

 Download:
Download:




-
Globally, over 55 million people live with dementia, and the aggregate financial burden of the disease is over 1 trillion US dollars annually (1-2). This burden has been growing rapidly in China, which habilitates almost one-fourth of the total dementia cases worldwide (3-4). Prior research shows that the prevalence of dementia in China is high and differs geographically (3-4). However, no previous study has revealed the geographic patterns of dementia care and costs in China. To bridge that gap, we used administrative data from an extensive national database to characterize the geographic patterns in healthcare utilization, outcomes, and costs for patients hospitalized for dementia in China. We obtained novel estimates at both the provincial and national levels to enrich the understanding of the disease burden nationwide and facilitate the effective allocation of resources for dementia care. Our results demonstrated significant geographic disparities in inpatient care utilization, outcomes, and costs for patients hospitalized for dementia in China across provincial-level administrative divisions (PLADs). Specifically, we found notable geographic clusters in inpatient care costs and length of stay. These regional patterns imply gaps in equity and efficiency of dementia care and management for this rapidly growing population of dementia patients. Future policies and practices should consider these geographical disparities and promote a more equitable system for dementia care.
Hospital service data were obtained through the Data Center for High-Quality Hospital Management at Peking University Institute for Global Health and Development. The Center integrates data on healthcare services and management of representative hospitals in China for health policy and management research. The national sample covers 30 PLADs except for Xizang (Tibet) Autonomous Region; Taiwan, China; Hong Kong Special Administrative Region (SAR); and Macau SAR, making it a representative sample for understanding geographic variations. The dataset, spanning from June 2017 to June 2019, provides information on inpatient records, including admission type, dates of admission and discharge, primary and secondary diagnoses, comorbidities, and costs. To ensure that the care utilization and costs were related directly to dementia, we extracted inpatient records with primary diagnosis as dementia based on the International Classification of Disease (ICD) codes (
Supplementary Table S1 ).Since dementia is an age-related condition, we restricted samples to patients aged 65 years or older at admission. Samples with a respective 2% of the highest and lowest total inpatient care costs were excluded from the analysis to mitigate the influence of extreme values; and the results were similar if we excluded extreme values based on other criteria (e.g., excluding 1% of the highest and lowest). Overall, 1,917 hospitals in the database had valid dementia cases (51,530 total cases), with 960 (50.1%) tertiary hospitals and 957 (49.9%) secondary hospitals or below. The distribution of hospitals and cases by PLAD is further illustrated in
Supplementary Figure S1 , where the total number of hospitals (and cases) and the proportion of types of hospitals are presented for each PLAD.In this study, the inpatient care utilization, i.e., the number of hospital admissions due to dementia per 100,000 person-years, was first assessed for each PLAD. This assessment utilized our medical records data and data from China Statistical Yearbook for hospital admission and provincial population (5). Specifically, we scaled our total number of dementia admissions by the ratio of hospital admissions included in our database to the total hospital admissions from the Yearbook. The provincial population aged 65 or older and the observed periods were used as the denominator. Second, we evaluated the disease severity/urgency and outcomes of hospital admissions for dementia patients. Specifically, we used the percentage of emergency room (ER) admission and the number of comorbidities to reflect the disease severity/urgency of admission; and we used the percentage of in-hospital mortality as an indicator for care outcomes. The number of comorbidities was calculated as the sum of all coexisting diagnosed conditions documented at the time of admission using ICD codes. The in-hospital mortality was calculated as the proportion of patients who died during hospitalization among all dementia inpatient admissions. Third, we estimated the average total costs per admission based on the total hospital expenditure reported for each admission (including out-of-pocket and insurance-covered expenses), the average length of stay (LOS), and the average daily cost per admission to assess the care intensity during the hospitalization.
The quality of data was highly reliable, with limited missing records and extreme cases. Specifically, we found no missing data for all measures except for mortality outcome (with only <0.01% missing records). No extreme cases with values outside valid/possible ranges were found in our data. For each outcome, we calculated the national average, by averaging the provincial estimates of the outcome. Furthermore, using Moran’s I statistic, we examined spatial autocorrelation and clustering using the distance decay parameter of 2. STATA (release 16.0, Stata Corp) and R (version 4.0.2, R Core Team) were used to perform the analyses.
Figure 1 displayed the geographic patterns of inpatient care utilization, severity/urgency, and outcomes. Panel A presented the number of dementia-related hospital admissions per 100,000 person-years for each PLAD. The national average number of dementia admissions was 111 [95% confidence interval (CI): 72–149] per 100,000 person-years. The utilization rate of care was higher in western PLADs and some central and southern PLADs, such as Xinjiang Uygur Autonomous Region (579), Yunnan Province (218), Guizhou Province (181), and Guangdong Province (273), but lower in northeastern PLADs. Panel B presented the percentage of ER admissions among all dementia admissions. The national average across PLADs was 19.5% (95% CI: 15.8%–23.2%). At the provincial level, the percentage of ER admissions ranged from 3.2% in Inner Mongolia Autonomous Region to 40.5% in Shanghai Municipality. Some PLADs with high percentages of ER admissions included Beijing Municipality (38.2%), Jilin Province (37.0%), Guizhou Province (33.4%), Qinghai Province (31.7%), Henan Province (31.3%), and Heilongjiang Province (30.3%). Panel C presented the average number of comorbidities per admission. Hospitalized dementia patients generally had multiple comorbidities. The national average across PLADs was 5.5 (95% CI: 4.9–6.1) comorbidities; and at the provincial level, the average number of comorbidities ranged from 3.1 in Liaoning Province to 9.5 in Yunnan Province. The average number of comorbidities in patients was higher in western PLADs and some eastern or northern PLADs, such as Xinjiang Uygur Autonomous Region (7.6), Qinghai Province (7.5), Fujian Province (8.9), Zhejiang Province (7.0), and Beijing Municipality (7.5), as compared to others. Lastly, for care outcomes, Panel D displayed the percentage of in-hospital mortality among all dementia-related admissions. The national average across PLADs was 1.0% (95% CI: 0.5%–1.4%). Northern PLADs had the highest percentage of in-hospital mortality, including Inner Mongolia Autonomous Region (6.5%), Heilongjiang Province (2.5%), Jilin Province (1.8%), and Liaoning Province (1.3%). The Moran’s I statistics were all very small and no significant spatial autocorrelation was found for these measures except for the utilization rate.
 Figure 1.
Figure 1.Geographical variation in health care utilization and outcomes for hospitalized dementia patients in China. (A) Number of hospital admissions due to dementia per 100,000 person-years; (B) percentage of emergency room admissions (%); (C) average number of comorbidities; (D) percentage of in-hospital mortality (%).
Note: In each panel, the sample period was from June 2017 to June 2019; and data were available for all PLADs except for Xizang (Tibet); Taiwan, China; Hong Kong SAR; and Macau SAR. Moran’s I statistic for spatial autocorrelation is displayed at the bottom; and the national average across PLADs is displayed on the right with 95% CI presented in the parentheses. The following terms were used interchangeably: Xizang=Xizang (Tibet); Nei Mongol=Inner Mongolia; Zizhiqu=Autonomous Region.
Abbreviation: PLAD=provincial-level administrative division; SAR=Special Administrative Region; CI=confidence interval.
Figure 2 further illustrated the geographic variation in average total costs, daily costs, and LOS per admission, as measures of care intensity and disease burden. Panel A presented the average total costs per admission. The national average total cost across PLADs was 14,755 (95% CI: 12,738–16,772) CNY per admission which presented clear geographic patterns at the provincial level. Notably, the average total costs per admission were highest among Jing-Jin-Ji metropolitan area (i.e., Tianjin Municipality: 35,357; Beijing Municipality: 28,660; and Hebei Province: 15,618) and were consistently higher among eastern or southern coastal PLADs (e.g., Fujian Province: 22,072; Shanghai Municipality: 19,624; and Zhejiang Province: 17,406) than others. Panels B and C, presented the average daily costs and LOS per admission. At the national level, the average daily costs were 1,171 (95% CI: 965–1,377) CNY, and the average LOS was 15.5 (95% CI: 13.7–17.4) days per admission. At the provincial level, the average daily costs were higher among Jing-Jin-Ji metropolitan area and some northern PLADs than others, including Beijing Municipality (3,491), Tianjin Municipality (2,818), Hebei Province (1,385), Inner Mongolia Autonomous Region (1,442), and Jilin Province (1,175). The average daily costs were also relatively high in some coastal PLADs, such as Shanghai Municipality (1,385) and Guangdong Province (1,126). By contrast, the LOS was highest in coastal areas and some western PLADs, such as Fujian Province (23.0), Zhejiang Province (23.0), Jiangsu Province (20.7), Shanghai Municipality (18.4), Sichuan Province (22.5), and Guizhou Province (21.0). The Moran’s I statistics for average total costs, daily costs, and LOS were large and significant at 0.1% (P<0.001), indicating strong spatial correlation and clustering across PLADs.
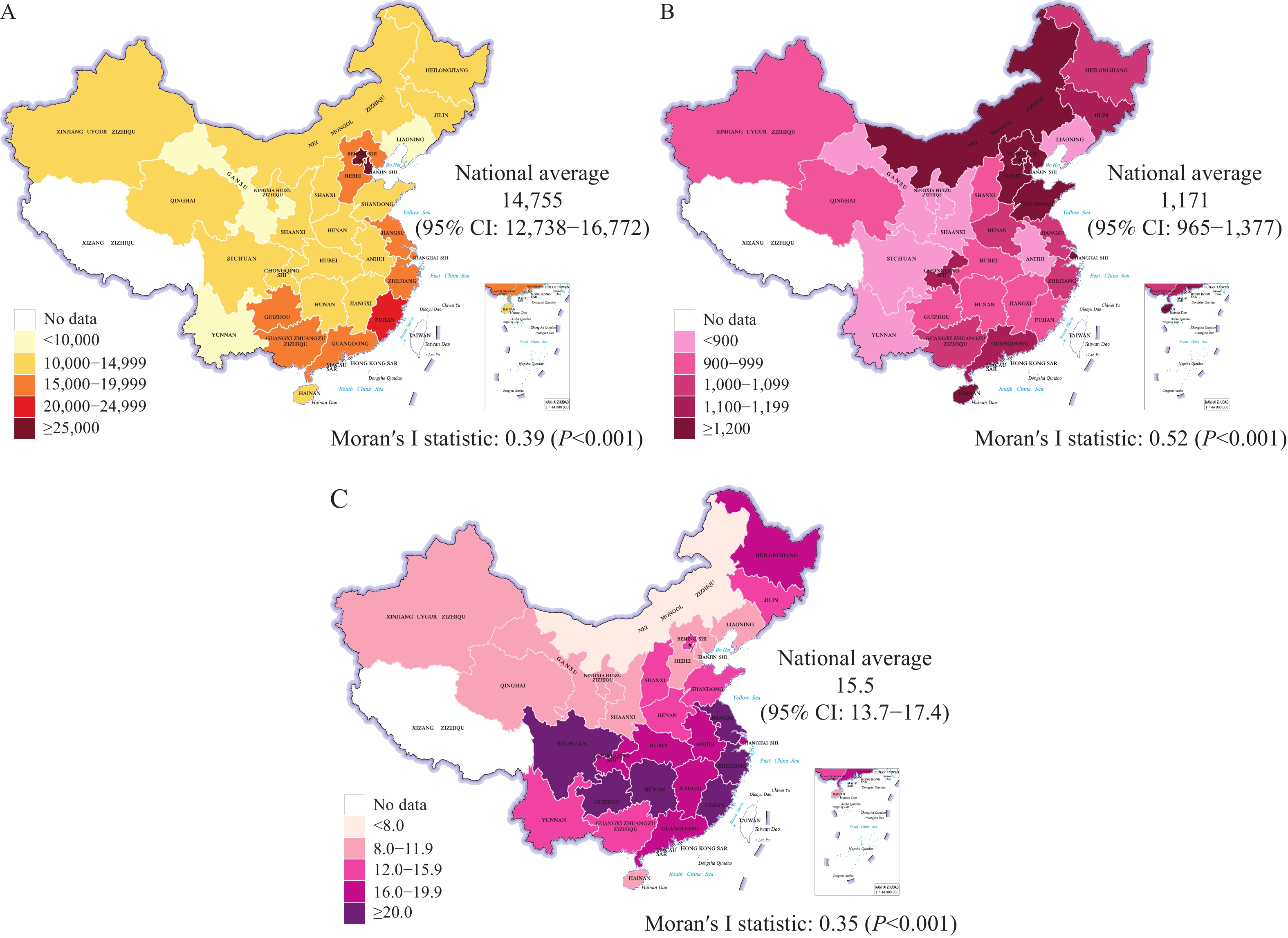 Figure 2.
Figure 2.Geographical variation in health care costs, daily costs, and length of stay for hospitalized dementia patients in China. (A) Average total inpatient cost per admission (in CNY); (B) average daily cost per admission (in CNY); (C) average length of stay per admission (in days).
Note: In each panel, the sample period was from June 2017 to June 2019; and data were available for all PLADs except for Xizang (Tibet); Taiwan, China; Hong Kong SAR; and Macau SAR. Moran’s I statistic for spatial autocorrelation was displayed at the bottom; and the national average across PLADs was displayed on the right with 95% CI presented in the parentheses. The following terms were used interchangeably: Xizang=Xizang (Tibet); Nei Mongol=Inner Mongolia; Zizhiqu=Autonomous Region.
Abbreviation: PLAD=provincial-level administrative division, SAR=Special Administrative Region, CNY=Chinese Yuan, CI=confidence interval.
-
The study demonstrated geographic variation in inpatient care utilization, disease severity/urgency, care outcomes, and costs for dementia patients in China. Several findings in the study warrant further discussion.
First, the geographical patterns of inpatient care utilization and costs overall were not entirely consistent with the patterns of disease prevalence, which may reflect the underlying disparities in dementia care and management (4). While some western PLADs with higher dementia prevalence showed greater utilization and disease burden, the patterns of other regions and PLADs differed in many other aspects. Such differences between utilization and prevalence could be partially explained by the regional variations in the proportion of older adults, economic development, healthcare infrastructure, disease awareness, and management. Varying levels of financial burden and coverage for dementia care may contribute to regional patterns (4).
Second, we showed that the regional patterns might vary across utilization measures, disease urgency/severity, outcomes, and costs, which deserves investigation in future research. For instance, while we observed greater utilization rates in western PLADs, the severity/urgency of the admissions (e.g., percentage of ER admissions) seemed to be higher in some other PLADs. Both demand and supply-side factors might explain these patterns. On the demand side, the utilization rate is mainly determined by disease prevalence and patients’ care-seeking behaviors. Many demand-side factors, such as economic difficulties, low awareness, and social stigma, may impede dementia patients from seeking care and treatment at an early stage, which will consequently lead to greater severity/urgency of the diseases and higher rates of ER admissions (1-2,4). On the supply side, inpatient care utilization largely depends on prompt access and quality of care. The varying availability of well-trained specialists and dementia care facilities across PLADs may result in the differential capacity of clinical management and control, thereby shaping the patterns of utilization, disease outcomes, and costs. Additionally, the criteria for dementia admissions may vary across areas due to the uneven distribution of dementia care resources, leading to diverse patient compositions and care outcomes (4). Our initial evidence on the geographic patterns highlights the potential differences in various aspects of dementia care. Future studies should consider this and further disentangle the underlying causes of the patterns.
Third, we found strong geographic clustering of costs, daily costs, and LOS. The costs and the care intensity were consistently higher in more developed areas, such as Jing-Jin-Ji metropolitan area and eastern coastal PLADs, which reemphasized the regional disparities in dementia care and utilization across PLADs. As the demand for healthcare and nursing is intertwined, a lack of access to primary and long-term care, especially in less developed areas, has limited the care for people with dementia and enlarged their health inequities. Demographic shifts to a greater proportion of older adults and the rising burden of dementia suggest a need to establish and strengthen primary care and long-term care systems and affordable and equitable dementia caring models (6-7).
This study was subject to some limitations. First, only hospital admissions with dementia as the primary diagnosis were included. Yet restrictions by medical technology, dementia misdiagnosis and misclassifications may affect some PLADs more than others, leading to certain levels of geographic differences. The ubiquitous underdiagnosis of dementia may also apply to our study context for all PLADs. Moreover, dementia could have been a secondary diagnosis for admission, which was not examined in this study. Second, the underlying mechanisms for the geographic variations were not fully illuminated. Data on local policies and practices needs to be linked to the medical records to understand the mechanisms of the regional patterns.
-
The authors have no conflicts of interest.
HTML
| Citation: |

|