
 Download:
Download:




-
In 2008, the World Health Organization defined multimorbidity as the presence of two or more chronic conditions in an individual (1). Multimorbidity is associated with an increased risk of premature death, hospitalization, reduced function, depression, polypharmacy, worsened quality of life, and, thus, poses a substantial economic burden on health systems (2). However, few studies have shown the prevalence and patterns of multimorbidity among adults aged 18 years and older in China, most of which focused on middle-aged and older adults. This study used data from the 2018 China Chronic Disease and Risk Factor Surveillance (CCDRFS) to estimate the prevalence and patterns of multimorbidity among Chinese residents aged ≥18 years. For adults with two chronic conditions in China, hypertension and dyslipidemia were the most prevalent multimorbidity combination. For those with three, hypertension, dyslipidemia, and obesity were the most prevalent co-occurence of three chronic conditions. Effective prevention and control measures are essential to reduce the burden of multimorbidity in China.
The CCDRFS program was established in 2004 to provide periodic nationwide data on the prevalence of major chronic diseases and the associated behaviors and metabolic risk factors. Details of the design, objective, and survey methods of the CCDRFS have been described previously (3). In 2018, 194,811 individuals were invited and 184,876 participated yielding a 94.9% response rate. This study analyzed 163,972 participants aged ≥18 years in 2018. Those missing information on the included chronic diseases or conditions and sampling weights were excluded.
In this study, information on the following 12 chronic conditions with high prevalence in China that significantly affect health or decrease functional performance and quality of life was collected by the 2018 CCDRFS: cancer, hypertension, diabetes, dyslipidemia, heart disease, stroke, chronic kidney disease, chronic obstructive pulmonary disease (COPD), musculoskeletal disorders, cervical and lumbar diseases, digestive system disorders, and obesity. Additionally, the inclusion criteria also considered a core list of chronic conditions for any multimorbidity measurement as recommended by a systematic review (4). Although it is controversial whether obesity should be considered as a chronic condition or a risk factor in multimorbidity studies, the British Academy of Medical Sciences recommended that obesity should be reported in multimorbidity research wherever possible (5). In this study, multimorbidity was defined as the presence of two or more of the 12 chronic conditions coexisting in an individual.
To assess the 12 selected conditions, the CCDRFS used a combined method that included self-reports based on physician diagnosis, physical measurements, and/or laboratory tests. Participants were asked if they had previously been diagnosed with either of the 12 selected chronic conditions by a doctor at a township health center, community health center, or higher-level health center. The definition and diagnostic criteria of the included chronic conditions and methods of data collection are shown in
Supplementary Table S1 .Estimates of prevalence rate and their 95% confidence intervals (CIs) for multimorbidity were generated using a range of characteristics, including age group, sex, ethnicity, household income, residency, educational level, and region. The top three most common multimorbidity combinations with two and three chronic conditions were described by sex and age group.
Descriptive analyses were performed using frequencies for categorical variables and means [standard deviation (SD)] for continuous variables. For all estimates, sampling weights were used (3). Rao Scott chi-squared tests were used to test global differences, and logistic regression models were used to test for trends in ordinal categorical variables. Contingency tables were used to generate the most prevalent multimorbidity combinations of two and three chronic conditions. All differences were found to be statistically significant using two-tailed significance tests (P<0.05). All statistical analyses were performed using the SAS software package (version 9.4, SAS Institute, Inc. Cary, NC, USA), and Microsoft Office Excel 2019MSO (version 2205, Microsoft Corporation, Santa Rosa, California, USA) was used to generate the figures.
In this study, a total of 163,972 Chinese residents aged ≥18 years were included, with 72,444 (44.2%) males and 91,528 (55.8%) females. In 2018, 46.5% (95% CI: 45.6%–47.3%) had multimorbidity (Table 1). Men aged 18–59 years old were more likely to have multimorbidity than women. However, the prevalence was higher among women aged ≥60 years. The prevalence of multimorbidity increased with age, decreased with household income in all age groups, and decreased with educational levels among adults aged 18–44 years. Among adults with three or more chronic conditions, multimorbidity prevalence was higher among people with lower household income and educational levels than in the other groups (
Supplementary Table S2 ).Characteristics N ≥2 Chronic conditions, % (95% CI§) 18–44 years 45–59 years ≥60 years Total Total 163,972 32.1 (31.0−33.2) 59.8 (58.9−60.6) 74.6 (73.8−75.5) 46.5 (45.6−47.3) Gender Male 72,444 39.5 (38.0–41.0) 60.9 (59.7−62.1) 70.5 (69.5−71.6) 50.1 (49.0−51.2) Female 91,528 24.5 (23.2–25.8) 58.6 (57.7−59.5) 78.5 (77.6−79.4) 42.8 (41.7−43.9) P value for difference <0.0001 0.0005 <0.0001 <0.0001 Ethnicity Han 144,178 32.0 (30.9–33.2) 59.8 (58.9–60.7) 74.9 (74.1–75.8) 46.6 (45.7–47.6) Minorities 19,794 32.7 (30.6–34.8) 59.2 (57.6–60.8) 70.7 (68.6–72.8) 44.7 (43.0–46.3) P value for difference 0.6113 0.5313 <0.0001 0.0475 Residency Urban 67,262 32.8 (31.4–34.3) 59.2 (57.8–60.5) 77.2 (75.8–78.5) 45.6 (44.3–47.0) Rural 96,710 31.2 (29.8–32.6) 60.3 (59.3–61.4) 72.6 (71.7–73.5) 47.3 (46.2–48.4) P value for difference 0.109 0.1767 <0.0001 0.0521 Household income (CNY) <15,000 27,034 34.3 (31.5–37.0) 62.1 (60.5–63.7) 73.1 (72.0–74.3) 53.3 (51.6–55.0) 15,000– 33,681 32.9 (30.5–35.3) 60.5 (59.1–62.0) 73.1 (71.7–74.5) 48.1 (46.6–49.5) 30,000– 35,819 33.8 (31.9–35.8) 59.2 (57.8–60.6) 76.5 (75.1–77.8) 46.7 (45.2–48.2) >60,000 29,759 30.8 (29.0–32.7) 57.8 (56.3–59.3) 77.1 (75.4–78.7) 42.1 (40.4–43.7) Unwilling to disclosure 37,679 30.4 (28.5–32.4) 60.1 (58.5–61.7) 73.9 (72.7–75.0) 45.8 (44.3–47.4) P value for trend¶ 0.0385 0.0001 <0.0001 <0.0001 Education Illiterate 25,900 39.3 (34.4–44.2) 62.6 (61.0–64.2) 76.1 (74.8–77.3) 67.4 (66.0–68.8) Primary 55,295 39.9 (37.6–42.1) 59.5 (58.4–60.7) 73.7 (72.7–74.7) 56.5 (55.2–57.8) Secondary 71,397 32.5 (31.1–33.8) 60.3 (59.2–61.4) 74.4 (72.7–76.0) 44.1 (42.9–45.3) Tertiary or higher 11,380 26.6 (24.9–28.4) 52.5 (49.9–55.2) 75.6 (72.7–78.4) 30.1 (28.4–31.8) P value for trend <0.0001 0.1070 0.9703 <0.0001 Region East 61,661 32.0 (30.3–33.7) 59.4 (58.0–60.7) 75.7 (74.4–77.0) 46.4 (44.9–47.8) Center 46,605 33.3 (31.6–35.1) 60.7 (59.0–62.4) 75.6 (74.1–77.0) 47.8 (46.1–49.4) West 55,706 30.9 (28.8–33.0) 59.3 (57.7–60.8) 71.8 (70.3–73.3) 45.0 (43.5–46.6) P value for difference 0.2645 0.3941 0.0003 0.0947 Abbreviation: CI=confidence interval; CNY=Chinese Yuan.
* Adults considered with multimorbidity are persons who had been diagnosed by a healthcare professional that they had two or more of the following 12 conditions: cancer, hypertension, diabetes, dyslipidemia, heart disease, stroke, chronic kidney disease, chronic obstructive pulmonary disease (COPD), musculoskeletal disorders, cervical and lumbar diseases, digestive system disorders, and obesity.
† Table presented weighted prevalence, which represents the overall national population. The standard population estimation for 2010 were obtained from the National Bureau of Statistics of China.
§ Considered complex survey design.
¶ Category “unwilling to disclosure” was excluded in the trend test.Table 1. Prevalence of multimorbidity* among adults aged 18 years and older — China, 2018†.
Most people with any of the 12 chronic conditions examined had two or more conditions rather than a single condition alone (Figure 1). People with stroke and heart disease were more likely to suffer from multimorbidity.
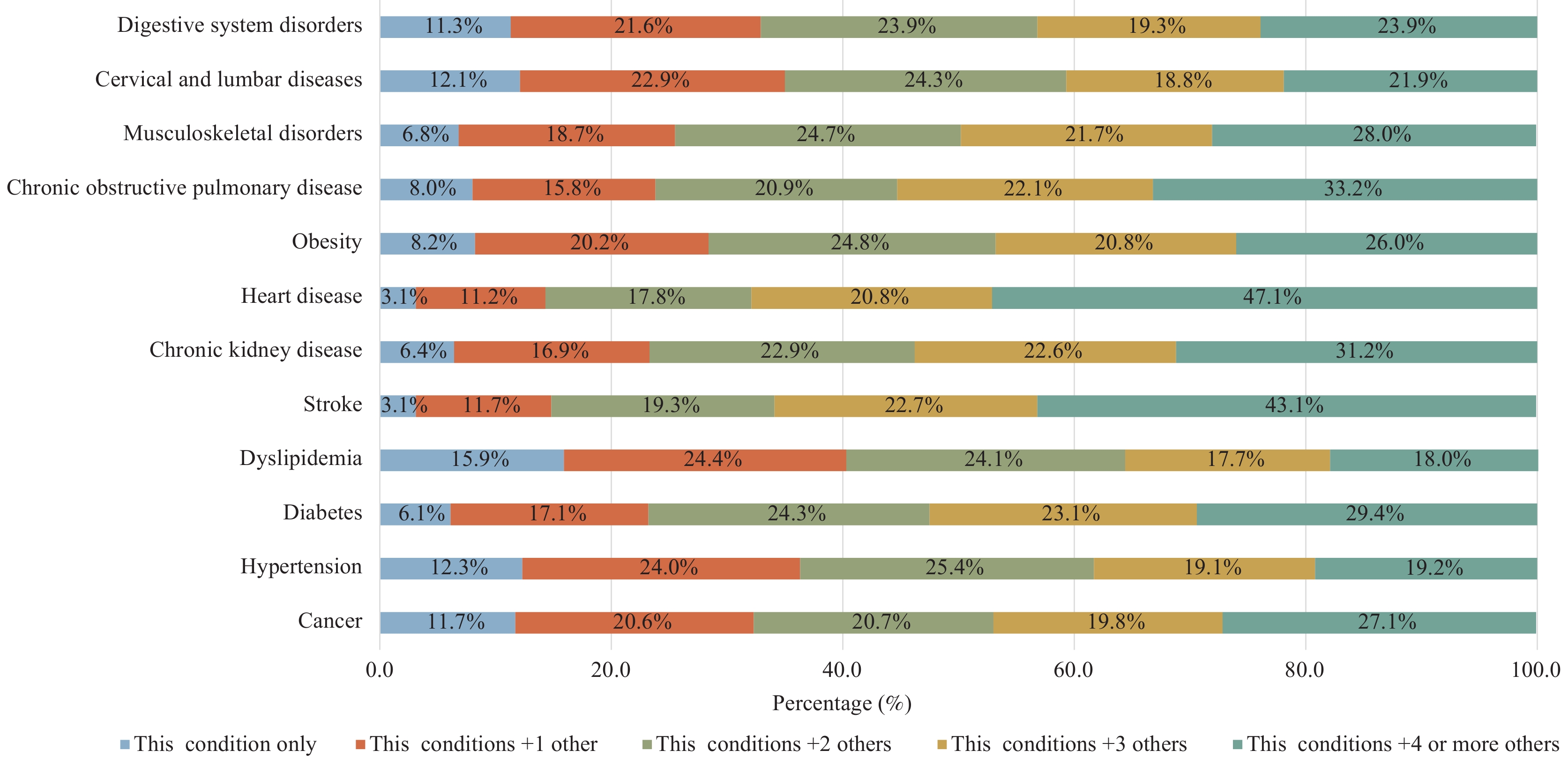 Figure 1.
Figure 1.Distribution of multimorbidity of each chronic disease among adults — China, 2018.
Abbreviation: COPD=chronic obstructive pulmonary disease.For adults with two chronic conditions in China, the most prevalent multimorbidity combination of two chronic conditions was hypertension and dyslipidemia (12.9%) (Table 2). Additionally, it was also the most prevalent among people aged ≥45 years. The second most common combination of two chronic condition was dyslipidemia and obesity (12.8%). Among Chinese adults with three chronic conditions, hypertension, dyslipidemia, and obesity was the most prevalent (12.4%) (Table 2).
Characteristics With two chronic conditions Prevalence
% (95% CI§)With three chronic conditions Prevalence
% (95% CI§)Total 1 Hypertension + Dyslipidemia 12.9 (12.1–13.8) Hypertension + Dyslipidemia + Obesity 12.4 (11.3–13.6) 2 Dyslipidemia + Obesity 12.8 (11.6–14.1) Hypertension + Diabetes + Dyslipidemia 6.1 (5.5–6.7) 3 Dyslipidemia + Cervical and lumbar diseases 9.7 (9.0–10.3) Hypertension + Dyslipidemia + Cervical and lumbar diseases 5.4 (4.9–5.9) Gender Male 1 Dyslipidemia + Obesity 16.1 (14.3–18.0) Hypertension + Dyslipidemia + Obesity 16.0 (14.3–17.6) 2 Hypertension + Dyslipidemia 15.2 (14.0–16.3) Hypertension + Diabetes + Dyslipidemia 6.7 (5.8–7.6) 3 Dyslipidemia + Cervical and lumbar diseases 9.3 (8.4–10.2) Hypertension + Dyslipidemia + Cervical and lumbar diseases 5.5 (4.7–6.2) Female 1 Cervical and lumbar diseases + Digestive system disorders 11.8 (10.6–12.9) Hypertension + Dyslipidemia + Obesity 8.2 (6.9–9.4) 2 Dyslipidemia + Cervical and lumbar diseases 10.2 (9.0–11.5) Musculoskeletal diseases + Cervical and lumbar diseases + Digestive system disorders 6.6 (5.9–7.3) 3 Hypertension + Dyslipidemia 10.2 (9.4–10.9) Hypertension + Diabetes + Dyslipidemia 5.4 (4.8–6.0) Age groups (years) 18–44 1 Dyslipidemia + Obesity 21.4 (19.4–23.5) Hypertension + Dyslipidemia + Obesity 21.0 (18.6–23.4) 2 Dyslipidemia + Cervical and lumbar diseases 11.8 (10.5–13.0) Dyslipidemia + Cervical and lumbar diseases + Digestive system disorders 6.6 (5.2–8.0) 3 Hypertension + Dyslipidemia 9.4 (8.0–10.9) Dyslipidemia + Obesity + Cervical and lumbar diseases 5.7 (4.6–6.6) 45–59 1 Hypertension + Dyslipidemia 15.5 (14.5–16.6) Hypertension + Dyslipidemia + Obesity 9.7 (8.9–10.6) 2 Dyslipidemia + Cervical and lumbar diseases 9.4 (8.8–10.0) Hypertension + Dyslipidemia + Cervical and lumbar diseases 7.0 (6.3–7.8) 3 Cervical and lumbar diseases + Digestive system disorders 7.7 (7.1–8.2) Hypertension +Diabetes + Dyslipidemia 7.0 (6.2–7.8) ≥60 1 Hypertension + Dyslipidemia 16.2 (15.3–17.1) Hypertension + Diabetes + Dyslipidemia 8.0 (7.3–8.8) 2 Hypertension + Chronic kidney diseases 7.7 (7.0–8.5) Hypertension + Musculoskeletal diseases + Cervical and lumbar diseases 5.6 (5.0–6.3) 3 Hypertension + Diabetes 7.6 (6.9–8.3) Hypertension + Dyslipidemia + Chronic kidney diseases 5.2 (4.5–5.9) * Adults considered with multimorbidity are persons who had been diagnosed by a healthcare professional that they had two or more of the following 12 conditions: cancer, hypertension, diabetes, dyslipidemia, heart disease, stroke, chronic kidney disease, chronic obstructive pulmonary disease (COPD), musculoskeletal disorders, cervical and lumbar diseases, digestive system disorders, and obesity.
† Table presented weighted prevalence, which represents the overall national population. Standard population estimation for the year 2010 were obtained from the National Bureau of Statistics of China.
§ CI=confidence interval, considered complex survey design.Table 2. Top 3 prevalent multimorbidity* combination of two and three chronic conditions among adults ― China, 2018†.
-
In 2018, the prevalence of multimorbidity among Chinese adults aged ≥18 years was 46.5%. Previous systematic reviews have reported that the pooled prevalence of multimorbidity was 42.4% (6). Estimates of multimorbidity prevalence vary widely across studies due to the lack of consensus on the definition and the number of chronic conditions included. Multimorbidity is common in all age groups in this study, especially among the elderly. This implies that research and prevention strategies for multimorbidity should not only focus on the elderly but should also recognize its impact among young and middle-aged adults. Men aged 18–59 years and women aged ≥60 years had a higher prevalence of multimorbidity. Menopausal and postmenopausal women experience hormonal changes accompanied by an increased risk of several chronic diseases, which may lead to higher multimorbidity prevalence among women aged ≥60 years (7). The prevalence of multimorbidity increased with age, consistent with previous studies (8). Many studies worldwide have confirmed that increasing age has a large impact on multimorbidity prevalence. The goal for older people with multimorbidity is to improve functional limitations and reduce adverse effects stimulated by chronic illness, and current best practices for the young population should focus on the prevention of common risk factors. Furthermore, the prevalence of multimorbidity decreased with household income in all age groups, and it decreased with educational levels among adults aged 18–44 years. According to a previous study, a low education level was significantly associated with the likelihood of multimorbidity (9). Health awareness was higher among those with higher education levels than among those with lower education levels. Additionally, multimorbidity is strongly associated with socioeconomic deprivation (8). This suggests that future strategies designed to reduce multimorbidity should consider the importance of socioeconomic status factors. Most individuals with selected chronic conditions have at least two or more diseases. Participants with stroke and heart disease had the highest multimorbidity prevalence, which was similar to the findings of previous studies (8).
Hypertension and dyslipidemia were the most prevalent co-occurence of two chronic conditions among Chinese adults, and dyslipidemia, hypertension, and obesity were the most prevalent co-occurence of three chronic conditions. According to a systemic review in Asia, cardiovascular and metabolic diseases were the most prevalent multimorbidity pattern, and the most common diseases identified in this pattern included hypertension, diabetes, dyslipidemia, coronary heart disease, kidney disease, stroke, and obesity (10). The combination of hypertension and dyslipidemia may be linked to increasing obesity in the Chinese people. Moreover, obesity is also associated with multimorbidity. Notably, some chronic conditions are considered to be risk factors for other more serious diseases, for example, hypertension can often lead to cardiovascular disease and stroke. The identification of these multimorbidity patterns could potentially recognize more serious diseases. Understanding the reasons for disease clusters may help to identify the possible etiology of clusters and prevent their development in the first place. On the other hand, from a clinical perspective, the identification of multimorbidity patterns contributes to developing more targeted treatments and care plans for patients with multimorbidity.
This study has some limitations. First, no mental health conditions were included in the study. Thus, the prevalence of multimorbidity might have been underestimated. Second, some chronic diseases were self-reported, leading to an underestimation owing to information bias. Third, some missing data on chronic conditions were excluded, resulting in significant differences in age, income, and ethnicity between the included participants and the excluded participants with missing values. This suggests that population representation was relatively limited. Therefore, the generalizability of the findings to other populations should be interpreted with caution.
In conclusion, this study used a nationally representative sample of Chinese adults to assess the prevalence and common patterns of multimorbidity. It is important to shift from single disease-oriented clinical guidelines to multimorbidity frameworks in Chinese populations, particularly among the elderly, people with low income, and those with low educational levels.
-
No conflicts of interest.
HTML
| Citation: |

|