
 Download:
Download:




-
The economic burden caused by chronic obstructive pulmonary disease (COPD) exacerbation in patients can lead to significant financial strain. However, limited evidence is available from cohort studies that examine the economic burden of exacerbations and the potential cost savings associated with vaccination in China. To address this gap, we conducted a prospective intervention cohort study to determine the economic burden of three adverse outcomes in COPD patients. We also estimated the cost savings associated with influenza and 23-valent pneumococcal polysaccharide vaccine (PPSV23) vaccination, as well as their combined use. Trivalent influenza vaccine (TIV) is a synthetic vaccine composed of three inactivated influenza viruses, including two types of influenza type A strains and one influenza type B strain, while PPSV23 protects against 23 different types of pneumococcus that cause pneumococcal disease. Our study showed that COPD patients experienced a high economic burden due to exacerbations and pneumonia, particularly hospitalization cases. However, vaccination with influenza vaccine and PPSV23, either separately or in combination, was associated with significantly reduced costs. These findings support the current vaccination recommendations for COPD patients and highlight the potential value of vaccination programs for disease management.
COPD is a chronic respiratory disease that is preventable and treatable. The disease burden of COPD is significant worldwide and in China (1-2). Patients with COPD frequently have acute exacerbations [acute exacerbation of chronic obstructive pulmonary disease (AECOPD)], which can lead to a further decline in lung function, aggravating the progression of the disease, increasing the risk of death, and creating a financial burden for families (3). AECOPD often result from infections with pneumococcus and influenza viruses (3). Immunization against influenza and pneumococcal diseases can reduce the risk and severity of these infections, easing the burden of AECOPD, pneumonia, and hospitalizations in COPD patients (4).
A prospective intervention study was conducted in Tangshan City, Hebei Province, China from November 2018 to November 2020. Vaccination was offered in November 2019. In this study, doctors from the respiratory outpatient clinics of ten hospitals recruited eligible patients between September and October 2018. The patients had a ratio of post-bronchodilator one-second forced expiratory volume (FEV1) to forced vital capacity (FVC) of less than 0.70 (1). Those who had received influenza vaccine during the 2018–2019 influenza season or PPSV23 in the past 5 years were excluded.
Our study utilized standardized questionnaires to collect data on fundamental characteristics, such as age, gender, occupation, COPD severity, comorbidities, and smoking status, as well as the occurrence and associated costs of three outcomes: AECOPD, pneumonia, and hospitalization related to these conditions during a 2-year period. We defined coal miners as individuals who worked or had worked in coal mining. Severity ratings for COPD were consistent with international standards (1). Comorbidities were defined as any other diagnosed diseases except COPD. Smoking was defined as the act of smoking at the time of participation in the study. The case definitions for AECOPD, pneumonia, and related hospitalization can be found in our previously published paper (4). To ensure data accuracy, we cross-checked outcome occurrences and associated cost data according to medical records of subjects’ medical visits and hospitalizations, health insurance reimbursement records, and original invoices. Cost information included outpatient expenses, hospitalization expenses, self-purchased medicine expenses, work-loss expenses (as calculated by salary per day multiplied by the number of work-loss days), and other related expenses. One year into the 2-year study, we offered TIV and PPSV23. Subjects chose to receive either, both, or neither vaccine, resulting in four distinct groups: TIV group, PPSV23 group, TIV&PPSV23 group, and an unvaccinated group. The Sanofi Pasteur and Merck Corporation produced the TIV and PPSV23 used in this study, respectively (Figure 1).
 Figure 1.
Figure 1.The study flow chart.
Abbreviation: COPD=chronic obstructive pulmonary disease; TIV=trivalent influenza vaccine; PPSV23=23-valent pneumococcal polysaccharide vaccine; AECOPD=acute exacerbation of chronic obstructive pulmonary disease.The software programs EpiData (version 3.1, EpiData Software, Epi Info V6, Denmark) and SAS (version 9.4, SAS Institute, Cary, NC, USA) were utilized for data entry and statistical analyses. The basic characteristics of subjects were compared using either chi-squared or Fisher’s exact probability testing. Non-parametric testing was conducted to compare the cost per person and cost per instance of different outcomes. Statistical significance was considered for P-values<0.05.
The Ethical Review Committee of the Chinese Center for Disease Control and Prevention provided the necessary approval for this study (Ethical Approval Notification Nos. 201826 and 201940). Prior to enrollment and vaccination, all participants provided written informed consent.
The study included 762 subjects who completed the study, with 109 receiving TIV, 69 receiving PPSV23, 296 receiving both vaccines, and 288 receiving no vaccine. Significant differences between groups were noted regarding age, occupation, comorbidities, and current smoking (
Supplementary Table S1 ). The unvaccinated group had the lowest average age, the lowest percentage of subjects with comorbidities, and the highest percentage of non-smokers.During the 2-year follow-up study period, a total of 486 cases of AECOPD, 223 cases of pneumonia, and 368 COPD-related hospitalizations were reported. Among these, 355 (73%) AECOPDs, 161 (72%) cases of pneumonia, and 250 (68%) COPD-related hospitalizations occurred in the year prior to vaccination. The frequency of AECOPDs, pneumonia, and related hospitalizations varied by month, with the highest frequency occurring from October to December and the lowest frequency from August to September (Figure 2). A previous publication reported on the incidence densities of AECOPD, pneumonia, and related hospitalization before and after vaccination within three vaccination groups (4). For the unvaccinated group, the number of AECOPD, pneumonia, and related hospitalization outcomes before and after vaccination were 52 and 30, 27 and 15, and 42 and 28, respectively. The corresponding incidence densities were 18.06/100 person-year and 10.42/100 person-year, 9.38/100 person-year and 5.21/100 person-year, 14.58/100 person-year and 9.72/100 person-year.
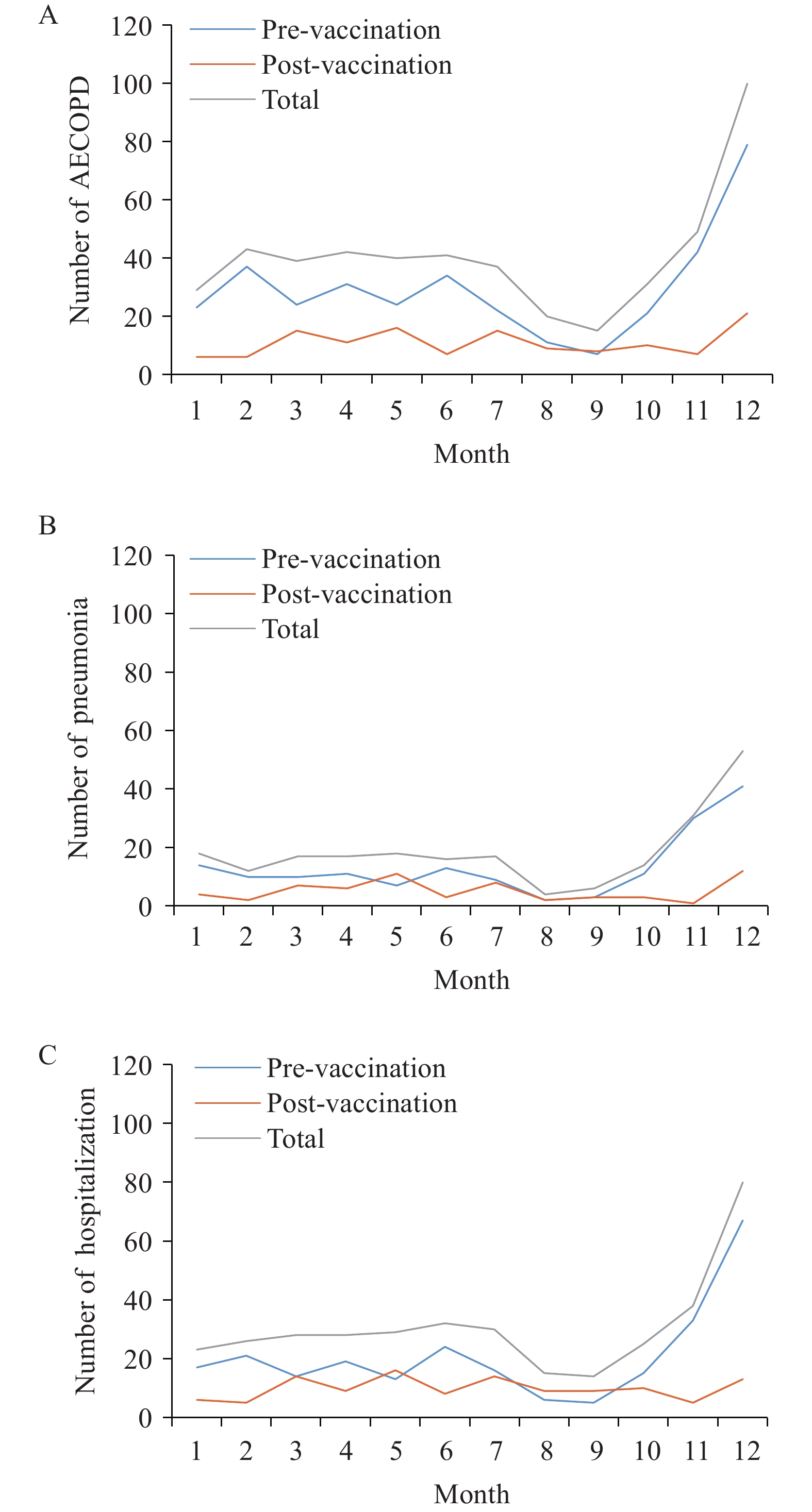 Figure 2.
Figure 2.Distribution of incidence of AECOPDs, pneumonia, and hospitalizations by month. (A) Month distribution of AECOPDs, (B) Month distribution of pneumonia, (C) Month distribution of hospitalizations.
Abbreviation: AECOPD=acute exacerbation of chronic obstructive pulmonary disease.The study results showed that the total cost incurred by subjects who experienced AECOPD, pneumonia, and related hospitalization was 3,912,985 CNY. Outpatient visits accounted for 3.10% of the total cost, while hospitalizations, self-purchased medication, work-loss, and other related expenses accounted for 83.47%, 0.91%, 8.43%, and 4.09%, respectively. A breakdown of these costs by study group and period is provided in Table 1.
Groups Total expenses Outpatient expenses Proportion (%) Hospitalization expenses Proportion (%) Self-purchased medicine expenses Proportion (%) Work-loss expenses Proportion (%) Other related expenses Proportion (%) TIV group Pre- 448,553.9 13,082.7 2.92 378,732.5 84.43 3,530.0 0.79 33,158.7 7.39 20,050.0 4.47 Post- 210,646.9 2,650.0 1.26 177,715.9 84.37 1,861.0 0.88 19,800.0 9.40 8,620.0 4.09 P 0.04 <0.001 0.12 0.24 0.19 0.01 PPSV23 group Pre- 298,823.0 20,335.3 6.81 208,316.0 69.71 5,085.0 1.70 54,416.7 18.21 10,670.0 3.57 Post- 237,367.6 5,148.6 2.17 191,599.0 80.72 2,620.0 1.10 31,170.0 13.13 6,830.0 2.88 P 0.23 0.001 0.56 0.04 0.02 0.20 TIV&PPSV23 group Pre- 1,193,468.4 33,564.4 2.81 1,008,669.9 84.52 8,106.0 0.68 83,688.0 7.01 59,440.0 4.98 Post- 625,897.3 28,570.8 4.56 507,948.9 81.16 2,476.0 0.40 52,811.7 8.44 34,090.0 5.45 P <0.001 <0.001 <0.0001 <0.001 0.001 <0.001 Unvaccinated group Pre- 488,660.3 9,354.5 1.91 434,474.8 88.91 5,221.0 1.07 29,990.0 6.14 9,620.0 1.97 Post- 409,567.3 8,446.7 2.06 358,754.9 87.59 6,558.0 1.60 24,927.7 6.09 10,880.0 2.66 P 0.26 0.44 0.49 0.50 0.43 0.92 Abbreviation: TIV=trivalent influenza vaccine; PPSV23=23-valent pneumococcal polysaccharide vaccine. Table 1. Composition of total expenses (in CNY) across different groups, one year prior to and following vaccination.
The study also found that in the year after vaccination, the total expenses, outpatient expenses, and other related expenses in the TIV group were statistically lower compared to the year before vaccination. Similarly, all types of expenses in the TIV&PPSV23 group and outpatient expenses, self-purchased drug expenses, and work-loss expenses in the PPSV23 group were also significantly lower in the year after vaccination compared to the year before vaccination (Table 1).
During the 2-year follow-up, 505 outcome-related events were reported. Of those, 92 were AECOPD alone, 4 were pneumonia alone, 41 were AECOPD and pneumonia, 190 were AECOPD and hospitalization, 15 were pneumonia and hospitalization, and 163 were AECOPD, pneumonia, and hospitalization. Among them, 82 AECOPD alone, 4 pneumonia alone, 36 AECOPD and pneumonia, 129 AECOPD and hospitalization, 13 pneumonia and hospitalization, and 108 AECOPD, pneumonia, and hospitalization occurred during the year prior to vaccination. Meanwhile, 10 AECOPD alone, 0 pneumonia alone, 5 AECOPD and pneumonia, 61 AECOPD and hospitalization, 2 pneumonia and hospitalization, and 55 AECOPD, pneumonia, and hospitalization occurred during the year following vaccination. The costs per instance of the six outcome combinations were 770.0 CNY for AECOPD alone, 1,423.5 CNY for pneumonia alone, 1,054.9 CNY for AECOPD and pneumonia, 1,0650.0 CNY for AECOPD and hospitalization, 9,047.2 CNY for pneumonia and hospitalization, and 10,007.5 CNY for AECOPD, pneumonia, and hospitalization, respectively. There were no significant differences in most of the costs per instance of the six outcome combinations before and after vaccination (Table 2). However, the costs per instance of the outcome combinations that involved hospitalization were significantly higher (P<0.001).
Group Pre-vaccination Post-vaccination AECOPD Pneumonia AECOPD& pneumonia AECOPD& Hospitalization Pneumonia& hospitalization AECOPD& pneumonia& hospitalization AECOPD AECOPD& pneumonia AECOPD& hospitalization Pneumonia& hospitalization AECOPD& pneumonia& hospitalization TIV group 701.1 – 1,069.1 13,146.5 5,433.3 9,549.7 – 1,566.7 10,903.1 18,617.2 11,633.2 PPSV23 group 1,103.6 – 1,363.9 6,667.4* – 8,449.1 722.2 2,500.0 11,147.6* – 10,102.1 TIV&PPSV23 group 649.3 1,231.3 805.5 8,810.2 9,140.6 8,134.6 1,057.4 1,343.3 11,877.6 14,276.4 12,777.0 Unvaccinated group 550.5 2,000.0 1,276.9 12,509.2† 7,510.0 10,591.5§ 716.0 1,000.0 15,098.8† – 13,962.0§ Total 751.4 1,423.5 986.0 9,852.1 7,908.8 8,814.9¶ 922.7 1,550.7 12,337.4 16,446.8 12,349.5¶ Note: “–” means no outcome was reported.
Abbreviation: TIV=trivalent influenza vaccine; PPSV23=23-valent pneumococcal polysaccharide vaccine; AECOPD=acute exacerbation of chronic obstructive pulmonary disease.
* P=0.01;
† P=0.004;
§ P<0.001;
¶ P=0.04.Table 2. Cost (in CNY) per instance of different outcomes, pre-vaccination, and post-vaccination.
The average costs per person before and after vaccination were analyzed across four groups: TIV, PPSV23, TIV&PPSV23, and unvaccinated. In the TIV group, the average costs per person before and after vaccination were 4,115.2 CNY and 1,932.5 CNY respectively. In the PPSV23 group, the average costs per person before and after vaccination were 4,330.8 CNY and 3,440.1 CNY respectively. For the TIV&PPSV23 group, the average costs per person before and after vaccination were 4,032.0 CNY and 2,114.5 CNY respectively, while for the unvaccinated group, the average costs per person before and after vaccination were 1,696.7 CNY and 1,422.1 CNY respectively. For the TIV group and TIV&PPSV23 group, costs per person after vaccination were significantly lower than before vaccination (P=0.04, P<0.001). However, for the PPSV23 and unvaccinated groups, there were no significant differences observed between year 1 and year 2 (P=0.23, P=0.26), as shown in Table 3. In the TIV&PPSV23 group, the cost savings between different COPD severity levels were statistically different (P=0.008, P>0.005). However, there were no other statistically significant differences observed among different age groups, genders, occupations, COPD severity, comorbidities, and smoking status, in different groups. We observed a trend of lower cost savings with increasing age and COPD severity, and higher cost savings in COPD patients without comorbidities.
variable TIV group PPSV23 group TIV&PPSV23 group Unvaccinated group No. of
casesPre- Post- No. of
casesPre- Post- No. of
casesPre- Post- No. of
casesPre- Post- Age (years) <65 41 4,337.3 509.4 23 3,015.8 2,327.3 125 3,815.9 1,550.8 151 1,402.5 1,103.2 ≥65 68 3,981.2 2,790.6 46 4,988.2 3,996.5 171 4,189.9 2,526.6 137 2,021.1 1,773.6 Gender Male 94 4,668.2 2,148.4 52 5,433.3 4,541.7 226 4,419.3 2,769.5 214 1,992.2 1,724.4 Female 15 649.7 579.8 17 958.2 70.6 70 2,781.6 0.0 74 842.3 547.9 Occupation Coal miner 79 5,532.3 2,666.4 41 6,435.2 4,887.2 230 4,460.6 2,717.3 202 1,873.3 1,818.0 Other 30 383.3 0.0 28 1,249.3 1,321.1 66 2,538.2 13.8 86 1,281.9 492.3 Severity of COPD Mild 12 1,965.5 2,534.1 13 639.5 3,311.2 39 1,073.8 479.2 43 362.6 739.8 Moderate 40 3,817.0 952.4 18 3,083.9 2,469.4 120 4,417.7 1,717.2 105 1,687.0 771.4 Severe 40 4,866.5 2,676.7 21 8,755.9 6,622.5 101 5,075.2 2,200.5 82 1,862.5 2,027.3 Very severe 17 4,566.3 2,063.2 17 3,007.3 635.3 36 3,024.2 4,969.5 58 2,469.2 2,250.3 Comorbidities Yes 76 3,531.7 2,164.7 42 4,512.6 4,005.5 193 3,788.1 2,310.4 134 2,474.4 1,746.0 No 33 5,459.0 1,397.9 27 4,047.9 2,560.6 103 4,489.0 1,747.5 154 1,020.0 1,140.3 Smoking Yes 53 5,353.8 2,081.2 26 4,234.6 2,404.5 100 4,581.2 2,112.0 82 1,791.4 1,096.7 No 56 2,942.9 1,791.8 43 4,388.9 4,066.3 196 3,751.8 2,115.8 206 1,659.1 1,551.7 Total 109 4,115.2 1,932.5 69 4,330.8 3,440.1 296 4,032.0 2,114.5 288 1,696.7 1,422.1 Abbreviation: TIV=trivalent influenza vaccine; PPSV23=23-valent pneumococcal polysaccharide vaccine; AECOPD=acute exacerbation of chronic obstructive pulmonary disease. Table 3. Costs (in CNY) per person of AECOPD, pneumonia, and related hospitalization pre-vaccination and post-vaccination.
-
The prevention of AECOPD in patients with COPD can be facilitated through influenza and pneumococcal vaccination. The World Health Organization (5), the United States Centers for Disease Control and Prevention (CDC) (6-7), and the expert consensus in China (2) all recommend the use of both TIV and PPSV23 in COPD patients. Our study is a prospective, before-and-after vaccination, cohort study which aims to determine the burden of illness and impact of TIV and PPSV23 vaccination in COPD patients. Our study findings demonstrate that the economic burden of AECOPD, pneumonia, hospitalization in COPD patients is high. Costs are highest when hospitalization is necessary. Additionally, the economic burdens of these outcomes were significantly decreased following vaccination. These results support the current recommendations for influenza and pneumococcal polysaccharide vaccination in COPD patients.
Seasonal variations in the exacerbation of COPD, pneumonia, and hospitalizations were observed among COPD patients, with the highest occurrences in winter and the lowest in summer and autumn. The most significant reductions associated with vaccination were observed during the winter season. These results corroborate a previous study conducted by Wang et al. (3), which identified a higher incidence of AECOPD during winter, attributed to an increased prevalence of respiratory viral infections associated with colder outdoor temperatures.
Hospitalization costs accounted for over 80% of all outcome costs, which is consistent with the findings of a previous economic study on COPD conducted in India (8). Our study revealed a higher proportion of costs due to work-loss (over 8%) compared to the Indian study (4%). The average cost of outpatient visits in our cohort was approximately 1,000 CNY, while the average cost of hospitalization was approximately 10,000 CNY. Interestingly, the costs per hospitalization in our study were lower than those observed in two studies conducted in Beijing (9-10), indicating regional variations within China. Additionally, the hospitalization costs we found were lower than those reported in the United States (11) and Canada (12), but higher than those in India (8), Italy (13), Türkiye (14), and Vietnam (15). This comparison suggests that the economic burden caused by AECOPD in China is relatively high. Our study demonstrated that vaccination was associated with the greatest reduction in hospitalization costs due to the decreased number of hospitalizations.
In both the TIV group and the TIV&PPSV23 group, costs decreased significantly following vaccination, providing evidence that vaccination is correlated with a reduction in COPD-related expenses. This outcome aligns with findings from other studies (16–17). Research has identified risk factors for AECOPD, including smoking, the presence of comorbidities, and the severity of COPD (1,3). In our study, we observed an upward trend in costs with increasing COPD severity, while COPD patients without comorbidities exhibited lower costs.
The present study has several strengths. First, we utilized a self-controlled pre-and-post design to estimate the economic burden associated with exacerbation, pneumonia, and related hospitalizations in COPD patients. Second, the comparable epidemic intensity of pre- and post-vaccination influenza (18) made our study design particularly meaningful. Lastly, our study offered cost-savings evaluations for three vaccination groups — an influenza vaccine group, a PPSV23 group, and an influenza&PPSV23 group — within a single study.
That being said, our study also has limitations. One potential issue relates to the accuracy of cost estimates. Although we verified the bulk of costs associated with the project, some expenses were ultimately estimated by study participants; thus the accuracy of these costs may be questionable. Nevertheless, we believe the impact of incomplete estimates will be negligible. Additionally, it is worth noting that COVID-19 interventions since February 2020 may impact the effect of vaccination. However, since AECOPD, pneumonia, and hospitalizations occur most frequently in the winter, the influence of COVID-19 interventions may be limited. Lastly, the small size of the PPSV23 group and sub-groups in all groups precluded accurate estimates for desirable comparisons — such as the vaccination impact by COPD severity.
In conclusion, the economic burden of AECOPD, pneumonia, and hospitalization related to COPD in patients residing in China is substantial. Immunization with influenza vaccine and PPSV23, either individually or in combination, can yield substantial reductions in costs, thereby lending support to extant vaccination guidance for patients with COPD.
-
No conflicts of interest reported.
-
Jianquan Li, Xiaohui Zhang, Yi Wang, Yanru Zhang, Yadi Su, Xueying Li, and other colleagues from ten hospitals participating in this study; Lance Rodewald from China CDC.
HTML
| Citation: |

|