

 Download:
Download:




-
Tuberculosis (TB) is a multisystem disease that could affect any organ (1-2). Extrapulmonary tuberculosis (EPTB) cases account for 13.37% to 53.00% of TB cases globally, which were 11.93% to 33.40% of cases found in China (3). The National TB Program (NTP) sponsored by the State Council of China only covers control and prevention of pulmonary tuberculosis (PTB). The control and prevention status of EPTB remains unclear. It has been found that EPTB has played an important role in achieving the promoted target of End-TB strategy (4). Therefore, it is essential to understand the status of EPTB in China to develop an action plan to address this important issue. A nationwide questionnaire survey to investigate current diagnosis, treatment, and management of EPTB at county level was conducted by China CDC in 2021. It was found that at county level in China, there were no unified diagnostic criteria and methods for EPTB, and patient management was also disparate. Currently, not enough attention has been paid to the control and prevention of EPTB. It is suggested that EPTB be included in NTP.
This study was conducted through questionnaire to investigate the current diagnosis, treatment and management of EPTB nationally in China by China CDC in the first half year of 2021. All Center for Disease Control and Prevention or TB dispensaries at county level were investigated. The professionals responsible for tuberculosis prevention and control work were designated to fill in the questionnaire. Upon completion, the questionnaires were collected and checked by responsible staff of CDCs or TB dispensaries at provincial level. A total of 2,825 questionnaires were distributed with a response rate of 100%. The questionnaire consisted of three parts: basic information of EPTB status, diagnostic capacity for EPTB of the local medical institutions, and opinion on incorporating EPTB into NTP. Data were cleaned in Microsoft Office Excel (version 2019, Microsoft Corp, Washington, USA). The results were summarized with descriptive analysis methods.
As of July 2021, counties in which EPTB was mainly diagnosed by TB designated hospitals accounted for 58.09%, whereas counties in which EPTB was mainly diagnosed by both TB designated hospitals and non-TB designated hospitals accounted for 35.08%; 50.30% of counties adopted individualized treatment regimen for EPTB; 61.77% of counties didn’t enter EPTB’s information in the routine surveillance system at all; the percentage of counties registered all EPTB cases was just 23.36%; 55.54% counties had the same medical insurance policy for EPTB as for other diseases, while 11.58% counties did not include EPTB in basic medical insurance program; 69.95% of counties did not manage EPTB in the same way as they managed PTB, which has been defined by NTP (Table 1).
Question Eastern area
(n, %)Middle area
(n, %)Western area
(n, %)Total
(n, %)Diagnosis Q1: Which is the main hospital for EPTB in your district? TB designated hospital 457 (49.51) 510 (61.67) 674 (62.70) 1,641 (58.09) Non-TB designated hospital 86 (9.32) 44 (5.32) 43 (4.00) 173 (6.12) TB and Non-TB designated hospital 371 (40.20) 271 (32.77) 349 (32.47) 991 (35.08) No response 9 (0.98) 2 (0.24) 9 (0.84) 20 (0.71) Treatment Q2: Which is the main treatment regimen for EPTB in your district? 2HRZE/4HR 72 (7.80) 82 (9.92) 109 (10.14) 263 (9.31) 2HRZE/7-10HRE 337 (36.51) 343 (41.48) 379 (35.26) 1,059 (37.49) Individualized regimen 487 (52.76) 381 (46.07) 553 (51.44) 1,421 (50.30) No response 27 (2.93) 21 (2.54) 34 (3.16) 82 (2.90) Management Q3: Are EPTB cases registered in routine surveillance system in your district? Yes, they are all registered 158 (17.12) 239 (28.90) 263 (24.47) 660 (23.36) Yes, just a part is registered 139 (15.06) 139 (16.81) 121 (11.26) 399 (14.12) No, they aren't 617 (66.85) 444 (53.69) 684 (63.63) 1,745 (61.77) No response 9 (0.98) 5 (0.60) 7 (0.65) 21 (0.74) Q4: What is the medical insurance policy for EPTB in your district? The same as PTB 280 (30.34) 297 (35.91) 307 (28.56) 884 (31.29) The same as other diseases 517 (56.01) 423 (51.15) 629 (58.51) 1,569 (55.54) Wasn't include in basic medical insurance program 109 (11.81) 99 (11.97) 119 (11.07) 327 (11.58) No response 17 (1.84) 8 (0.97) 20 (1.86) 45 (1.59) Q5: Are EPTB cases managed in local TB control program? Yes, the same as PTB 86 (9.32) 136 (16.44) 241 (22.42) 463 (16.39) Yes, but not as strict as PTB 86 (9.32) 149 (18.02) 126 (11.72) 361 (12.78) No, they aren't 738 (79.96) 538 (65.05) 700 (65.12) 1,976 (69.95) No response 13 (1.41) 4 (0.48) 8 (0.74) 25 (0.88) Total 923 (100.00) 827 (100.00) 1,075 (100.00) 2,825 (100.00) Note: The eastern area included the following provincial-level administrative divisions: Beijing, Tianjin, Hebei, Liaoning, Shanghai, Jiangsu, Zhejiang, Fujian, Shandong, Guangdong, and Hainan; the middle area: Shanxi, Jilin, Heilongjiang, Anhui, Jiangxi, Henan, Hubei, and Hunan; and the western area: Inner Mongolia, Guangxi, Chongqing, Sichuan, Guizhou, Yunnan, Xizang (Tibet), Shaanxi, Gansu, Qinghai, Ningxia, and Xinjiang.
Abbreviation: TB=tuberculosis; PTB=pulmonary tuberculosis; EPTB=extrapulmonary tuberculosis.Table 1. Basic information of EPTB in China, 2021.
Approximately 43.68% TB designated hospitals made EPTB diagnosis based on both pathogenesis and histopathology, while 27.86% TB designated hospitals based on pathogenesis or histopathology, and 26.30% based on clinical examination only. As for non-TB designated hospitals, 53.52% of them made EPTB based on clinical examination only, and the percentage of them made EPTB diagnosis based on both pathogenesis and histopathology was 24.25% (Table 2).
Region Only clinical diagnosis Pathogenesis or Histopathology diagnosis Pathogenesis and histopathology diagnosis No response Total Designated hospital
(n, %)Non-designated hospital
(n, %)Designated hospital
(n, %)Non-designated hospital
(n, %)Designated hospital
(n, %)Non-designated hospital
(n, %)Designated hospital
(n, %)Non-designated hospital
(n, %)Designated hospital
(n, %)Non-designated hospital
(n, %)Eastern area 221 (23.94) 407 (44.10) 218 (23.62) 189 (20.48) 458 (49.62) 294 (31.85) 26 (2.82) 33 (3.58) 923 (100.00) 923 (100.00) Middle area 250 (30.23) 455 (55.02) 223 (26.96) 160 (19.35) 337 (40.75) 183 (22.13) 17 (2.06) 29 (3.51) 827 (100.00) 827 (100.00) Western area 272 (25.30) 650 (60.46) 346 (32.19) 165 (15.35) 439 (40.84) 208 (19.35) 18 (1.67) 52 (4.84) 1,075 (100.00) 1,075 (100.00) Total 743 (26.30) 1,512 (53.52) 787 (27.86) 514 (18.19) 1,234 (43.68) 685 (24.25) 61 (2.16) 114 (4.04) 2,825 (100.00) 2,825 (100.00) Note: The eastern area included the following provincial-level administrative divisions: Beijing, Tianjin, Hebei, Liaoning, Shanghai, Jiangsu, Zhejiang, Fujian, Shandong, Guangdong, and Hainan; the middle area: Shanxi, Jilin, Heilongjiang, Anhui, Jiangxi, Henan, Hubei, and Hunan; and the western area: Inner Mongolia, Guangxi, Chongqing, Sichuan, Guizhou, Yunnan, Xizang (Tibet), Shaanxi, Gansu, Qinghai, Ningxia, and Xinjiang.
Abbreviation: EPTB=extrapulmonary tuberculosis.Table 2. Capability of diagnosis on EPTB in different hospitals in China, 2021.
The results of the survey on whether EPTB should be incorporated in NTP management showed that 56.32% of the respondents thought that EPTB should be part of NTP, and only 13.13% of the respondents thought that no attention should be paid to EPTB (Figure 1).
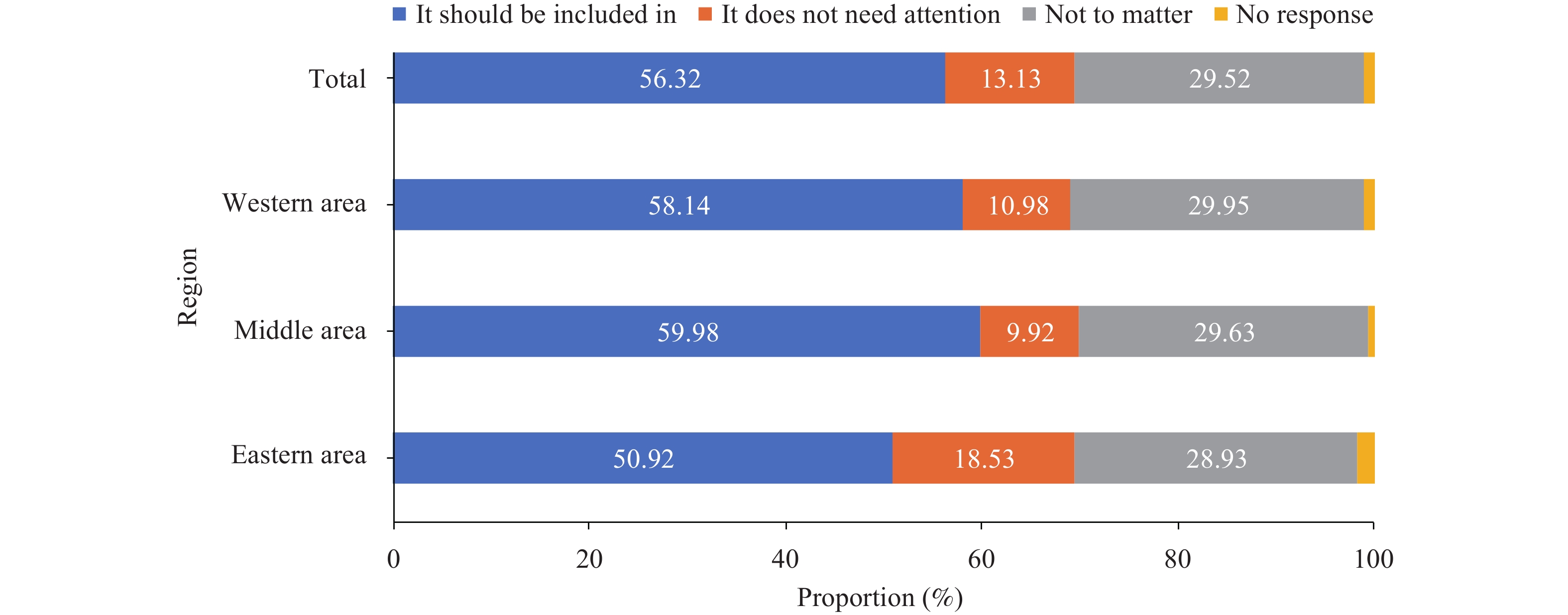 Figure 1.
Figure 1.Results of the survey on whether EPTB should be incorporated in NTP management in China, 2021.
Note: The eastern area included the following provincial-level administrative divisions: Beijing, Tianjin, Hebei, Liaoning, Shanghai, Jiangsu, Zhejiang, Fujian, Shandong, Guangdong, and Hainan; the middle area: Shanxi, Jilin, Heilongjiang, Anhui, Jiangxi, Henan, Hubei, and Hunan; and the western area: Inner Mongolia, Guangxi, Chongqing, Sichuan, Guizhou, Yunnan, Xizang (Tibet), Shaanxi, Gansu, Qinghai, Ningxia, and Xinjiang.
Abbreviation: EPTB=extrapulmonary tuberculosis; NTP=National TB Program.
-
To our best knowledge, this is the first national study to address the status of EPTB diagnosis, treatment and management in China, which offers light for policymakers to develop related strategies for EPTB. The study indicated that there were no specific health facilities responsible for diagnosis, treatment and management of ETPB in China, while more than half of counties thought EPTB should be included into NTP.
There is a lack of standardized diagnosis and management of EPTB throughout the country. Some counties made diagnosis in TB designated hospitals, some in non-TB designated hospitals or TB and non-TB designated hospitals both. The majority of non-TB designated hospitals diagnosed EPTB by only clinical examination, while TB designated hospitals diagnosed EPTB by pathogenesis or histopathology and clinical examination. TB designated hospitals were better than non-TB designated hospitals in diagnostic ability, which was related to the long-term planning of NTP. The NTP required TB designated hospitals to carry out sputum smears, culture and molecular biology examinations for patients, key indicators such as bacteriologically positive rate and treatment success rate had to be a specific level (5-6). On the contrary, non-TB designated hospitals didn’t have the laboratory testing equipment for TB or need to complete the indicators, their diagnostic ability was lower. As a result, EPTB patients cannot be diagnosed accurately, misdiagnoses and missed diagnoses were very likely to occur in non-TB designated hospitals. In addition, not all counties entered EPTB’s information in the routine system and the treatment regimens were different across China, which lead to difficulty to accurately determine the epidemic status of EPTB and evaluate the final outcomes of EPTB patients.
Our study also showed that half of the counties had different medical insurance policy for EPTB, the patients had great economic pressure during the process of seeing a doctor. A cross-sectional study calculated the average total medical expenditure for TB treatment was 12,635.5 CNY (7). EPTB needs longer hospital stays and higher costs than PTB (8), it can be a catastrophic expenditure easily for patients without medical insurance policy.
This study was subjected to some limitations. First, we didn’t survey the epidemic situation of EPTB in China, for example the incidence and mortality of different EPTB, and the policy-makers may not fully understand the importance of EPTB control and prevention. Secondly, our study did not investigate the hospitals and patients linked to EPTB, more targeted policies and practices need to be based on epidemiological and clinical characteristics of patients, costs of medical care, difficulties in seeking medical treatment etc. Therefore, studies based on hospitals and patients should be carried out in the future.
Achieving a TB-free world is a desirable goal with respect to human, animal, and environmental health — according to the tenets of One Health (9). Both PTB or EPTB belong to tuberculosis, ending tuberculosis epidemic needs paying attention to control and prevention of EPTB, this study implied that EPTB should be included in NTP. The governments at all levels need to provide adequate personnel, funding, and policy support for EPTB. TB prevention and treatment organization should establish standards of the diagnosis, treatment and management to EPTB. Whether TB designated hospitals or non-TB designated hospitals need to improve their capacity of recognition and diagnosis to EPTB and enter EPTB information in the routine surveillance system. CDCs and TB dispensaries should actively carry out EPTB screening and strengthen monitoring EPTB in order to grasp the epidemiological trends. Further studies about drugs and treatment regimens for TB are also necessary to do, which will give the patients more effective treatment and reduce their medical burden.
HTML
| Citation: |

|