
 Download:
Download:




-
Since December 2022, a significant coronavirus disease 2019 (COVID-19) epidemic has emerged in China following the easing of prevention and control measures. The objective of the current study was to characterize the epidemic curve and investigate the vaccine effectiveness (VE) against the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) Omicron variant infection and associated symptoms during this epidemic in China. A total of 4 online surveys were conducted across 31 provincial-level administrative divisions (PLADs) in China to collect data on vaccination and infection status and to delineate the epidemic curve. Furthermore, a test-negative case-control study was carried out to examine the effectiveness of COVID-19 vaccines. The findings of our study revealed that the self-reported infection rate reached its peak between December 19 and 21, 2022, with 82.4% of the Chinese population being infected as of February 7, 2023. The booster vaccination demonstrated effectiveness against infection and symptoms within six months, albeit VE declined over time. These results underscore the importance of developing and producing efficacious vaccines and promoting timely or emergency vaccinations among eligible populations.
In the context of high vaccination coverage in China (91.5% and 89.3% of people received partial and full vaccination, respectively), along with the relatively weak virulence of the SARS-CoV-2 Omicron variant (comprising 99.8%, 99.7%, and 99.3% of analyzed sequences in China, the United States, and the United Kingdom, respectively; sourced from:
https://ourworldindata.org/coronavirus ), the Chinese government relaxed COVID-19 prevention and control measures in December 2022 (1). However, a significant surge in cases occurred between December 2022 and January 2023, as reported by the China CDC (2). Due to the relaxation of control measures, many infected individuals may not have undergone nucleic acid or antigen testing, potentially resulting in an imprecise representation of the epidemic’s magnitude in the China CDC data. In this situation, online surveys may serve as a rapid surveillance tool for assessing the epidemic status. Moreover, this sizable epidemic presented an opportunity to evaluate the real-world effectiveness of domestic vaccines in China (3).Although previous research has demonstrated the effectiveness of vaccines against overall symptoms (the occurrence of any COVID-19-related symptoms) rather than specific COVID-19 symptoms (e.g., sore throat, cough, fever, etc.), more detailed symptomatology information could prove valuable for future vaccine research (3–4). To address these knowledge gaps, the present study conducted multiple online surveys from December 2022 to February 2023, aiming to describe the large-scale epidemic and explore VE in relation to the SARS-CoV-2 Omicron variant’s infection and associated symptoms.
From December 2022 to February 2023, a four-wave online survey was conducted across 31 PLADs in China. Using an anonymous questionnaire provided by “Wen Juan Xing (www.wjx.cn)”, data was collected on participants’ gender, age, address, occupation, vaccination status, vaccine type, time since last vaccination, infection status (symptoms, diagnosis date, and diagnosis method), and the number of infected cohabitants. The characteristics of participants are presented in
Supplementary Table S1 .In this study, the data from the fourth wave online survey of individuals with confirmed infection dates were utilized to estimate the epidemic curve and cumulative infection rate. A test-negative case-control study was employed to investigate the efficacy of COVID-19 vaccines in preventing SARS-CoV-2 Omicron variant infections and associated symptoms. A total of 4,688 individuals with confirmed infections were included, with an equal number of uninfected participants selected as controls from the four-wave online surveys (
Supplementary Figure S1 ).In this study, vaccine effectiveness against COVID-19 infection was evaluated, considering that some participants exhibited COVID-19 related symptoms but did not undergo nucleic acid or antigen tests. We categorized cases into three types: 1) those identified by positive nucleic acid tests; 2) those identified by positive antigen tests; and 3) those identified by self-reported COVID-19 related symptoms. To control for confounding factors, such as sex and age, these cases were matched 1∶1 using a propensity score approach (5).
A caliper of 0.2 standard deviation (SD, with a specific value of 0.002) was implemented for the distance of all participants to prevent far matching. Cases without controls within the 0.2 SD distance were discarded. To estimate vaccine effectiveness against COVID-19 related symptoms, individuals reporting specific symptoms were defined as cases, and they were also matched 1∶1 using the propensity score approach.
Vaccination status was categorized based on the number of vaccination doses received (unvaccinated, partially vaccinated, fully vaccinated, or boosted), booster vaccination status, the time elapsed since the last vaccination and subsequent infection (<3 months, 3–6 months, >6 months), and the type of booster vaccine administered (inactivated, adenovirus vector, or recombinant protein vaccine). Unvaccinated individuals were those who had not received any COVID-19 vaccinations; partially vaccinated individuals had received only the first dose of an inactivated vaccine; fully vaccinated individuals had received two doses of an inactivated vaccine; and those with a booster vaccination had received two doses of inactivated vaccine plus one booster dose of either an inactivated, adenovirus vector, or recombinant protein vaccine.
The daily self-reported infection rate, derived from the online survey, was calculated by dividing the number of new cases by the total number of survey participants. Similarly, the cumulative self-reported infection rate was determined by dividing the number of cumulative cases by the total number of survey participants. A conditional logistic regression was employed to assess the odds ratio of vaccination between cases and controls. Subsequently, the vaccine effectiveness and corresponding 95% confidence interval (CI) were estimated utilizing the given formula:
$$ \begin{aligned} {\rm{VE}} = & \;(1 - {\rm{odds}}\; {\rm{ratio}}\; {\rm{of}}\; {\rm{vaccination}}\; {\rm{in}}\; {\rm{cases}}\;\\ &{\rm{compared}}\; {\rm{to}}\; {\rm{controls}}) \times 100\%. \end{aligned} $$ (1) The primary focus of this study was to investigate the effectiveness of the booster vaccination. Subgroup analyses were conducted based on age (≤18, 19–59, and ≥60 years) and sex to provide additional insights into specific population groups.
All P-values were evaluated using a two-sided test, with a significance level of α=0.05 to indicate the presence of a Type I error. Statistical analyses were conducted using R software (version 4.0.5; R Foundation for Statistical Computing, Vienna, Austria).
The epidemic curve was constructed using data from 2,391 participants in the fourth online survey, in which 82.4% reported being infected as of February 7, 2023. The self-reported infection rate began to rise in early December 2022, reaching a peak between December 19 and 21, 2022 (15.5%), before declining to 0.1% during February 2 to 4, 2023 (Figure 1). The epidemic curves by gender and age were generally consistent with the pattern observed in the total population (
Supplementary Figure S2 ).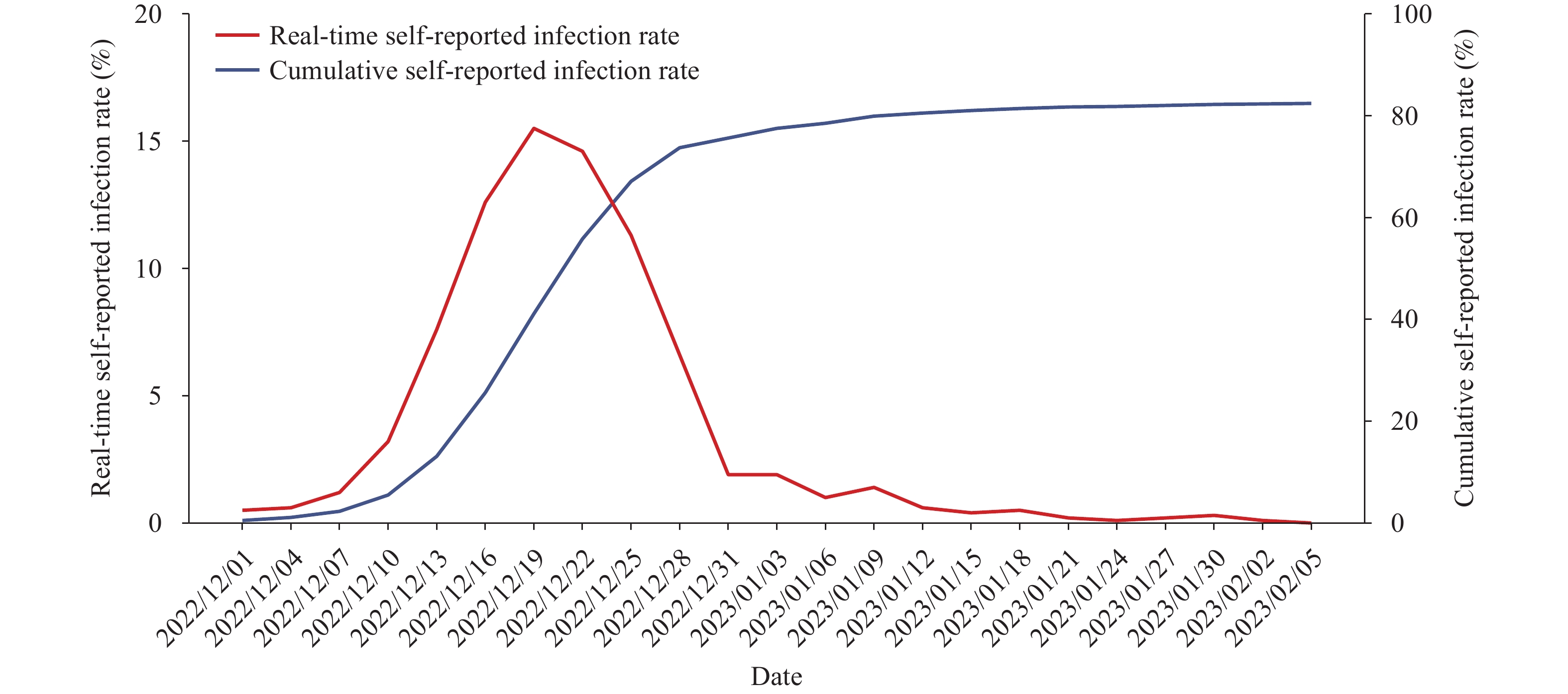 Figure 1.
Figure 1.Real-time and cumulative self-reported infection rates of COVID-19 in China based on an online survey conducted between December 1, 2022 and February 7, 2023.
Abbreviation: COVID-19=coronavirus disease 2019.A total of 4,688 participants were infected with SARS-CoV-2. Among them, 3.5% were unvaccinated, while 1.7%, 14.9%, and 79.9% had received partial, full, and booster vaccinations, respectively (
Supplementary Table S2 ). In the matched control group of 4,688 uninfected participants, the proportions of unvaccinated, partially vaccinated, fully vaccinated, and booster-vaccinated individuals were 3.1%, 1.3%, 12.8%, and 82.8%, respectively. No significant VE against infection was observed for full or booster vaccinations beyond 6 months post-vaccination. However, within 3 months of receiving a booster vaccination, significant protection against infection was observed (VE: 49.0%; 95% CI: 27.1%–64.3%), as well as between 3–6 months (VE: 37.9%; 95% CI: 13.7%–55.4%). Similar results were observed for various case definitions and different vaccines (Figure 2,Supplementary Figure S3 ). Notably, the VE of the booster vaccination was lower among individuals aged >60 years (Supplementary Table S3 ).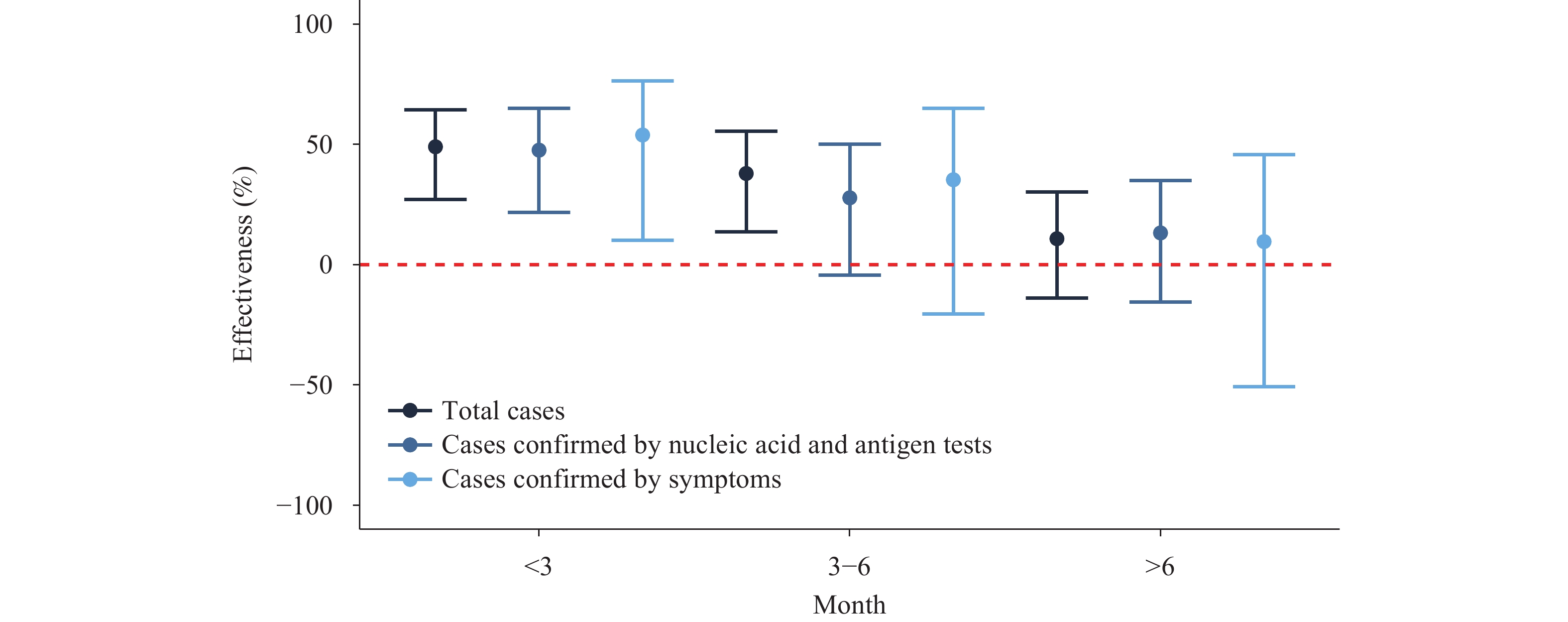 Figure 2.
Figure 2.Effectiveness of booster vaccination against SARS-CoV-2 infection, categorized by time period following vaccination.
Abbreviation: SARS-CoV-2=severe acute respiratory syndrome coronavirus 2.The booster vaccination demonstrated effectiveness against various COVID-19 symptoms, including fever, nasal obstruction, rhinorrhea, sore throat, cough, expectoration, headache, muscle soreness, anorexia, fatigue, and hypogeusia within six months after administration. However, VEs were not statistically significant beyond six months post-booster vaccination. Within three and six months following the booster vaccination, VEs ranged from 48.7% to 83.2% and 25.9% to 69.0%, respectively (Figure 3)
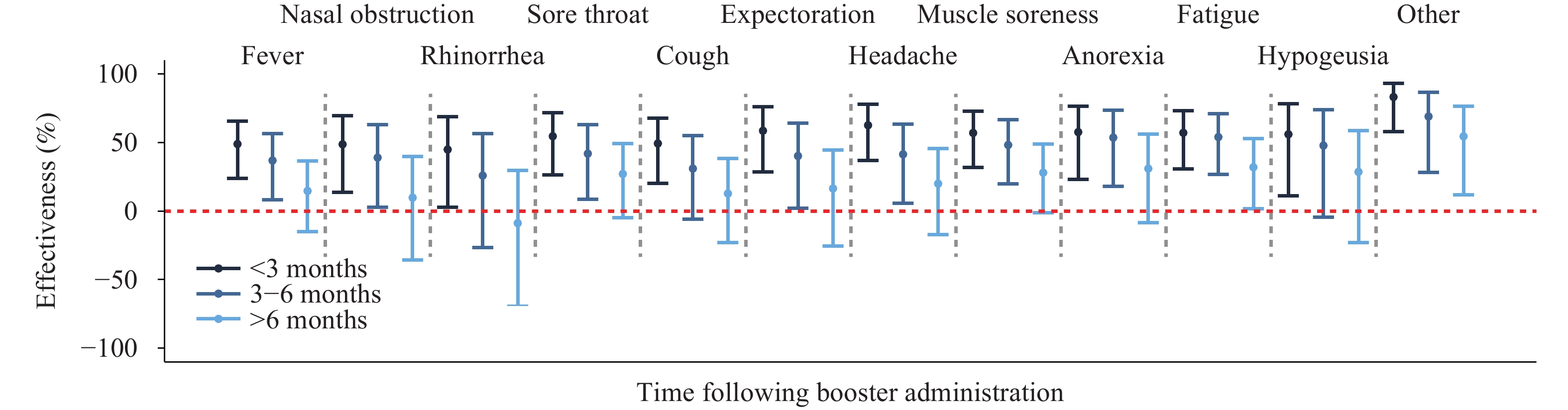 Figure 3.
Figure 3.Effectiveness of COVID-19 vaccination in reducing related symptoms over time (months) following booster administration.
Abbreviation: COVID-19=coronavirus disease 2019. -
In December 2022, a significant COVID-19 outbreak occurred in China, with over 82% of the population being infected within a two-month period. Accurately monitoring the daily number of infections during such a large-scale outbreak within a short timeframe has proven to be challenging for health departments because mass nucleic acid testing was discontinued in China after December 2022. Health authorities consequently relied on the positive rate of nucleic acid and antigen tests from fever clinics to dynamically monitor the epidemic (2).
Nonetheless, since most infected individuals did not undergo nucleic acid and antigen testing after December 2022, and only a select few symptomatic or suspected individuals visiting fever clinics received these tests, the positive rate from fever clinics could overestimate the epidemic’s scale. Consequently, online surveys have emerged as a rapid approach to monitoring the epidemic. A study utilizing an online survey of teachers and students in public health schools across China found that the epidemic peaked between December 17 and 22, 2022, in most PLADs (6). Our findings align with those of national community-based surveillance, which also indicated a peak between December 20 and 22 (7).
A series of studies have documented the efficacy of inactivated vaccines used in China (3,8). However, these investigations were conducted within clinical trials or limited regional outbreaks during the “dynamic zero” policy, thus not providing real-world evidence. According to our findings, booster vaccinations demonstrated effectiveness against infection within a six-month period, and the VE diminished over time. These results align with previous studies conducted in China and Brazil (3,9). Furthermore, a recent meta-analysis that reviewed 27 randomized controlled trials confirmed significant effectiveness against symptomatic infection and the waning of VE over time (10). Nevertheless, few studies have investigated VE against specific symptoms within a real-world context in China. Our study reveals that booster vaccinations can effectively protect against COVID-19 symptoms such as fever, nasal congestion, and runny nose.
This study had several limitations. First, the online survey utilized a convenience sample conducted through WeChat. Second, the epidemic curve was constructed using data from only 2,316 participants with a specific infection date. Third, study participants were not evenly distributed throughout China. Finally, the infection history of participants was not collected, which may introduce bias. Fourth, when exploring the VE against specific symptoms, the limited sample size may lead to relatively large confidence intervals, and further study with larger sample is necessary in the future.
In conclusion, China faced a significant COVID-19 epidemic, resulting in over 82% of individuals becoming infected between December 2022 and February 2023. Throughout this epidemic, booster vaccinations administered within a six-month period demonstrated effectiveness in preventing infection and mitigating COVID-19 symptoms. The findings of this study may contribute valuable insights to inform the development of future COVID-19 vaccination strategies.
HTML

| Citation: |

|