

 Download:
Download:




-
Three years into the coronavirus disease 2019 (COVID-19) pandemic, several severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variants have emerged with increasing potency in the human population, causing considerable morbidity and mortality worldwide, while Chinese mainland had been able to maintain local containment through an extensive set of targeted non-pharmaceutical interventions (NPIs) (1). Here we developed a fully stochastic, spatially structured, agent-based model of SARS-CoV-2 ancestral strain and reconstructed the Beijing Xinfadi outbreak between June 11 and July 10, 2020. This quantitatively assessed the feasibility and prerequisites for containing the virus before it had the opportunity to acquire its highly transmissivity and immune-evasive properties. We found that screening for symptoms and among high-risk populations served as an aid in uncovering the cryptic community transmission in the early stages of the outbreak. Effective contact tracing greatly reduces transmission. Targeted community lockdowns and temporal mobility restrictions could slow down the spatial spread of the virus. Mass testing could further improve the speed at which the outbreak is contained. Our analysis suggests that the containment of SARS-CoV-2 ancestral strains was certainly feasible. Early in time measures to stop further spread of the outbreak, prevent mutation of the virus into a more deadly variant is cost-effective and can save lives.
The Beijing Xinfadi Wholesale Market outbreak was initially identified on June 11, 2020, shortly after the successful suppression of the initial wave in Wuhan that ended in March 2020 and caused by the ancestral strain of SARS-CoV-2, with the D614G mutation reintroduced from outside China (2). Other details of the outbreak have been previously described (3-5). It is ideal to imitate a generic model of initial containment for countries other than China following the emergence and exportation of SARS-CoV-2 ancestral strain, as few adaptive mutations had been acquired and the herd immunity was negligible (no available vaccine and few prior SARS-CoV-2 infections) during the outbreak. The timing gap between the initial and the Xinfadi Wholesale Market outbreaks also allowed Beijing to expand its SARS-CoV-2 molecular testing capacity (with an initial testing capacity of 100,000 tests per day ramped up to 500,000 tests per day by July 7, 2020), permitting mass testing of the population at risk.
We first analyzed the highly detailed line-list data of the outbreak that had been extracted from the Notifiable Infectious Disease Reporting System and the Epidemiological Investigation Information System of the People’s Republic of China to characterize the epidemiological patterns of the outbreak. We then developed a fully stochastic, spatially structured agent-based model to reconstruct the containment effort and recover the epidemiologic patterns observed in the epidemiological data. The model structure, detailed in the
Supplementary Material andSupplementary Tables S1 –S5 , was well informed by high-resolution population mobility data, allowing us to explicitly model the targeted testing and intervention programme at high spatial resolution. Lastly, we created eight possible intervention scenarios (Levels 1–8, Table 1) by progressively layering additional NPIs on top of the prior scenario, to dissect the relative contribution of each intervention individually to the overall containment of the Xinfadi outbreak.NPI Level 1 Level 2 Level 3 Level 4 Level 5 Level 6 Level 7 Level 8 Symptom surveillance Percentage of detected symptomatic infections (%) 66.7 66.7 66.7 66.7 66.7 66.7 66.7 66.7 Mask wearing Percentage of population wearing masks in the workplace (%) − 20 20 20 20 20 20 20 Percentage of population wearing masks in the community (%) − 50 50 50 50 50 50 50 Closure of the Xinfadi Wholesale Market Date of closure − − 2020-
06-132020-
06-132020-
06-132020-
06-132020-
06-132020-
06-13Quarantine of key population Workers at the Xinfadi Wholesale Market − − − Centralized Centralized Centralized Centralized Centralized Visitors to the Xinfadi Wholesale Market − − − Home Home Home Home Home Residents around the Xinfadi Wholesale Market − − − Lockdown Lockdown Lockdown Lockdown Lockdown Contact tracing Percentage of traced household contact (%) − − − − 100 100 100 100 Percentage of traced work contact (%) − − − − 100 100 100 100 Percentage of traced community contact (%) − − − − 70 70 70 70 Residential community lockdown Duration of lockdown after the identification of the last case (days) − − − − − 14 14 14 Mobility restrictions* Percentage of mobility reductions in high-risk region (%) − − − − − − 70 70 Percentage of mobility reductions in moderate-risk region (%) − − − − − − 50 50 Percentage of mobility reductions in low-risk region (%) − − − − − − 20 20 Mass testing Rounds of RT-PCR testing − − − − − − − 3 Note: “–” means not applicable.
Abbreviation: NPI=non-pharmaceutical intervention; RT-PCR=reverse transcription-polymerase chain reaction.
* The intervention parameters of mobility restrictions are defined as percentages of reductions in population flows between different risk regions during the Xinfadi outbreak, detailed in the Supplementary Table S5 (available in https://weekly.chinacdc.cn/).Table 1. Hypothetical intervention parameters of each NPI in different simulation scenarios.
We ran 500 simulations with each scenario capturing the stochasticity of the transmission process. For each simulation, the following summary statistics were calculated to quantify the impact of each intervention individually: 1) the overall effective reproduction number (
$ {R}_{eff} $ ), defined as the average of the individual reproduction number of each individual infected after the implementation of NPIs; 2) the total number of infections (N) before July 10, 2020 (the end date of the Xinfadi outbreak); and 3) the proportion of undetected infections. The details of each NPI in response to the Xinfadi outbreak were described in the Supplementary Materials. The model was coded in Python (version 3.10.4, Python Software Foundation, Fredericksburg, VA, US). The statistical analyses and visualization were performed using R (version 4.0.2, R Foundation, Vienna, Austria).A total of 368 SARS-CoV-2 infections were reported during the Xinfadi outbreak, including 335 (91.03%) confirmed cases and 33 (8.97%) asymptomatic infections (Figure 1A). Most of the infections were clustered in or around Huaxiang Street, where the Xinfadi Wholesale Market was located (Figure 1B), and were aged between 20 and 59 years (Figure 1C). Simulations closely the imitate real world. We present one realization of the temporal distributions of the reported infections (Figure 1D). Similar to the observed distribution in Figure 1A, a total of 355 infections were detected in the simulated outbreak, of which 18.87% were asymptomatic infections and 81.13% were confirmed cases. Figure 1E–F show the spatial distribution and age profile of the infections aggregating from the results of 500 simulated outbreaks. Both the spatial patterns and age distributions were similar to the real-world observations in Figure 1B–C, with most of the infections detected around the Xinfadi Wholesale Market and in the working age population.
 Figure 1.
Figure 1.Observed and simulated epidemiologic patterns during the Xinfadi outbreak. (A) Observed temporal distribution of SARS-CoV-2 infections stratified by clinical type. (B) Observed spatial distribution of SARS-CoV-2 infections. (C) Observed age distribution of SARS-CoV-2 infections. (D) Time series of SARS-CoV-2 infections stratified by clinical type based on one simulated outbreak. (E) Spatial distribution of SARS-CoV-2 infections estimated based on 500 simulations. (F) Age distribution of SARS-CoV-2 infections estimated based on 500 simulations.
Abbreviation: SARS-CoV-2=severe acute respiratory syndrome coronavirus 2.To quantify the relative contribution of each individual NPI to outbreak containment, we consecutively added each intervention to the unmitigated chains of transmission. The estimated effective reproduction numbers (
$ {R}_{eff} $ ) and total number of infections (N) are reported in Figure 2A and Figure 2B. We found heterogeneity across simulations even under the same intervention intensity, reflecting the intrinsic stochasticity of SARS-CoV-2 transmission. We found that the outbreak could not be contained with only symptom surveillance (Level 1) due to the pre-symptomatic and asymptomatic transmission of SARS-CoV-2, with a median$ {R}_{eff}=2.05 $ and a median N=13,421, respectively. Layering mask wearing (Level 2) and closure of Xinfadi Wholesale Market (Level 3) did not lead to significant improvement, with all simulations having effective reproduction numbers larger than 1.8, well above the epidemic threshold. Quarantine of the key populations (Level 4) could remove the potential infections from the susceptible population at the early phase of viral shedding, thus effectively reducing the number of infections (median N=2,967), but the further transmission could not be suppressed (median${R}_{eff}=1.78$ ). Contact tracing (Level 5), in contrast, could significantly reduce further transmission, leading to fewer infections (median N=1,141) and lower effective reproduction numbers (median$ {R}_{eff}=1.19 $ ), but for most simulations, the estimated$ {R}_{eff} $ was still above the epidemic threshold, indicating that containment could not be achieved through Level 5 intervention intensity. With lockdown of infected individuals’ residential communities (Level 6), the median$ {R}_{eff} $ hovered around the epidemic threshold of 1, resulting in highly stochastic outcomes with the probability of achieving containment at 50%. Implementing targeted population mobility restrictions (Level 7) would achieve the goal of containment, with the estimated$ {R}_{eff} $ ranging from 0.39 to 0.89 and the number of infections less than 1,000 for all simulations. Although the outbreak could be suppressed with Level 7 intervention intensity, additional mass testing at the street/town level was adopted during the Xinfadi outbreak, which could further reduce the effective reproduction number and the number of infections, with a median${R}_{eff}=0.64$ and a median N=447, leading to faster clearance and fewer infections. Furthermore, we found that approximately 10.6% of the infections were undetected in the absence of mass testing (Level 7), while the number of undetected infections fell to 3.6% after the implementation of mass testing (Level 8), indicating that the outbreak could be contained earlier through mass testing, with more infections being detected and isolated, and thus the onward transmission could be truncated (Figure 2C).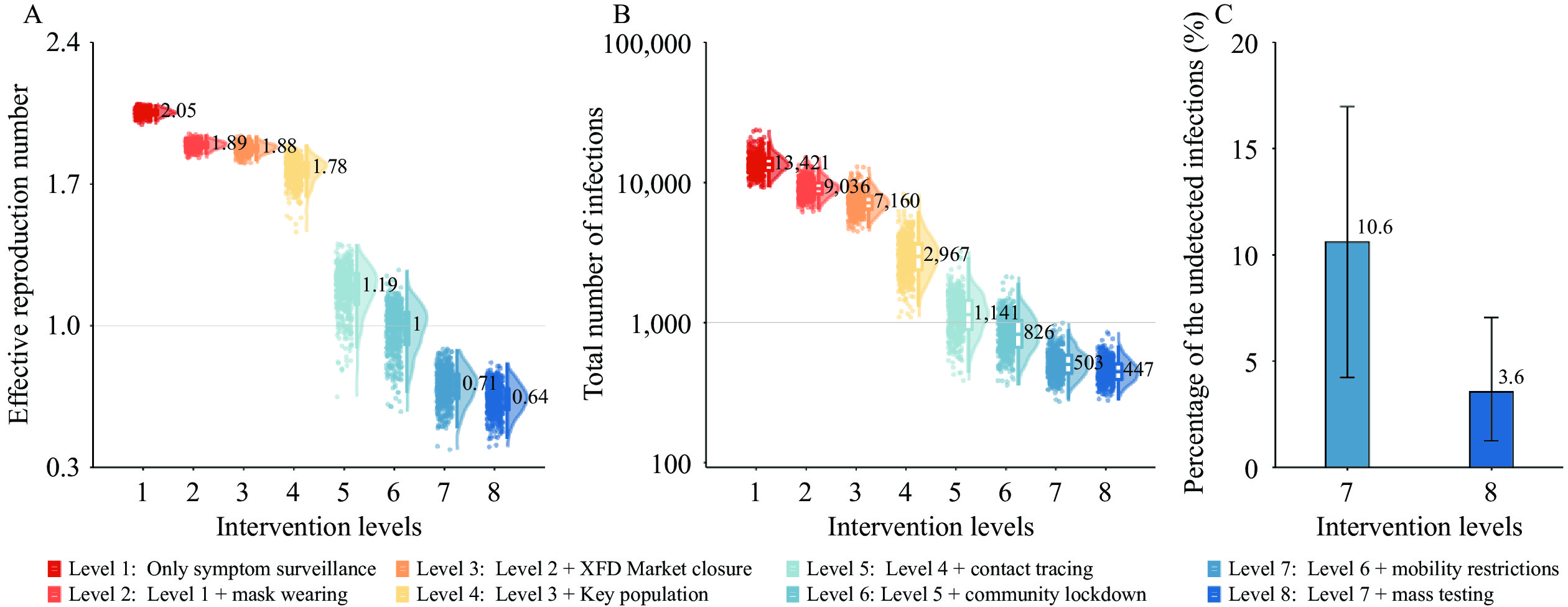 Figure 2.
Figure 2.The impact of each NPI. (A) Effective reproduction numbers under different intervention scenarios. (B) Number of infections under different intervention scenarios. (C) Proportion of undetected infections.
Note: The bars represent the median of 500 simulations, and the lines give the range of the 2.5 and 97.5 quantiles.
Abbreviation: NPI=non-pharmaceutical intervention, XFD Market=Xinfadi Wholesale Market.
-
In this study, we demonstrated through both empirical data and modeling analysis that a multilayer deployment of targeted NPIs could easily contain outbreaks caused by the SARS-CoV-2 ancestral strain. We found that robust implementation of symptom surveillance and high-risk population screening served as sentinels to discover cryptic community transmission in the early stage of the outbreak. Effective contact tracing combined with case isolation and close contact quarantine have been shown to substantially reduce transmission, highlighting the importance of training and maintaining epidemiologic teams with field experience. Targeted community lockdown and rapid turnaround of molecular testing for the confined population could further limit undetected infections missed by contact tracing, as the transmission of SARS-CoV-2 demonstrates clear spatial clustering. It is more cost-effective than population-wide lockdowns, with fewer people being affected. Temporal reductions in mobility (rather than blanket lockdowns) in and out of regions with high infection risk could slow down the spatial dissemination of the outbreak. If conditions permit, population-wide mass testing could further improve the speed of outbreak containment. These evidences carried critical policy implications for the ongoing COVID-19 pandemic and other epidemics caused by newly emerged pathogens.
Currently, the adaptive evolution of SARS-CoV-2 continues with no sign of slowing down, with multiple sublineages of SARS-CoV-2 Omicron emerging continuously and causing recurring Omicron waves despite high levels of population immunity achieved by vaccination and natural infection. In addition, unmitigated spreading could also lead to spillover into other animal reservoirs (6), leaving pathogen eradication impossible to achieve. In contrast, at the beginning of the pandemic, even with negligible population immunity (i.e., no effective vaccine available), due to the limited transmissibility of the ancestral strain (R0=2.5) (7), multiple regions across all socioeconomic statuses successfully achieved temporal suppression of SARS-CoV-2 in the early stage of the pandemic through the implementation of NPIs. In retrospect, had the virus been successfully contained in the early stage of the pandemic, a great deal of the global morbidity, mortality and tremendous socioeconomic costs could have been avoided.
This study was subject to some limitations. First, it suffers from the uncertainty of epidemiological parameters from previous estimates, such as the distribution of the generation interval and the age-specific asymptomatic rates. Second, the temporal span of our simulations is limited. Finally, we cannot simulate all the NPIs during the Xinfadi outbreak, such as the population screening based on the positive environmental samples.
Our study clearly demonstrated that the containment of the SARS-CoV-2 ancestral strain would have been achievable through NPIs once a reliable and scalable diagnostic test became available. More broadly, the critical opportunity window for containing a newly emerged pathogen is in the very early stage of the pandemic, before the pathogen has the opportunity to evolve and adapt in the human population with greatly enhanced transmissibility and immune evasion properties, if all countries decide to pursue such strategies collectively. Furthermore, sustaining SARS-CoV-2 local containment at the early stage of the pandemic could buy some time to achieve high immunization coverage as well as stockpile effective antiviral drugs, potentially ensuring a smooth transition to mitigation strategies while minimizing the overall disease burden.
-
The findings and conclusions in this study are those of the authors and do not necessarily represent the official position of the funding agencies, the National Institutes of Health, or the U.S. Department of Health and Human Services.
HTML









| Citation: |

|