
 Download:
Download:




-
Pertussis, a highly contagious acute respiratory disease caused by Bordetella pertussis bacteria, has been a significant contributor to morbidity and mortality in infants and young children (1). The average incubation period spans 7 to 10 days, with a range of 2 to 21 days (2). Since the initiation of China’s national immunization program in 1978, pertussis has been effectively controlled through the widespread use of the diphtheria, tetanus, and whole-cell pertussis vaccine (DTwP). From 2007 to 2013, DTwP was gradually replaced by the co-purified diphtheria, tetanus, and acellular pertussis vaccine (DTaP).
There are three primary types of pertussis vaccines utilized worldwide: whole-cell, component purified acellular, and co-purified acellular vaccines (
Supplementary Materials ). In countries with high DTaP vaccination rates, such as the United States and Australia, the incidence of pertussis has increased following years of low incidence — a phenomenon referred to as the “pertussis resurgence” (1). In China, the reported coverage for three doses of the pertussis vaccine has been maintained at over 99% in recent years (3), yet the incidence of pertussis has also risen, with the majority of cases occurring among infants (4). This increase followed the transition from DTwP to co-purified DTaP, and since few countries employ the co-purified DTaP, it is of critical importance to evaluate the vaccine effectiveness (VE) of co-purified DTaP on a dose-by-dose basis. Since 2016, Linyi Prefecture in Shandong Province has conducted enhanced pertussis surveillance, revealing that the number of reported cases rose from 96 in 2016 to 688 in 2018.In this study, a retrospective cohort design was employed to assess the absolute VEs of each of the four recommended doses of co-purified DTaP in preventing pertussis-related illnesses and hospitalizations. The aim was to provide empirical support for optimizing pertussis immunization strategies.
The study was conducted in Linyi Prefecture, the largest city in Shandong Province, China, encompassing a population of 10 million residents spread over 17,000 square kilometers. The pertussis vaccination schedule in Linyi aligns with that of Chinese mainland, consisting of four 0.5 mL doses of co-purified DTaP administered at 3 months, 4 months, 5 months, and 18 months of age.
The study population consisted of children born between January 1, 2017, and December 31, 2017, who were permanent residents in Linyi Prefecture and had records in Shandong’s Immunization Information System. Exclusion criteria included children who received vaccinations outside of Linyi Prefecture, those vaccinated with co-purified DTaP-Hib or component purified DTaP-IPV/Hib, individuals missing gender information, those with a history of pertussis vaccination prior to 3 months of age, or those diagnosed with pertussis before 3.5 months of age.
Data on vaccination and key demographic information were obtained from the China Immunization Information System. Pertussis diagnoses were gathered from the National Notifiable Diseases Reporting System (NNDRS), the Hospital Management Information System (HIS), and telephone surveys. Pertussis cases were either clinically diagnosed or laboratory-confirmed.
The definitions, such as cases, cumulative vaccination rates, timely vaccination rates, n-group, and VE, can be found in the Supplementary Materials. The cohort was divided into 0-, 1-, 2-, 3-, and 4-dose groups based on the number of doses received and infection status by 24 months of age (
Supplementary Figure S1 ). VE was estimated using the hazard ratio (HR).Descriptive statistics were utilized to summarize cumulative vaccination rates, and timely vaccination rates. HRs and their 95% confidence intervals (CIs) for doses 1, 2, 3, and 4 were obtained using multivariate Cox regression models. HRs were employed to calculate VE and its associated 95% CIs. Data analyses were conducted using Excel software (version Home and Student 2019, Microsoft Office, USA) and SAS software (version 9.4, SAS Institute Inc., Cary, NC, USA).
The cohort included 194,981 individuals (
Supplementary Figure S2 ). 104,210 (53.45%) were male and 90,771 (46.55%) were female; 77,112 (39.55%) lived in urban areas and 117,869 (60.45%) lived in rural areas (Table 1). Figure 1 displays the cumulative vaccination rate for each dose of co-purified DTaP by age in days. The cumulative vaccination rates for 1–4 doses of co-purified DTaP by age 2 years were 92.30%, 90.73%, 88.89%, and 73.34%, respectively, while timely vaccination rates with a one-month grace period were 69.77%, 52.36%, 39.27%, and 27.30%. Details on vaccination ages and intervals for 1–4 doses of co-purified DTaP can be found inSupplementary Table S1 andSupplementary Figure S3 .Characteristics All participants N (%) Pertussis cases N (%) Pertussishospitalization N (%) 0-dose group N (%) 1-dose group N (%) 2-dose group N (%) 3-dose group N (%) 4-dose group N (%) Gender Male 104,210 (53.45) 134 (0.13) 91 (0.09) 104,210 (100) 95,854 (91.98) 94,018 (90.22) 91,846 (88.14) 73,368 (70.40) Female 90,771 (46.55) 132 (0.15) 89 (0.10) 90,771 (100) 84,002 (92.54) 82,640 (91.04) 81,049 (89.29) 65,884 (72.58) Living place Urban 77,112 (39.55) 88 (0.11) 59 (0.08) 77,112 (100) 69,584 (90.24) 67,994 (88.18) 66,238 (85.90) 51,304 (66.53) Rural 117,869 (60.45) 178 (0.15) 121 (0.10) 117,869 (100) 110,272 (93.55) 108,664 (92.19) 106,657 (90.49) 87,948 (74.62) Total 194,981 (100) 266 (0.14) 180 (0.09) 194,981 (100) 179,856 (92.24) 176,658 (90.60) 172,895 (88.67) 139,252 (71.42) Table 1. Demographic characteristics of the study cohort.
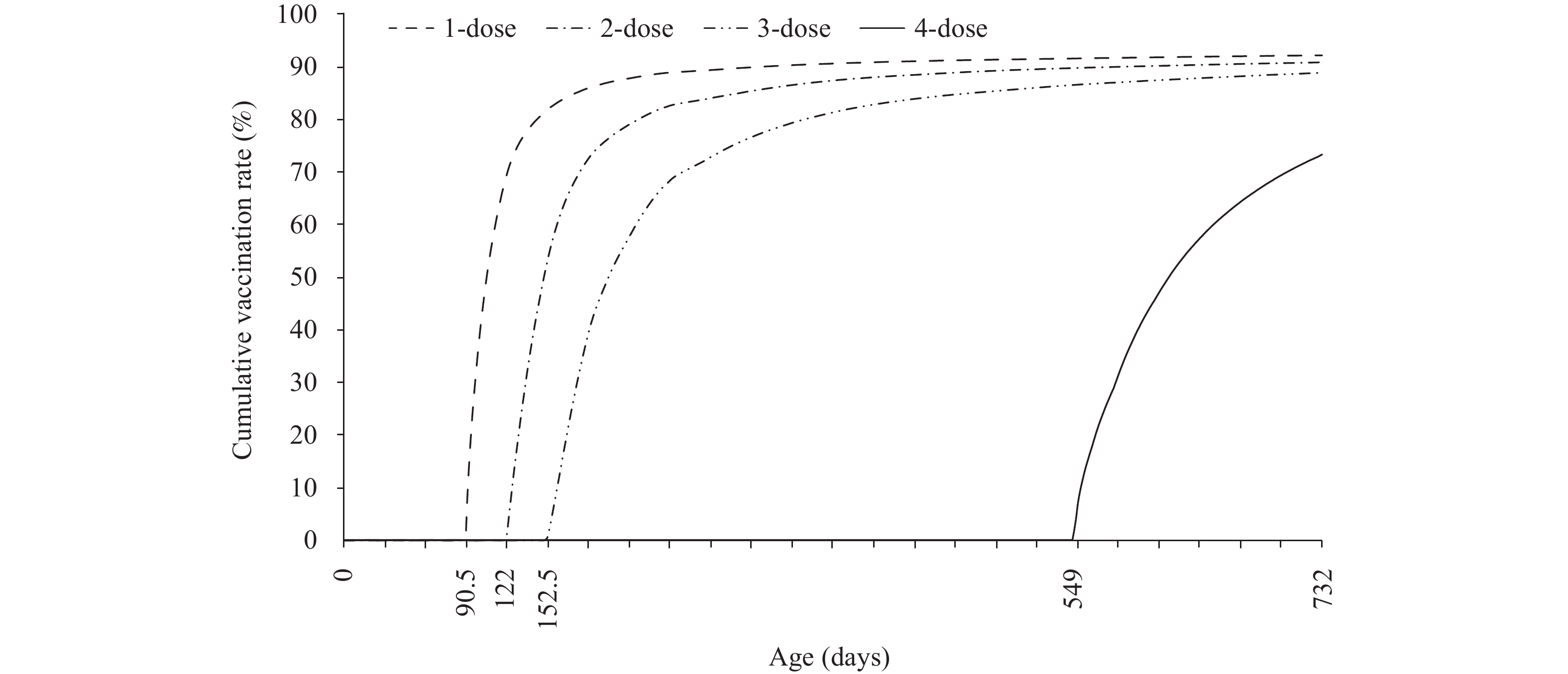 Figure 1.
Figure 1.Cumulative vaccination rates for each dose of the co-purified diphtheria, tetanus, and acellular pertussis vaccine (DTaP) by age in days.
Participants were categorized into non-mutually exclusive 0-, 1-, 2-, 3-, and 4-dose groups as follows: 194,981 individuals (100%) were in the 0-dose group, 179,856 (92.24%) in the 1-dose group, 176,658 (90.60%) in the 2-dose group, 172,895 (88.67%) in the 3-dose group, and 139,252 (71.42%) in the 4-dose group.
In the study cohort, 266 individuals (0.14%) were diagnosed with pertussis between the ages of 3.5 months and 2 years, including 135 clinically diagnosed cases and 131 laboratory-confirmed cases. Among the pertussis cases, 180 were hospitalized (comprising 113 clinically diagnosed cases and 67 confirmed cases). Three of the hospitalized individuals were admitted to an intensive care unit (ICU), including one clinically diagnosed case and two confirmed cases (Table 1).
After adjusting for gender and urban/rural residency, the adjusted VEs of 1–4 doses in the prevention of pertussis-related diseases were as follows: 24.1% (95% CI: −18.3, 51.3), 45.5% (95% CI: 14.4, 65.3), 57.9% (95% CI: 41.4, 69.7), and 87.1% (95% CI: 75.0, 93.4). Additionally, the adjusted VEs against pertussis-related hospitalization were 25.6% (95% CI: −27.2, 56.5), 63.2% (95% CI: 31.5, 80.2), 60.3% (95% CI: 41.7, 73.0), and 86.6% (95% CI: 69.7, 94.1). Due to the limited number of patients admitted to an ICU (3 cases), a reliable estimate of VE against ICU admission could not be calculated (Table 2).
Immunizationgroup Median observation time, person-days Total observation time, person-days Pertussis onset Pertussis-related hospitalization Casenumber Incidence density, 100,000 person-days Unadjusted VE, % (95% CI) Adjusted VE, % (95% CI)* Casenumber Incidence density, 100,000 person-days Unadjusted VE, % (95% CI) Adjusted VE, % (95% CI)* 0 15.5 15,138,796.5 56 0.370 ref. ref. 42 0.277 ref. ref. 1 36 10,463,060.0 38 0.363 23.4 (−19.4, 50.8) 24.1 (−18.3, 51.3) 25 0.239 24.4 (−29.3, 55.8) 25.6 (−27.2, 56.5) 2 38 11,462,479.0 33 0.288 44.8 (13.3, 64.9) 45.5 (14.4, 65.3) 15 0.131 62.7 (30.7, 79.9) 63.2 (31.5, 80.2) 3 399 68,429,951.0 127 0.186 55.4 (38.1, 67.9) 57.9 (41.4, 69.7) 90 0.132 58.3 (38.8, 71.5) 60.3 (41.7, 73.0) 4 131 16,553,757.0 12 0.072 86.4 (73.7, 93.0) 87.1 (75.0, 93.4) 8 0.006 85.7 (67.7, 93.6) 86.6 (69.7, 94.1) Abbreviation: VE=vaccine effectiveness; DTaP=diphtheria, tetanus, and acellular pertussis vaccine; CI=confidence interval; ref.=reference.* Adjusted for sex, urban/rural status. Table 2. VE of 1–4 doses of co-purified DTaP.
-
Our study revealed that the co-purified DTaP manufactured in China demonstrated considerable effectiveness against pertussis disease and associated hospitalizations in children aged 2 years and below. Furthermore, the effectiveness increased progressively with each subsequent dose. When adjusted for gender and urban/rural status, the absolute VEs for the prevention of pertussis-related disease were found to be 24.1%, 45.5%, 57.9%, and 87.1% for the first through the fourth doses, respectively. Corresponding effectiveness levels against pertussis-related hospitalization were 25.6%, 63.2%, 60.3%, and 86.6%, respectively.
Our VE findings align with those reported in previous DTaP VE investigations. Two case-control studies, matching participants based on residence and sex, were conducted in Guangdong Province. One study in Zhongshan City demonstrated VE against pertussis in children aged 4–11 months to be 42%, 88%, and 95% for one, two, and three doses of co-purified DTaP, respectively (5). Another study in Shenzhen found VE against pertussis-related illness among children aged 4 months to 6 years to be 82% for one or two doses, 87% for three doses, and 91% for four doses of DTaP, analyzing co-purified DTaP, co-purified DTaP-Hib, and component purified DTaP-IPV/Hib together (6). Both studies classified infants vaccinated within 21 days of illness onset as unvaccinated, potentially leading to an overestimation of VE.
A systematic review estimated acellular pertussis VEs for pertussis diagnosis and hospitalization to be 82% and 91%, respectively (7). A retrospective case series in Singapore reported the VE of acellular pertussis vaccines (component purified DTaP-IPV/Hib and DTaP-HBV-IPV/Hib) against intensive care unit or high-dependency admission to be 87% among children with a median age of 2.75 months (8). A case-cohort study in Switzerland indicated that, among children under 2 years old, VE of one to four doses of component purified DTaP against pertussis hospitalization was 42%, 84%, 98%, and 100% (9).
In the present study, VE against pertussis incidence and hospitalization revealed a significantly higher VE following a booster dose when compared to the outcome after the primary three-dose series. VE estimates may vary due to factors such as the definition of pertussis infection timing, study design, vaccine type, and immunization schedule. Although direct comparison of study results is not feasible, VE investigations generally indicate enhanced protection after the fourth dose of DTaP, suggesting that timely and complete vaccination with DTaP can effectively minimize the risk of pertussis-related illness and hospitalization.
A strength of our study design lies in the ability to estimate dose-by-dose VE through the calculation of HRs using Cox regression model, even in the context of high vaccine coverage. Cohort members were categorized into five non-mutually exclusive groups (0–4 dose groups) based on the time each dose was deemed effective and the time of pertussis infection, and then we obtained VE for doses 1, 2, 3, and 4. A similar method was utilized in a study conducted in Switzerland using a case-cohort design, yielding positive results (9). We believe our approach allows immunization programs to accurately evaluate dose-by-dose VE in the context of high vaccination coverage.
Additionally, the large cohort size of nearly 200,000 young children provided sufficient power to construct a robust Cox regression model for estimating VE against two outcomes: pertussis disease and pertussis hospitalization.
The study design facilitated the determination of cumulative vaccination rates, revealing that the coverage levels for 1–4 doses among children aged ≤2 years in Linyi Prefecture were 92.30%, 90.73%, 88.89%, and 73.34%, respectively. The cumulative 3-dose coverage rate was marginally higher than the global rate estimated by WHO (86%) but marginally lower than the 90% target value proposed in 2015 (10). Cumulative 4-dose coverage, however, remained relatively low. This discrepancy could be attributed to the inclusion of doses administered only before the second birthday, excluding those given to older children. Timely vaccination rates (allowing for a one-month grace period) for all four doses were low, with respective values of 69.77%, 52.36%, 39.27%, and 27.30%. It is crucial to emphasize the role and importance of DTaP, regularly review missed vaccinations, and implement catch-up vaccinations to enhance timely and comprehensive vaccination coverage among age-eligible children.
In China, the existing co-purified DTaP vaccination schedule commences at three months of age. However, the current WHO position paper suggests that the initial dose could be administered as early as six weeks and should be administered no later than eight weeks of age (11). Consequently, it is important to investigate the potential benefits of introducing pertussis vaccination at an earlier age in China.
Our study presents several limitations. While we took into account the effects of gender and urban/rural status on VE, other confounding variables, such as pre-existing medical conditions, might also impact VE. Moreover, due to the heightened sensitivity of pertussis surveillance in China for children under 2 years of age, our VE assessments were confined to this particular age group.
In children under 2 years of age, the overall VE against pertussis disease or hospitalization demonstrated an increase with a higher number of administered co-purified DTaP doses; four doses providing substantial protection. We recommend reinforcing the importance of timely and complete DTaP vaccination for age-appropriate children and investigating the possibility of administering the first dose at 2 months of age to minimize the risk of pertussis disease and hospitalization in infants.
-
No conflicts of interest.
-
Linyi Center for Disease Control and Prevention and Jinan Center for Disease Control and Prevention.
HTML
| Citation: |

|