

 Download:
Download:




-
Cervical cancer is a major public health problem among women in China. China is one of the few countries experiencing an increase in cervical cancer incidence (1). Middle-aged females with large social and family responsibilities are at high risk of cervical cancer incidence, which results in poor health outcomes and an increased financial burden. Therefore, there has been much concern about the changing trend in age distribution of cervical cancer.
In recent years, the Chinese government has devoted resources to preventing and treating cervical cancer in rural areas (2). Currently, there is a gap in the literature examining incidence and mortality of cervical cancer in China (3). Hence, we aimed to describe the trends in incidence and mortality rates of cervical cancer from 2003 to 2017 and to identify risk factors for cervical cancer by geography. Our study can provide references for effectiveness evaluation of existing anticancer strategies and for future policy planning in China.
-
We extracted and pooled cervical cancer datasets (codes: C53, International Statistical Classification of Diseases and Related Health Problems 10th Revision) of 22 population-based cancer registries (11 in urban areas and 11 in rural areas) from 2003 to 2017 in China. A total of 41,326 cervical cancer cases and 10,863 cancer deaths from a population of 329,750,392 person-years (35,420 cases and 8,899 deaths from 274,073,539 person-years in urban areas and 5,906 cases and 1,964 deaths from 55,676,853 person-years in rural areas).
We excluded data from females over 20 years old since the number of cases and deaths of females in this population was less than 5 in each age group (n<5). We classified districts as urban areas and counties/county-level cities as rural areas. The incidence and mortality rates were calculated using 5-year age grouping (20–24, 25–29,…, 80–, ≥85), by 5-year period (2003–2007, 2008–2012, 2013–2017) and by geography (urban and rural areas).
-
The age-standardized incidence rate (ASIR) and mortality rate (ASMR) were calculated using Segi’s world standard population (4). We used Joinpoint regression analyses for trend analysis and reported the annual percent changes (APC), and average annual percent change (AAPC). Age-period-cohort effects were analyzed using the intrinsic estimator method and risk ratios were reported (5). Statistical analyses were performed using Stata (version 13.0, Stata Corporation, College Station, Texas, USA) and Joinpoint software (version 4.6.0.0 Applications Branch, National Cancer Institute, Bethesda, USA).
-
Supplementary Table S1 presents the incidence rates of cervical cancer. Overall, the ASIR for cervical cancer in females over 20 years old increased from 6.66/100,000 in 2003 to 16.30/100,000 in 2017. A clear upward trend was observed during 2003−2007, but this trend dampened during 2007−2017. In urban areas, the ASIR increased from 6.91/100,000 in 2003 to 16.15/100,000 in 2017. ASIR increased significantly during 2003–2009, and then leveled off. In rural areas, the ASIR increased from 5.72/100,000 in 2003 to 17.07/100,000 in 2017. The ASIR increased during 2003−2007, however, this upward trend slowed down during 2007−2017 (Figures 1A, 1B, 1C). The corresponding APCs and AAPCs for incidence rates were provided inSupplementary Table S2 . Figure 1.
Figure 1.The trends of incidence and mortality rates of cervical cancer by age group and area, from 2003 to 2017. (A) Incidence rates in all areas, (B) Incidence rates in urban areas, (C) Incidence rates in rural areas, (D) Mortality rates in all areas, (E) Mortality rates in urban areas, (F) Mortality rates in rural areas.
In urban areas, the ASIR in females aged 20–34 years decreased significantly from 2003–2017. The ASIR in females aged 35–49 years varied, increasing from 2003–2009, then decreasing from 2009–2017. The ASIR in females aged 50–64 years increased significantly during 2003–2006, however, this upward trend slowed down afterwards. The ASIR in females over 65 years increased during 2003–2017 (Figure 1B).
In rural areas, the ASIR in females aged 20–34 years and 50–64 years increased significantly during 2003–2017. The ASIR in females aged 35–49 years increased during 2003–2017. The ASIR in females over 65 years was stable during 2003–2010 but increased rapidly afterward (Figure 1C).
-
Supplementary Table S3 presents the mortality rates of cervical cancer. In all areas, the ASMR increased from 2.07/100,000 in 2003 to 4.16/100,000 in 2017. In urban areas, it increased from 1.86/100,000 in 2003 to 3.91/100,000 in 2017. In rural areas, it increased from 3.12/100,000 in 2003 to 5.56/100,000 in 2017. The ASMRs all followed continuously increasing trends (Figures 1D, 1E, and 1F). The corresponding APCs and AAPCs for mortality rates were provided inSupplementary Table S4 .In urban areas, the ASMR in females aged 20–34 years stayed stable. The ASMR in females aged 35−49 years increased during 2003−2007 and then leveled off. The ASMR in females aged 50−64 years and over 65 years increased during the whole period of 2003−2017 (Figure 1E).
In rural areas, the increasing trend of ASMR in females aged 20−34 years was not significant. The ASMR in females aged 35−49 years increased during 2003−2017. The ASMR in females aged 50−64 years stayed stable. The ASMR in females over 65 years fluctuated during 2003−2009 and then increased during 2009−2017 (Figure 1F).
-
In urban areas, the peak age group for the incidence rate rose by one age group each 5-year period, from 40−44 years during 2003−2007 to 45−49 years during 2008−2012, and to 50−54 years during 2013−2017. Compared to period 2008−2012, the age-specific rates were lower in age groups <45 in period 2013−2017. The trends in all areas were similar to those in urban areas (Figure 2B).
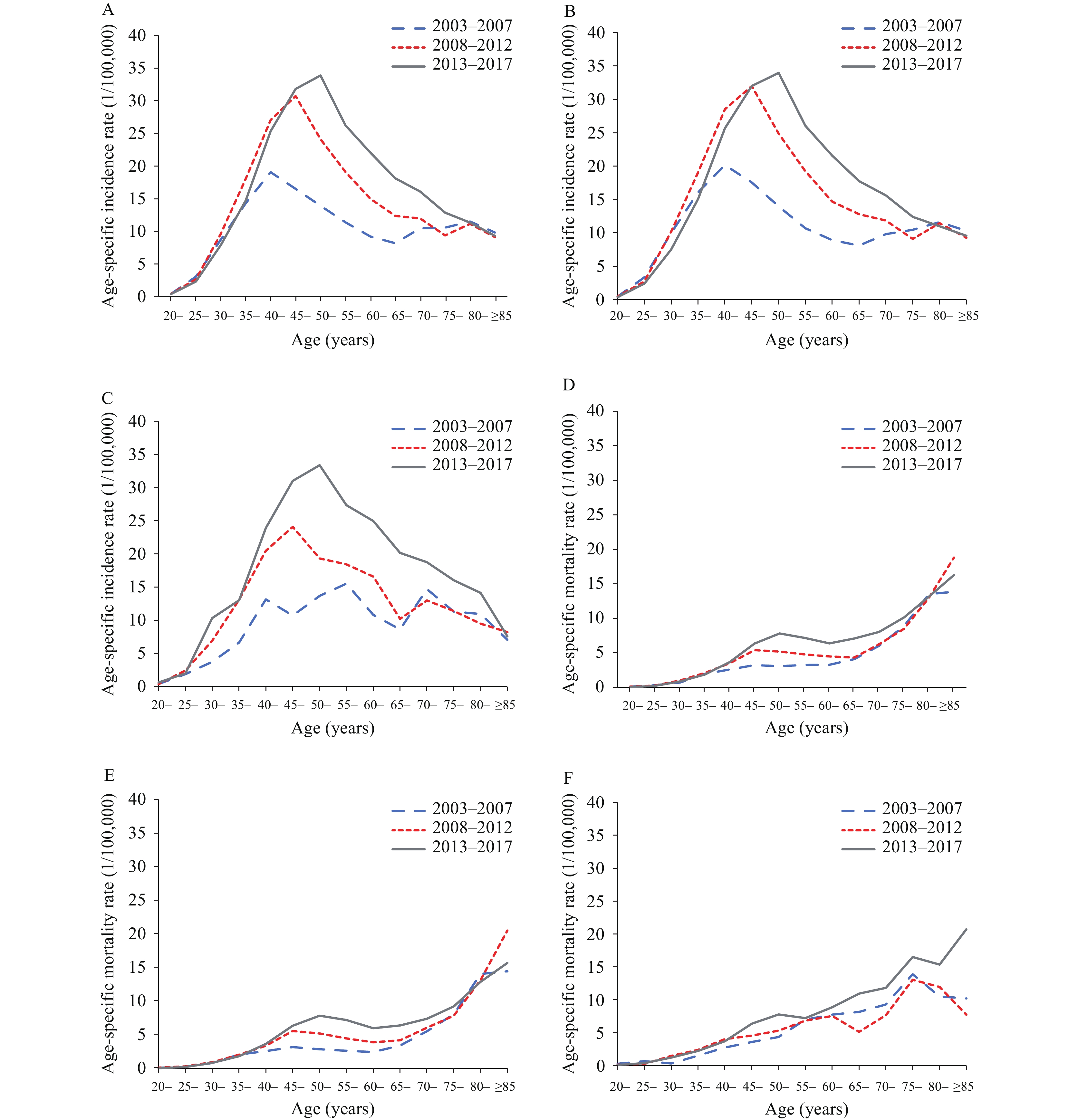 Figure 2.
Figure 2.The age-specific incidence and mortality rates of cervical cancer, by time period and area. (A) Incident rates in all areas. (B) Incident rates in urban areas. (C) Incident rates in rural areas. (D) Mortality rates in all areas. (E) Mortality rates in urban areas. (F) Mortality rates in rural areas.
Note: Each line represents the connection of age-specific rates for a 5-year period.In rural areas, the age group with the highest incidence rate was 55−59 years during 2003−2007. It decreased to 45−49 age group during 2008−2012, and then rose to 50−54 age group during 2013−2017. The age-specific incidences in most age groups increased with period (Figure 2C).
The incidence rates increased for cohorts between 1928 and 1978 (25−79 years) in urban areas and cohorts between 1918 and 1978 (>25 years) in rural areas (Figures 3A, 3B).
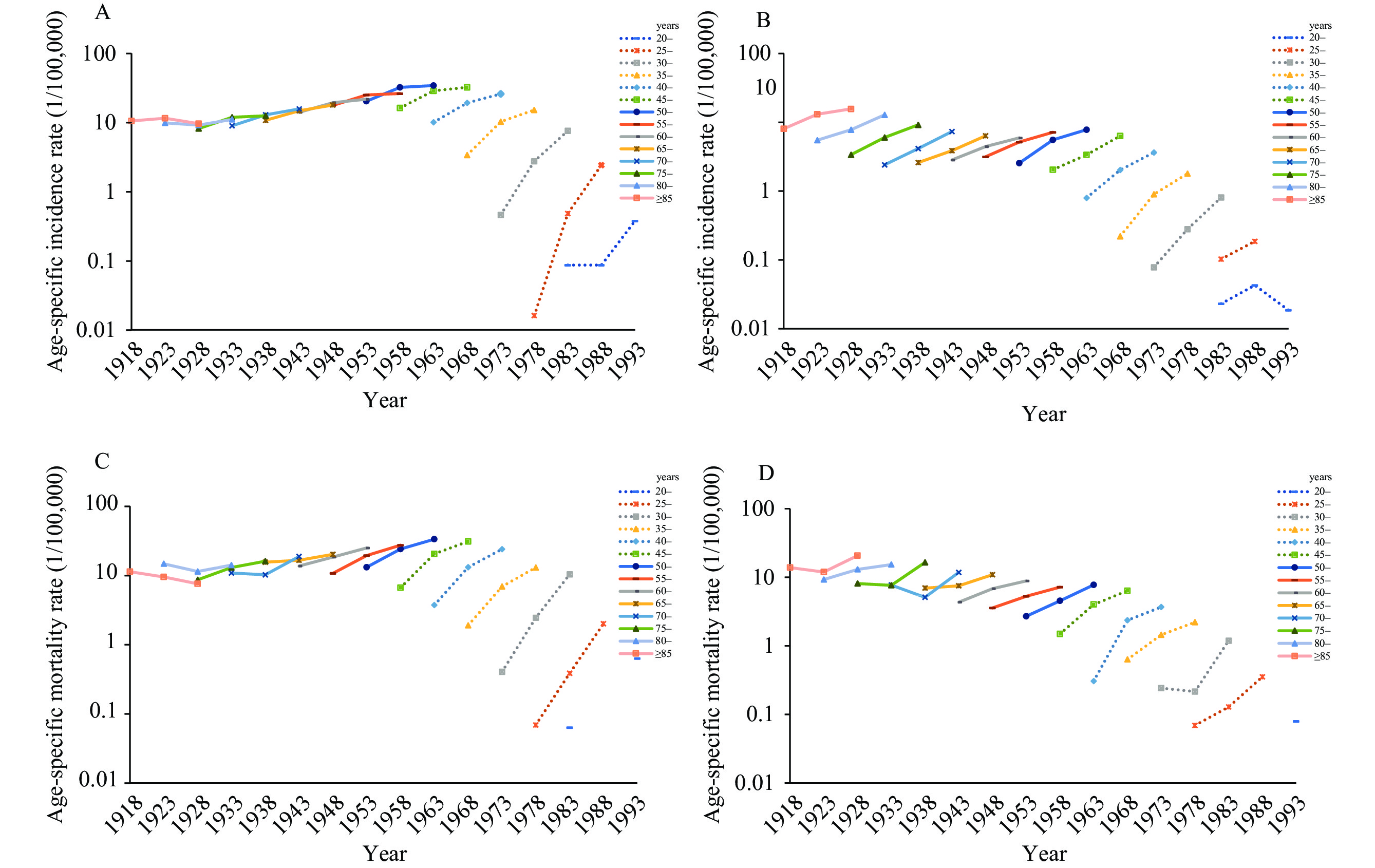 Figure 3.
Figure 3.The birth cohort-specific incidence and mortality rates of cervical cancer, by area. (A) Incident rates in urban areas. (B) Incident rates in rural areas. (C) Mortality rates in urban areas. (D) Mortality rates in rural areas.
Note: Results are not shown in age group 20–24 if the age-specific rate is 0. Each line represents the connection of cohort-specific rates for a 5-year age group. -
In urban areas, the age-specific mortality rate peaked at 45–49 years during 2003–2012 and at 50–54 years during 2013–2017. From the 60–64 year age group, mortality rates increased continuously with age. The trends in all areas were similar to those in urban areas (Figure 2E).
In rural areas, the mortality rate increased with age all along, and no peaks were found in young age groups (Figure 2F).
The mortality rates of cervical cancer increased for younger cohorts between 1943 and 1978 but fluctuated in elder cohorts between 1918 and 1938 in both urban and rural areas (Figures 3C, 3D).
-
The age effect for cervical cancer incidence rates rose significantly from age groups 20–24 and peaked in the age groups of 45–49 (urban) and 50–54 (rural). It began to decrease slowly afterward but rose again in the age group of 70–74. The age effect dropped rapidly in subsequent age groups. The age effect on mortality rates increased with age all through in urban areas but fluctuated in elder age groups in rural areas (Figure 4).
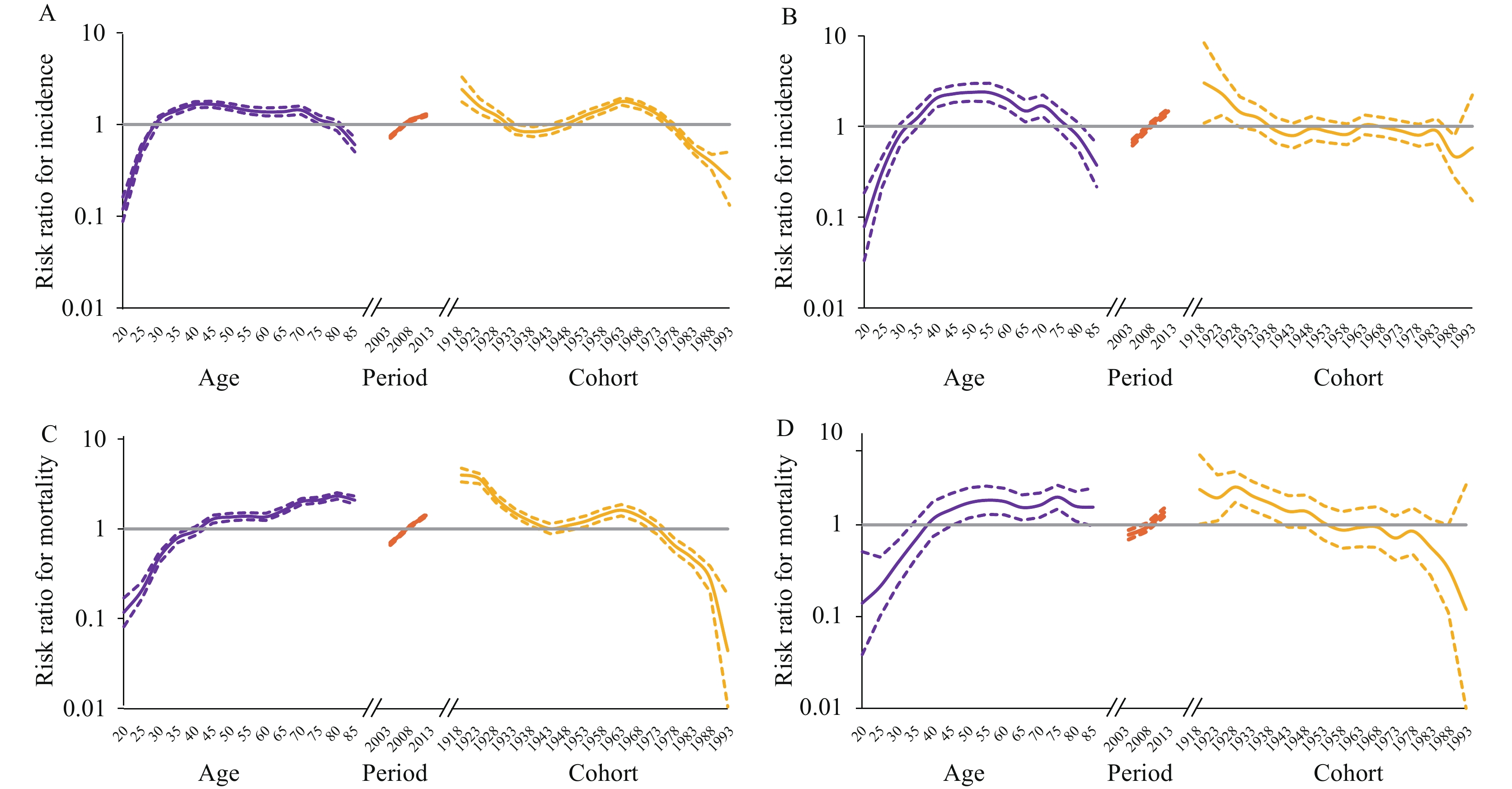 Figure 4.
Figure 4.The result of age-period-cohort analysis of incidence and mortality rates of cervical cancer, by area. (A) Incident rates in urban areas; (B) Incident rates in rural areas; (C) Mortality rates in urban areas; (D) Mortality rates in rural areas.
Notes: Purple solid and dash lines represent the age effect and 95% confidence interval. Orange solid and dash lines represent the period effect and 95% confidence interval. Yellow solid and dash lines represent the cohort effect and 95% confidence interval.The period effect for the incidence and mortality rates of cervical cancer increased during 2003 to 2017 in urban and rural areas (Figure 4).
For cohort effects in urban areas, the risk ratios of incidence and mortality rates decreased in birth cohorts 1918–1938 and 1918–1943, respectively. Then the risk ratios increased in birth cohorts 1938–1963 and 1943–1963, and decreased after 1963. In rural areas, the risk ratios of incidence rate decreased in birth cohort 1918–1943 and then fluctuated after that. The risk ratios of mortality rate decreased among all cohorts from 1918 to 1993 (Figure 4). The age-period-cohort estimates were provided in
Supplementary Table S5–S6 . -
Shift in trends. Wang et al. (6) showed that the incident rates of cervical cancer were highest in younger populations in Italy and Korea. Similar trends were also observed in China whereby Wei et al. (7) found that the mortality rate of cervical cancer increased in young females aged 25–54 from 1987 to 2015 in urban China, which was different from the results in our study. Li et al. (3) used cancer registry data and reported that the risk for younger females was rising in China. In this study, we updated the same cancer registry data for 3 years and found contrasting trends in incidence/mortality rates in younger females (<50) in recent 8 years, which were more significant in urban areas than in rural areas. This evidence indicated that the increasing trend in cervical cancer disease burden in younger females was being arrested in urban areas.
Age effect. We observed that the risk for cervical cancer incidence plateaued at age 40–74 in China, which was also observed in India (8) and Russia (9), indicating that the age span of targeted population for cervical cancer screening programs can be larger.
Period effect. The increased trends in cervical cancer incidence and mortality rates can be explained by period effects, which are caused by factors that can influence all age groups during a particular period of time. Considering that the National Cervical Cancer Screening Program in Rural Areas (NCCSPRA) was launched in 2009 for females aged 35–59, the effect of this screening program may have resulted in the cohorts rather than the periods in China. Guo et al. (10) also reported similar period effects on cervical cancer mortality. The possible explanation might also be the cumulative exposure to risk factors during the industrialization and urbanization processes, the improvement of health service capacity and the increasing demand for cancer treatment. Surveillance data indicated that the cancer incidence and mortality rates are still on the rise and the turning point is not yet in sight in China (11). Without harsher and more extensive intervention measures, the period effect is expected to keep rising in the near future (12).
Cohort effect. Cohort effect explains the influence of unique risk factors for different birth cohorts. In urban areas, risk ratios increased among females born in 1938–1963, which was echoed in Guo’s research (10). Possible explanations include an increase in HPV infection and smoking rate and changing sexual behaviors in 1938–1963 cohorts (13). The risk ratios decreased among females born after 1963, which might be explained by the cancer intervention strategies implemented in recent years, including health education, the promotion of women’s health care and the implementation of extensive cervical cancer screening programs after 2009. In rural areas, we observed no upward trends in cohort effects on incidence rate and decreased cohort effects on mortality rates, indicating that the cervical cancer intervention strategies in these areas have achieved promising effects. Increasing cohort effects were found in young generations in the Republic of Korea (14), Japan (15) and Russia (9) but were not observed in the present study. Considering that similar risk factors may also exist in China, corresponding public health measures for young generations should be implemented in advance.
In conclusion, the disease burden of cervical cancer in China is still on the rise, but the upward trend in young generations in urban areas is starting to slow down or even reverse. The decrease of cohort effects may reflect the effect of cervical cancer prevention and control strategies in China in recent years, which mainly affected females born after 1963 in urban areas and all females in rural areas. More comprehensive interventions for general female population with strengthened measures for young generations should be implemented in China.
-
Staffs of 22 population-based cancer registries for the effort they put in data collection, quality control and database creation, including Beijing Municipality; Cixian County in Hebei Province; Dalian and Anshan cities in Liaoning Province; Nangang District in Heilongjiang Province; Shanghai Municipality; Qidong City, Huai’an District, and Yangzhong City in Jiangsu Province; Hangzhou City, Jiaxing City , Jiashan County, and Haining City in Zhejiang Province; Changle District in Fujian Province; Linqu County and Feicheng City in Shandong Province; Linzhou City in Henan Province; Wuhan City in Hubei Province; Guangzhou, Sihui, and Zhongshan cities in Guangdong Province; and Yanting County in Sichuan Province.
-
No conflicts of interest.
HTML
Cancer Registry Data
Statistical Analysis
Trends in Incidence Rate
Trends in Mortality Rate
Trends in Age Distribution of Cervical Cancer Incidence
Trends in Age Distribution of Cervical Cancer Mortality
Results of Age-period-cohort Models
| Citation: |

|