358 (82.1) 68 (15.6) 368 (84.4) Urban 50 (10.3) 18 (36.0) 32 (64.0) 9 (18.0) 41 (82.0) 5 (10.0) 45 (90.0) Occupation, n (%) 0.122 0.351 0.616 Employed 210 (43.2) 86 (41.0) 124 (59.0) 42 (20.0) 168 (80.0) 34 (16.2) 176 (83.8) Unemployed 276 (56.8) 93 (33.7) 183 (66.3) 45 (16.3) 231 (83.7) 39 (14.1) 237 (85.9) Offspring, n (%) <0.001 0.024 0.154 Yes 371 (76.3) 154 (41.5) 217 (58.5) 75 (20.2) 296 (79.8) 61 (16.4) 310 (83.6) No 115 (23.7) 25 (21.7) 90 (78.3) 12 (10.4) 103 (89.6) 12 (10.4) 103 (89.6) Only child, n (%) 0.310 0.664 1.000 Yes 24 (4.9) 6 (25.0) 18 (75.0) 3 (12.5) 21 (87.5) 4 (16.7) 20 (83.3) No 462 (95.1) 173 (37.4) 289 (62.6) 84 (18.2) 378 (81.8) 69 (14.9) 393 (85.1) NPLT, mean (SD) 2.84 (1.20) 2.67 (1.15) 2.94 (1.23) 0.015 2.70 (1.06) 2.87 (1.23) 0.224 2.75 (1.05) 2.86 (1.23) 0.488 Years of SMD, mean (SD) 23.41 (13.41) 22.96 (13.75) 23.67 (13.22) 0.574 21.76 (13.80) 23.77 (13.32) 0.205 21.75 (14.05) 23.70 (13.29) 0.253 Alcohol use, n (%) 0.839 0.721 0.876 Yes 41 (8.4) 14 (34.1) 27 (65.9) 6 (14.6) 35 (85.4) 7 (17.1) 34 (82.9) No 445 (91.6) 165 (37.1) 280 (62.9) 81 (18.2) 364 (81.8) 66 (14.8) 379 (85.2) Cigarette smoking, n (%) 0.574 0.697 0.254 Yes 69 (14.2) 28 (40.6) 41 (59.4) 14 (20.3) 55 (79.7) 14 (20.3) 55 (79.7) No 417 (85.8) 151 (36.2) 266 (63.8) 73 (17.5) 344 (82.5) 59 (14.1) 358 (85.9) Poor family, n (%) 0.350 1.000 0.701 Yes 180 (37.0) 61 (33.9) 119 (66.1) 32 (17.8) 148 (82.2) 29 (16.1) 151 (83.9) No 306 (63.0) 118 (38.6) 188 (61.4) 55 (18.0) 251 (82.0) 44 (14.4) 262 (85.6) In debt, n (%) 0.225 0.053 0.078 Yes 135 (27.8) 56 (41.5) 79 (58.5) 32 (23.7) 103 (76.3) 27 (20.0) 108 (80.0) No 351 (72.2) 123 (65.0) 228 (35.0) 55 (15.7) 296 (84.3) 46 (13.1) 305 (86.9) Chronic disease, n (%) <0.001 0.178 0.319 Yes 217 (44.7) 99 (45.6) 118 (54.4) 45 (20.7) 172 (79.3) 37 (17.1) 180 (82.9) No 269 (55.3) 80 (29.7) 189 (70.3) 42 (15.6) 227 (84.4) 36 (13.4) 233 (86.6) BPRS, mean (SD) 55.47 (21.19) 61.21 (21.85) 52.12 (20.09) <0.001 64.01 (20.79) 53.60 (20.85) <0.001 65.59 (21.65) 53.68 (20.63) <0.001 Depressive symptoms, mean (SD) 9.71 (6.25) 12.54 (6.96) 8.06 (5.13) <0.001 13.30 (7.14) 8.93 (5.75) <0.001 13.41 (7.15) 9.06 (5.84) <0.001 Types of SMD, n (%) <0.001 <0.001 0.015 Schizophrenia 309 (63.6) 116 (37.5) 193 (62.5) 53 (17.2) 256 (82.8) 46 (14.9) 263 (85.1) Bipolar disorder 59 (12.1) 36 (61.0) 23 (39.0) 22 (37.3) 37 (62.7) 16 (27.1) 43 (72.9) Epileptic mental disorder 69 (14.2) 21 (30.4) 48 (69.6) 9 (13.0) 60 (87.0) 8 (11.6) 61 (88.4) Others 49 (10.1) 6 (12.2) 43 (87.8) 3 (6.1) 46 (93.9) 3 (6.1) 46 (93.9) Note: NPLT was counted including patients.
Abbreviation: BMI=body mass index; SD=standard deviation; NPLT=the number of persons living together; SMD=serious mental disorders; BPRS=brief psychiatric rating scale.Table 1. Descriptive and single analysis for suicidal behaviors among community SMD patients.
Furthermore, 63.2% of patients exhibited no suicidal behavior. There were significant differences in the prevalence of any suicidal behavior between males and females (χ2=4.639, P<0.05). Among the ideators, 18.1% had a plan, while 3.7% did not have a plan. In the case of attempters, 0.8% had a plan and 14.2% did not have a plan.
Figure 1 illustrates the percentages of suicidal behaviors across various age groups. Among these groups, patients aged 65–69 exhibited the highest percentage of suicidal ideation (47.3%), while those aged 55–59 demonstrated the highest percentages of both suicide planning and suicide attempts (31.0% and 29.3%, respectively). The percentages of suicidal ideation in younger patients showed a significant increase (P<0.01), whereas the percentages of suicide planning and attempts in the 55–59 age group significantly increased (P<0.05) and those in the 60–64 age group significantly declined (P<0.05).
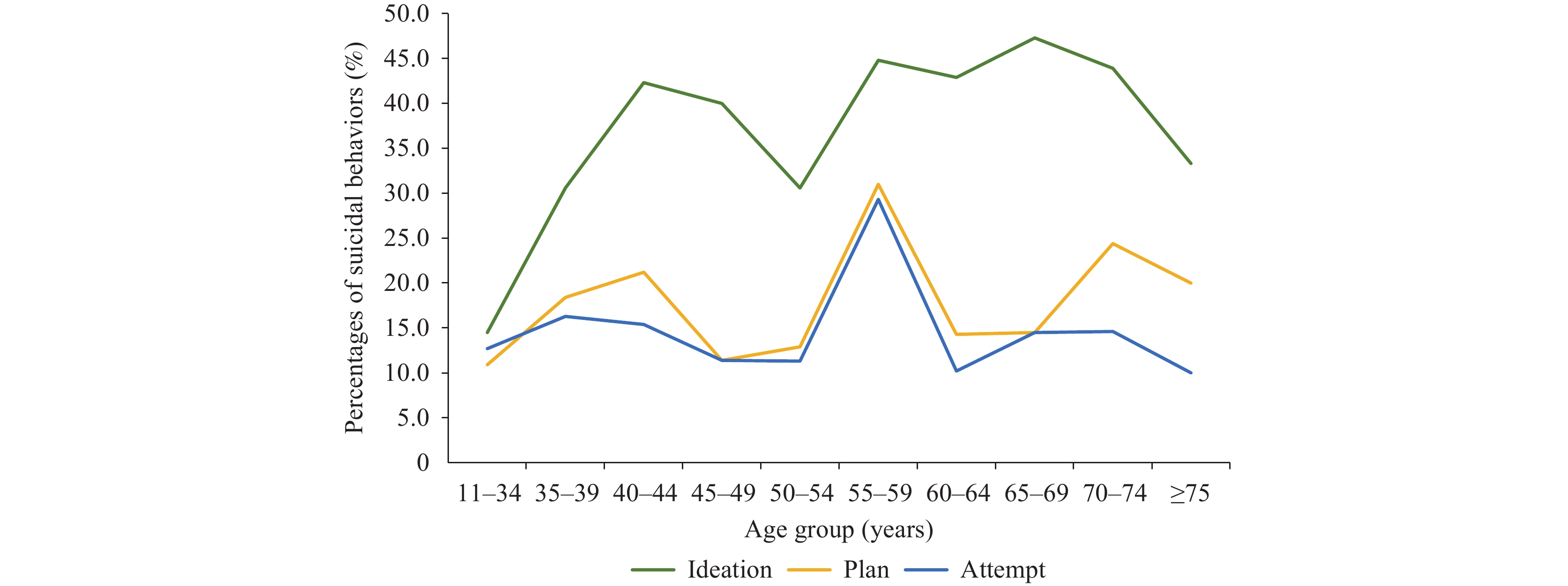 Figure 1.
Figure 1.Percentages of suicidal ideation, suicide plan, and suicide attempts across various age groups.
The logistic regression results for suicidal behaviors are presented in Table 2. Depressive symptoms were found to be significantly associated with suicidal behaviors [odds ratio (OR)=1.13, 95% confidence interval (CI): 1.09–1.18; OR=1.10, 95% CI: 1.05–1.15; OR=1.10, 95% CI: 1.05–1.15]. After adjusting for depressive symptoms, both religious belief and the number of persons living together including patients (NPLT) emerged as significant factors associated with suicidal ideation. Patients without a religious belief (OR=0.46, 95% CI: 0.26–0.81) and more NPLT (OR=0.80, 95% CI: 0.66–0.98) demonstrated a lower likelihood of experiencing suicidal ideation. Additionally, NPLT was significantly linked to suicide plans, with patients living with more individuals being less likely to consider such plans (OR=0.77, 95% CI: 0.60–0.98).
Variable Suicidal ideation Suicidal ideation Suicide plan Suicide plan Suicide attempt Suicide attempt Crude OR (95% CI) Adjusted OR (95% CI) Crude OR (95% CI) Adjusted OR (95% CI) Crude OR (95% CI) Adjusted OR (95% CI) Age (reference=younger patients) 45–64 years 1.59 (1.02, 2.49)* 0.81 (0.44, 1.51) 1.10 (0.64, 1.92) 0.54 (0.26, 1.14) 1.12 (0.63, 1.99) 0.73 (0.33, 1.59) ≥65 years 1.85 (1.13, 3.03)* 0.89 (0.42, 1.91) 1.18 (0.64, 2.17) 0.54 (0.22, 1.35) 0.90 (0.46, 1.77) 0.62 (0.23, 1.66) Male 0.66 (0.45, 0.96)* 0.85 (0.48, 1.49) 0.64 (0.40, 1.04) 0.80 (0.34, 1.24) 0.74 (0.44, 1.23) 0.75 (0.36, 1.56) BMI 1.05 (1.00, 1.09)* 1.02 (0.97, 1.08) 1.04 (0.99, 1.10) 1.01 (0.95, 1.08) 1.06 (1.00, 1.13)* 1.04 (0.98, 1.11) Han ethnicity 0.58 (0.81, 4.16) 0.51 (0.06, 4.22) 0.65 (0.07, 6.34) 0.31 (0.25, 3.72) 0.53 (0.05, 5.14) 0.26 (0.19, 3.56) No religious belief 0.43 (0.26, 0.73)** 0.42 (0.23, 0.77)** 0.70 (0.38, 1.32) 0.72 (0.35, 1.45) 0.61 (0.32, 1.16) 0.61 (0.30, 1.26) Marital status (reference=unmarried) Married 2.97 (1.74, 5.07)*** 2.97 (0.75, 11.76) 2.74 (1.31, 5.71)** 3.15 (0.64, 15.49) 1.87 (0.92, 3.82) 1.43 (0.27, 7.48) Others 3.52 (1.70, 7.28)** 2.87 (0.72, 11.46) 2.79 (1.08, 7.24)* 2.76 (0.55, 13.79) 1.94 (0.74, 5.12) 1.19 (0.22, 6.35) Education (reference=junior high school or above) Illiterate 0.65 (0.42, 1.00) 0.75 (0.41, 1.38) 0.87 (0.50, 1.54) 1.24 (0.59, 2.61) 0.74 (0.40, 1.34) 1.02 (0.47, 2.22) Primary school 0.69 (0.44, 1.09) 0.66 (0.38, 1.16) 1.17 (0.67, 2.05) 1.42 (0.73, 2.75) 0.89 (0.49, 1.63) 0.93 (0.46, 1.88) Rural 1.04 (0.57, 1.91) 1.02 (0.49, 2.14) 0.99 (0.46, 2.13) 0.90 (0.38, 2.14) 1.66 (0.64, 4.34) 1.52 (0.53, 4.38) Employed 1.37 (0.94, 1.98) 1.52 (0.96, 2.40) 1.28 (0.81, 2.04) 1.53 (0.88, 2.66) 1.17 (0.71, 1.94) 1.40 (0.78, 2.52) Offspring 2.56 (1.57, 4.17)*** 0.70 (0.18, 2.69) 2.18 (1.14, 4.16)* 0.66 (0.15, 2.99) 1.69 (0.88, 3.26) 1.04 (0.21, 5.15) Only child 0.56 (0.22, 1.43) 0.70 (0.20, 2.40) 0.64 (0.19, 2.21) 0.66 (0.15, 2.84) 1.14 (0.38, 3.43) 1.23 (0.31, 4.92) NPLT 0.82 (0.70, 0.96)* 0.75 (0.61, 0.93)* 0.88 (0.73, 1.08) 0.74 (0.57, 0.96)* 0.93 (0.75, 1.15) 0.84 (0.64, 1.10) Years of SMD 1.00 (0.98, 1.01) 1.00 (0.98, 1.02) 0.99 (0.97, 1.01) 0.99 (0.97, 1.02) 0.99 (0.97, 1.01) 0.99 (0.97, 1.02) Alcohol use 0.88 (0.45, 1.73) 0.92 (0.40, 2.13) 0.77 (0.31, 1.89) 0.78 (0.27, 2.26) 1.18 (0.50, 2.78) 1.22 (0.43, 3.46) Cigarette smoking 1.20 (0.72, 2.02) 1.57 (0.77, 3.21) 1.20 (0.63, 2.27) 1.46 (0.62, 3.43) 1.55 (0.81, 2.95) 1.87 (0.79, 4.41) Poor family 0.82 (0.56, 1.20) 0.91 (0.57, 1.46) 0.99 (0.61, 1.60) 1.13 (0.64, 1.99) 1.14 (0.69, 1.90) 1.24 (0.68, 2.25) In debt 1.31 (0.88, 1.97) 0.95 (0.57, 1.59) 1.67 (1.02, 2.73)* 1.47 (0.81, 2.65) 1.66 (0.98, 2.80) 1.35 (0.72. 2.54) Chronic disease 1.98 (1.36, 2.88)*** 1.23 (0.77, 1.97) 1.41 (0.89, 2.25) 0.79 (0.44, 1.41) 1.33 (0.81, 2.19) 0.80 (0.43, 1.49) BPRS 1.02 (1.01, 1.03)*** 1.01 (1.00, 1.02)* 1.02 (1.01, 1.03)*** 1.02 (1.00, 1.03)* 1.03 (1.01, 1.04)*** 1.02 (1.00, 1.03)* Depressive symptoms 1.13 (1.10, 1.17)*** 1.13 (1.09, 1.18)*** 1.12 (1.07, 1.16)*** 1.10 (1.05, 1.15)*** 1.11 (1.07, 1.16)*** 1.10 (1.05, 1.15)*** Types of SMD (reference=others) Schizophrenia 4.31 (1.78, 10.43)** 3.33 (1.19, 9.31)* 3.17 (0.95, 10.59) 2.63 (0.70, 9.88) 2.68 (0.80, 8.99) 1.89 (0.51, 7.09) Bipolar disorder 11.22 (4.12, 30.54)*** 6.83 (2.08, 22.44)** 9.12 (2.53, 32.84)** 7.70 (1.80, 32.91)** 5.71 (1.55, 20.96)** 4.05 (0.94, 17.55) Epileptic mental disorder 3.14 (1.16, 8.49)* 1.99 (0.63, 6.31) 2.30 (0.59, 8.98) 1.73 (0.40, 7.55) 2.01 (0.51, 8.00) 1.30 (0.29, 5.81) Note: NPLT was counted including patients;younger patients denote patients younger than or equal to 44 years old.
Abbreviation: BMI=body mass index; NPLT=the number of persons living together; SMD=serious mental disorders; BPRS=Brief Psychiatric Rating Scale; OR=odds ratio; CI=confidence interval.
* P<0.05.
** P<0.01.
*** P<0.001.Table 2. Logistic regression analysis for suicidal behaviors among community SMD patients.
Higher BPRS scores were associated with an increased likelihood of suicidal behaviors (OR=1.02, 95% CI: 1.01–1.03; OR=1.03, 95% CI: 1.01–1.04; OR=1.03, 95% CI: 1.01–1.04). Compared to patients with other SMD, those diagnosed with schizophrenia (OR=3.33, 95% CI: 1.19–9.31) and bipolar disorder (OR=6.83, 95% CI: 2.08–22.44) exhibited a higher propensity for suicidal ideation. Furthermore, bipolar disorder patients were more likely to have a suicide plan (OR=7.70, 95% CI: 1.80–32.91).
-
The findings of this study revealed a higher prevalence of suicidal ideation and suicide attempts (36.8%, 15.0%) among community-based patients with SMD than previously reported in a study focusing on inpatients with schizophrenia spectrum disorders (17.9%, 7.6%) (6). Additionally, the results indicated that 18.1% of community-based patients experienced ideation without a plan or attempt, and 15.0% of patients were attempters. In contrast, a study conducted in Sichuan Province found that 11.0% of psychiatric inpatients only considered suicide, while 27.6% attempted suicide (7). This comparison suggests that community-based patients exhibit a higher prevalence of suicidal ideation, but a lower prevalence of suicide attempts compared to psychiatric inpatients. The disparity might be attributed to the differing social and community environments experienced by community-based patients and inpatients. The presence of family attachment and support for community-based patients could potentially contribute to a reduced risk of suicide attempts.
When age was categorized into three groups, the prevalence of suicidal ideation and suicide plans increased with age. This finding aligns with a previous study indicating that older adults exhibited significantly higher suicide intent compared to younger and middle-aged adults (8). Moreover, the study also discovered that middle-aged patients demonstrated relatively high proportions of suicidal ideation, with the exception of those aged 50–54, while only patients aged 55–59 demonstrated relatively high percentages of suicide plans and attempts. This finding could suggest that community SMD patients contemplated suicide, but they did not act on these thoughts due to emotional stability, as well as a lack of motivation or courage to develop a plan or attempt suicide. Younger patients likely received family care and supervision, while older patients may have come to accept the reality of their long-term illness. However, community patients aged 55–59 might have experienced dual pressure from both their offspring and their patients, possibly leading to feelings of hopelessness regarding their recovery.
Community SMD patients with more severe depressive symptoms demonstrated a higher likelihood of engaging in suicidal behaviors, a finding consistent with previous research. Individuals without religious beliefs were found to be less susceptible to suicidal ideation. This aligns with prior studies, which reported a positive association between religious beliefs and suicide risk for non-political believers (9). Additionally, community patients living with more people exhibited a lower probability of considering and planning suicide. For these patients, cohabiting with family members provided opportunities to share their feelings, potentially reducing negative emotions and suicidal ideation. Furthermore, patients diagnosed with bipolar disorder were found to have an increased risk of suicidal ideation and planning.
The severity of psychiatric symptoms was found to be significantly associated with suicidal behaviors; however, the ORs were close to 1. One possible explanation for this finding is that the BPRS was primarily designed for assessing schizophrenia. In this study, however, patients with SMD included other diagnostic categories. Furthermore, other studies have also reported that the BPRS scores were not significantly associated with suicidal behaviors (10). Most notably, only a few correlated factors were identified. This suggests that the underlying nature of their illness may have influenced the likelihood of suicidal behaviors.
This study was subject to several limitations. First, the study employed a retrospective and cross-sectional design, which raised uncertainty regarding the causal relationships among socio-demographic factors, psychiatric symptom severity, and suicidal behaviors. Additionally, recall bias may have influenced the documented outcomes. Second, interviews with caregivers of patients who lacked communication abilities may have led to an underestimation of the results. Third, although the BPRS can assess psychotic symptoms, potential differences in symptoms among SMDs may have introduced bias to the findings. Finally, the results may not be generalizable, as a broader range of participants would be necessary to ensure the applicability of the outcomes to a wider population.
In summary, early identification and management of associated factors can effectively prevent the development of suicidal ideation and the progression to suicidal actions, ultimately reducing the overall suicide rate. Special attention should be given to the risk of suicide among community-based patients with SMD, particularly those who have religious beliefs, live alone, exhibit severe depressive symptoms, or experience pronounced psychiatric symptoms. It is crucial for governmental agencies and healthcare administrators to provide additional support and welfare programs for middle-aged community patients to alleviate their stress and mitigate their potential for suicide.
-
No conflicts of interest.
-
All the patients and their caregivers.
HTML
| Citation: |

|