
 Download:
Download:




-
Birth defects (BDs) are defined as structural or functional anomalies that occur before or at birth. BDs affect 6% of babies worldwide, resulting in 410,000 deaths annually (1). The prevalence of BDs in China is approximately 5.6% (2), which results in the deaths of 35,700 children younger than 5 years annually (3). However, the actual prevalence may be much higher because statistics rarely consider pregnancies terminated due to severe BDs before 28 weeks of gestation. Studies have reported that the regional prevalence of neural tube defects (NTDs) at ≥28 weeks of gestation is 66.0%–73.0% lower than that throughout pregnancy (4-5), but few have reported the total prevalence of overall BDs throughout pregnancy in China. Based on data extracted from the Birth Defects Surveillance Network, this study determined the total prevalence of BDs throughout pregnancy, depicted the epidemiological distribution of BDs in Shaanxi Province, and examined the impact of pregnancy termination before 28 weeks of gestation on the overall prevalence.
-
This study examined trends in BD prevalence using data from the hospital-based BD surveillance system, which includes 22 member hospitals in 10 districts in Shaanxi Province, from 2014 to 2020. The surveillance system collected information on livebirths or stillbirths of 28 or more complete gestational weeks, and pregnancy terminations at any gestational age occurring in member hospitals. Perinatal infants born at 28 weeks gestation to 7 days after birth, including live and stillborn infants, were subject to hospital monitoring of BDs. In addition, all terminated BDs were recorded, regardless of gestational age. All births and terminated pregnancies following a prenatal diagnosis of BD were included and coded by health professionals according to the Tenth Revision of the International Classification of Diseases (ICD-10).
This study used that data to analyze 18 frequent, major BDs in Shaanxi Province: NTDs (Q00, Q01, and Q05), hydrocephalus (Q03), anotia/microtia (Q16.0 and Q17.2), other deformities of the outer ear (Q17), Congenital Heart Defects (CHDs) (Q20 –Q26), cleft palate (CP; Q35), cleft lip with or without cleft palate (CL/P; Q36–Q37), esophageal atresia/stenosis (Q39), anorectal atresia/stenosis (Q42), hypospadias (Q54), club foot (Q66.0), polydactyly (Q69), syndactyly (Q70), limb reduction defects (LRD; Q71–Q73), congenital diaphragmatic hernia (Q79.2), omphalocele (Q79.2), gastroschisis (Q79.3), and Down syndrome (Q90).
According to the guidelines for the Chinese Birth Defects Monitoring Network, the perinatal prevalence rate was defined as the number of BD cases per 10,000 live and still perinatal births born in the range of 28 weeks gestation to 7 days after birth. The total prevalence rate (including BDs≥28 gestational weeks and BDs terminated at any gestational week) was also calculated. Any under-estimation of BDs was accounted for through the formula: under-estimated proportion equals to unreported cases divided by all cases then multiplied by 100%. This study calculated prevalence rates by calendar year, infant sex (female/male), and maternal residence area (urban/rural). Pearson chi-square tests were used to examine differences in prevalence between various groups, and linear chi-square tests were used to determine time-based trends. Two-tailed P≤0.05 was considered statistically significant. All statistical analyses were performed using SPSS (version 24.0. IBM Corp., Armonk, NY, USA). The study was approved by the Institutional Review Board of Northwest Women’s and Children’s Hospital, Shaanxi Province, China.
-
From 2014 to 2020, the system recorded 536,212 births and 12,790 cases of BDs. The prevalence of BDs at ≥28 gestational weeks and the total prevalence in Shaanxi Province have been increasing annually since 2016 (≥28 weeks: χ2trend =58.224, P<0.01; total: χ2trend =243.787, P<0.01), with a total prevalence of 318.6 per 10,000 in 2020. The prevalence would be underestimated by 40% at most, if counting only BDs at ≥28 gestational weeks (Figure 1). The annual increase in the total prevalence since 2016 includes both sexes and urban and rural areas in Shaanxi Province. The total prevalence in males was approximately 15% higher than in females each year (χ2=63.456, P<0.001). It was higher in urban areas than in rural areas each year except in 2014 (χ2=77.415, P<0.001), with a proportion of 47.2% in 2020 (Figure 2).
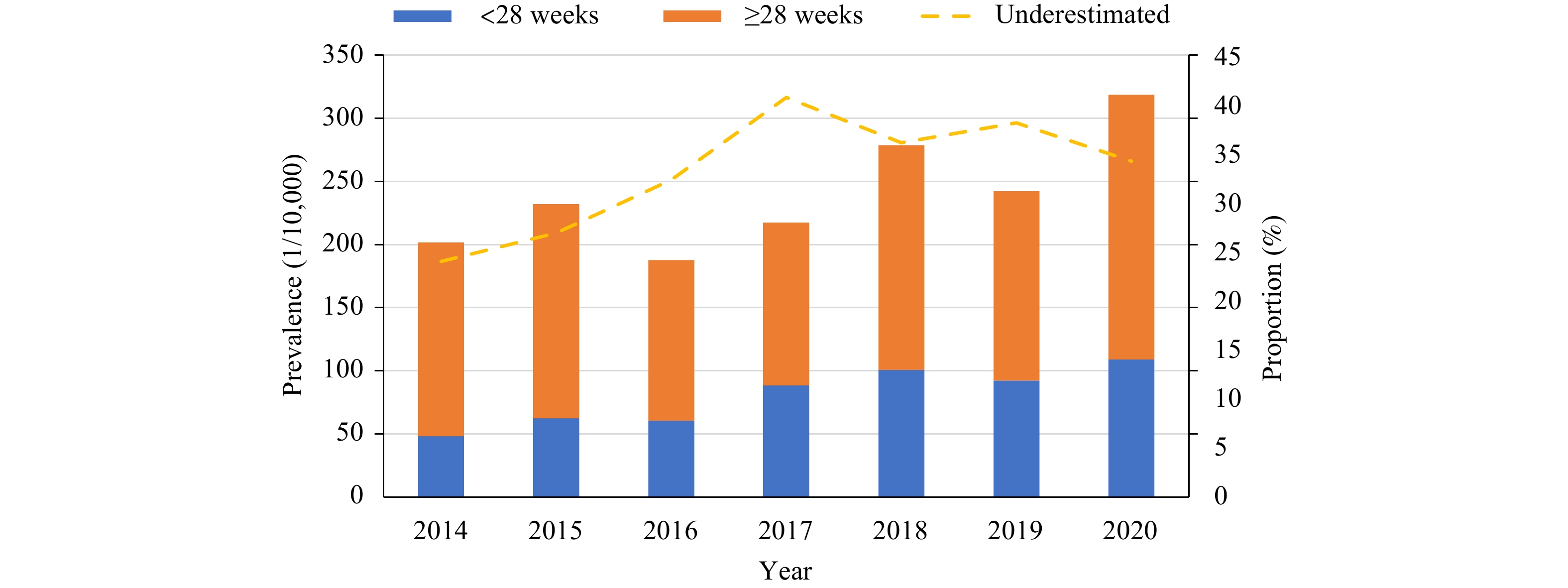 Figure 1.
Figure 1.The overall prevalence and underestimated proportion of birth defects in Shaanxi Province, 2014−2020.
Note: Perinatal prevalence (cases of 28 or more gestational weeks), the prevalence before 28 gestational weeks and under-estimated proportion of birth defects were calculated. Total prevalence (all cases regardless of gestational age) was shown as perinatal prevalence plus the prevalence before 28 gestational weeks.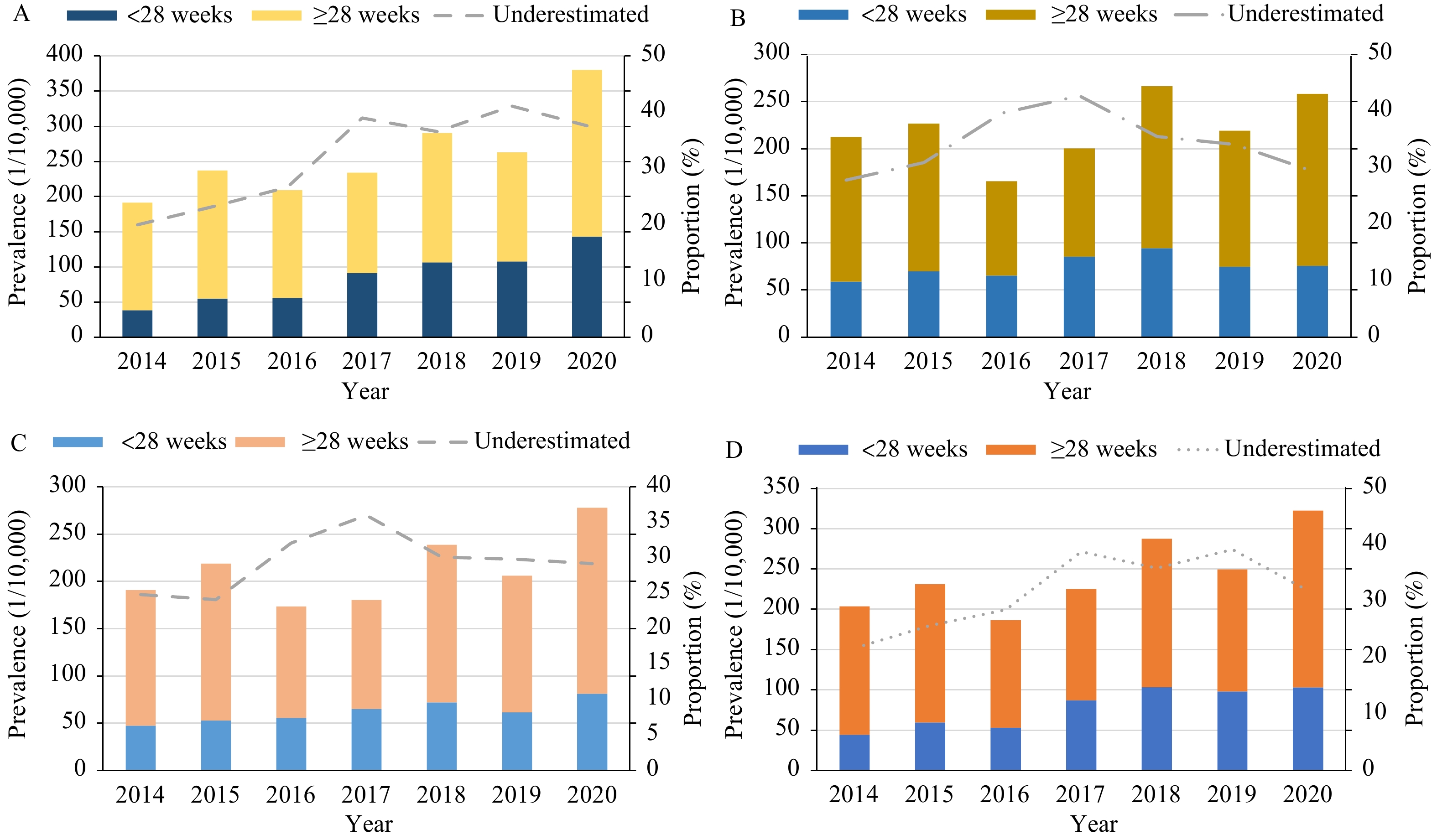 Figure 2.
Figure 2.The prevalence and underestimated proportion of BDs in (A) urban areas*, (B) rural areas†, and among (C) males§, and (D) females¶ in Shaanxi Province, 2014−2020.
Note: Perinatal prevalence (cases of 28 or more gestational weeks), the prevalence before 28 gestational weeks and under-estimated proportion of birth defects were calculated. Total prevalence (all cases regardless of gestational age) was shown as perinatal prevalence plus the prevalence before 28 gestational weeks.
Abbreviation: BD=birth defect.
* The perinatal prevalence of BDs: χ2trend=38.043, P<0.01; the total prevalence of BDs: χ2trend=249.138, P<0.01.
† The perinatal prevalence of BDs: χ2trend=21.110, P<0.01; the total prevalence of BDs: χ2trend=34.686, P<0.01.
§ The perinatal prevalence of BDs: χ2trend=31.520, P<0.01; the total prevalence of BDs: χ2trend=143.089, P<0.01.
¶ The perinatal prevalence of BDs: χ2trend=26.059, P<0.01; the total prevalence of BDs: χ2trend=56.366, P=0.01.
From 2014 to 2020, the prevalence of all major types of BD were underestimated by 10% to 100%−particularly severe external BDs such as NTDs, total cleft lip, Down syndrome, congenital hydrocephalus, and limb shortening (Table 1). In recent years, the rates of such severe defects after 28 weeks of gestation have declined steadily: not even reaching the top 10 in 2020. However, these still rank high when taking into account those terminated before 28 weeks of gestation. The top five BDs with the highest total prevalence in 2020 were CHD (155.0 per 10,000), cleft lip with or without palate (20.0 per 10,000), polydactyly (19.7 per 10,000), Down syndrome (12.2 per 10,000), and NTDs (11.6 per 10,000) in 2020. The overall prevalence of CHD increased significantly in 2020, and was about 50% higher than that in 2019 (Table 2).
Item 2014 2015 2016 2017 2018 2019 2020 ≥28 weeks Total Under-
estimated
(%)≥28 weeks Total Under-
estimated
(%)≥28 weeks Total Under-
estimated
(%)≥28 weeks Total Under-
estimated
(%)≥28 weeks Total Under-
estimated
(%)≥28 weeks Total Under-
estimated
(%)≥28 weeks Total Under-
estimated
(%)NTDs 5.4 16.0 66.2 3.4 12.0 71.6 2.5 12.8 80.4 2.2 12.6 82.5 1.0 11.8 91.5 0.9 6.8 86.8 1.7 11.6 85.4 Hydrocephalus 7.5 13.3 43.6 4.8 10.4 54.0 4.8 8.0 39.8 4.2 8.3 49.3 3.4 6.6 48.3 2.5 4.6 45.1 3.3 6.7 50.4 Cleft palate 1.0 1.3 21.5 2.2 2.6 14.3 2.5 3.0 15.6 2.2 2.6 14.1 2.7 3.0 11.1 2.3 2.3 −1.0 3.0 3.8 21.6 Cleft lip with or without palate 6.7 14.3 53.1 6.2 16.4 62.3 5.4 16.1 66.4 4.9 21.5 77.2 5.4 22.7 76.2 3.4 17.8 80.9 3.3 20.0 83.5 Anotia/microtia 2.0 2.0 −0.9 1 1.5 35.1 0.7 0.7 −2.4 1.6 1.7 6.3 1.0 1.3 21.0 1.5 1.7 12.2 1.1 1.4 22.3 Other deformities of the outer ear 2.4 2.4 0.3 4.5 4.6 2.6 4.1 4.1 0.1 2.6 2.6 −1.5 2.5 2.7 5.9 3.5 3.8 6.9 5.4 5.5 2.3 Esophagus atresia/stenosis 1.8 2.3 20.5 1.2 1.5 22.1 2.1 2.3 7.9 0.7 1.1 36.2 0.6 0.9 32.3 1.0 1.3 20.2 1.8 2.0 9.2 Anorectal atresia/stenosis 2.0 2.4 16.9 1.9 2.2 14.6 2.3 2.5 8.3 2.0 2.2 8.9 3.2 3.2 −1.1 1.8 2.4 24.7 2.1 2.7 22.0 Hypospadias 2.6 2.7 3.3 3.8 3.8 −0.9 4.0 4.1 2.5 6.2 6.2 0.3 5.8 6.1 4.5 4.2 4.6 7.8 5.2 5.2 0.8 Club foot 2.7 4.2 36.4 3.1 6.5 52.3 1.8 4.8 62.4 1.6 4.0 60.2 1.8 4.3 58.2 3.0 5.4 43.9 2.0 4.4 54.5 Polydactyly 13.6 13.9 2.0 15.4 15.6 1.2 14.4 14.9 3.6 13.5 14.3 5.4 16.5 17.2 4.4 13.6 15.0 9.9 18.8 19.7 4.3 Syndactyly 4.1 4.1 0.1 2.9 3.3 10.8 4.3 4.6 5.7 5.5 5.6 1.9 6.0 6.5 7.8 6.4 7.3 12.5 7.1 7.4 3.9 Limb reduction defects 2.0 3.4 41.1 2.6 4.1 36.7 1.6 3.6 56.1 1.2 5.1 76.6 1.0 4.3 76.8 1.0 3.8 73.4 1.7 4.7 63.6 Congenital diaphragmatic hernia 1.7 3.0 42.8 1.4 3.3 57.0 1.0 1.9 48.4 0.6 1.5 59.0 0.9 2.4 62.6 1.5 3.3 54.6 0.9 2.5 64.7 Omphalocele 0.1 0.4 76.5 0 1.2 100.0 0.6 1.5 59.5 1.0 2.7 62.7 0.6 3.3 80.9 1.0 3.6 72.6 0.3 4.5 93.4 Gastroschisis 0.9 2.1 57.6 0 3.1 100.0 0.1 1.3 92.0 0.4 2.0 79.5 0.3 1.0 75.3 0.0 0.7 100.0 0.3 2.1 85.9 Down syndrome 1.7 3.5 52.0 1.7 5.3 68.0 1.4 6.7 79.2 1.3 12.6 89.6 1.7 12.8 86.7 1.7 11.6 85.4 0.9 12.2 92.6 CHDs 82.3 92.7 11.3 97.2 112.8 13.8 54.8 68.7 20.3 64.8 82.4 21.4 108.5 137.2 20.9 79.6 104.8 24.0 128.1 155.0 17.3 Note: Perinatal prevalence (the number of cases of 28 or more gestational weeks per 10,000 births), total prevalence (the number of cases regardless of gestational age per 10,000 births) and underestimated proportion (cases before 28 gestational weeks accounting for all cases) of birth defects were calculated.
Abbreviation: BD=birth defect; NTDs=neural tube defects; CHDs=congenital heart defects.Table 1. Underestimated status of the main BDs in Shaanxi Province, 2014–2020.
Rank Perinatal prevalence (1/10,000) Total prevalence (1/10,000) 2014 2015 2016 2017 2018 2019 2020 2014 2015 2016 2017 2018 2019 2020 1 CHDs (82.3) CHDs (97.2) CHDs (54.8) CHDs (64.8) CHDs (108.5) CHDs (79.6) CHDs (128.1) CHDs (92.8) CHDs (112.8) CHDs (68.7) CHDs (82.5) CHDs (137.2) CHDs (104.8) CHDs (155.0) 2 Polydactyly (13.6) Polydactyly (15.4) Polydactyly (14.4) Polydactyly (13.5) Polydactyly (16.5) Polydactyly (13.6) Polydactyly (18.8) NTDs (16.0) Cleft lip with or without palate (16.4) Cleft lip with or without palate (16.1) Cleft lip with or without palate (21.5) Cleft lip with or without palate (22.6) Cleft lip with or without palate (17.7) Cleft lip with or without palate (20.0) 3 Hydrocephalus (7.5) Cleft lip with or without palate (6.2) Cleft lip with or without palate (5.4) Hypospadias (6.2) Syndactyly (6.0) Syndactyly (6.4) Syndactyly (7.1) Cleft lip with or without palate (14.3) Polydactyly (15.6) Polydactyly (14.9) Polydactyly (14.3) Polydactyly (17.3) Polydactyly (15.1) Polydactyly (19.7) 4 Cleft lip with or without palate (6.7) Hydrocephalus (4.8) Hydrocephalus (4.8) Syndactyly (5.5) Hypospadias (5.8) Hypospadias (4.2) Other deformities of the outer ear (5.4) Polydactyly (13.9) NTDs (12.0) NTDs (12.8) NTDs (12.6) Down syndrome (12.8) Down syndrome (11.6) Down syndrome (12.2) 5 NTDs (5.4) Other deformities of the outer ear (4.5) Syndactyly (4.3) Cleft lip with or without palate (4.9) Cleft lip with or without palate (5.4) Other deformities of the outer ear (3.5) Hypospadias (5.2) Hydrocephalus (13.3) Hydrocephalus (10.4) Hydrocephalus (8.0) Down syndrome (12.6) NTDs (11.8) Syndactyly (7.3) NTDs (11.6) 6 Syndactyly (4.1) Hypospadias (3.8) Other deformities of the outer ear (4.1) Hydrocephalus (4.2) Hydrocephalus (3.4) Cleft lip with or without palate (3.4) Cleft lip with or without palate (3.3) Club foot (4.2) Club foot (6.5) Down syndrome (6.7) Hydrocephalus (8.3) Hydrocephalus (6.6) NTDs (6.8) Syndactyly (7.4) 7 Club foot (2.7) NTDs (3.4) Hypospadias (4.0) Other deformities of the outer ear (2.6) Anorectal atresia
stenosis (3.2)Club foot (3.0) Cleft palate (3.0) Syndactyly (4.1) Down syndrome (5.3) Club foot (4.8) Hypospadias (6.2) Syndactyly (6.5) Club foot (5.4) Hydrocephalus (6.7) 8 Hypospadias (2.6) Club foot (3.1) NTDs (2.5) NTDs (2.2) Cleft palate (2.7) Hydrocephalus (2.5) Anorectal atresia/
stenosis (2.1)Down syndrome (3.5) Other deformities of the outer ear (4.6) Syndactyly (4.6) Syndactyly (5.6) Hypospadias (6.1) Hydrocephalus (4.6) Other deformities of the outer ear (5.5) 9 Other deformities of the outer ear (2.4) Syndactyly (2.9) Anorectal atresia/
stenosis (2.3)Anorectal atresia/
stenosis (2.0)Other deformities of the outer ear (2.5) Cleft palate (2.3) Club foot (2.0) limb reduction defects (3.4) limb reduction defects (4.1) Other deformities of the outer ear (4.1) limb reduction defects (5.1) Club foot (4.3) Hypospadias (4.6) Hypospadias (5.2) 10 Anorectal atresia/
stenosis (2.0)Limb reduction defects (2.6) Esophagus atresia/
stenosis (2.1)Club foot (1.6) Club foot (1.8) Anorectal atresia/
stenosis (1.8)Esophagus atresia/
stenosis (1.8)Congenital diaphragmatic hernia (3.0) Hypospadias (3.8) Hypospadias (4.1) Club foot (4.0) limb reduction defects (4.3) Other deformities of the outer ear (3.8) Limb reduction defects (4.7) Note: Perinatal prevalence (cases of 28 or more gestational weeks), total prevalence (all cases regardless of gestational age) and underestimated proportion (cases before 28 gestational weeks accounting for all cases) of birth defects were calculated.
Abbreviation: BD=birth defect; NTDs=neural tube defects; CHDs=congenital heart defects.Table 2. The ranking for top 10 most common BDs in Shaanxi Province, 2014–2020.
-
BDs are increasing worldwide due to an increase in known risk factors, such as maternal diabetes and obesity, as well as emerging threats, such as the Zika epidemic (6). The total prevalence of BDs in Shaanxi Province from 2014 to 2020 trended upward, similar to the global trend. In recent years, with improvements in prenatal screening, diagnostic technology, and ultrasound technology, external BDs are more likely to be detected than ever before. In addition, the detection rate of congenital heart diseases, especially micromalformation, has greatly increased, which is one reason for the increase in the incidence of BDs. In most years, the prevalence has been higher in males and in urban areas. These results are consistent with studies in other areas of China, such as Shanxi Province and Ningxia Hui Autonomous Region (7-8). Compared to many developed countries (9), the prevalence of BDs in Shaanxi Province is lower, mainly because BD monitoring usually begins from 20–22 weeks in Western countries as opposed to after 28 weeks in China. Many domestic studies have reported the prevalence of BDs after 28 weeks of gestation, while few have reported the total prevalence including those before 28 weeks. Excluding BDs before 28 weeks likely significantly underestimates the prevalence of BDs in China. The World Health Organization (WHO) proposes that countries may determine the feasibility of earlier gestation monitoring according to the capacity to ascertain cases prior to 28 weeks’ gestation (10). With the development of capacity of ascertaining BDs, such as due to aforementioned technological advances, the beginning week of BD surveillance ought to be earlier than 28 gestation weeks in China. The inclusion of BDs before 28 weeks of gestation in order to obtain the true incidence of BDs could provide a basis for assessing the true effect of primary prevention measures and encourage health authorities at all levels to pay attention to the better implementation of primary prevention measures in the future.
The incidence of several severe BDs that are monitored in Shaanxi Province, such as NTDs, limb shortening, omphalocele, gastroschisis, and Down syndrome, has been underestimated by 40%–90%. A few domestic studies have reported an underestimation of NTDs and cleft lip and palate in local areas. For example, in one study, the incidence of NTDs was underestimated by 62.2% and that of cleft lip was underestimated by 12.6% in Shanxi Province (5). A study in the Tongzhou District of Beijing showed that, if BD surveillance began at 13 weeks of gestation, the number of reported NTDs cases would increase by about 2.7 times (4). In this study, the incidence of NTDs monitored in Shaanxi Province was underestimated by 80.1%, while the incidence of cleft lip and palate was underestimated by 78.5%. The underestimation of other major defects has not been reported in China. To the best of authorial knowledge, this study is the first to describe the underestimation of all major BDs systematically.
The top 10 most frequent BDs in Shaanxi Province are the same as those in China overall when those before 28 weeks of gestation are not included (11). However, their ranking changed significantly when considering both those before and after 28 weeks of gestation. The top five BDs are similar, particularly NTDs and cleft palate. In addition to preventing NTDs, periconceptional supplementation with folic acid appears to prevent CHD and oral clefts (12). Good adherence to folic acid supplementation may reduce the prevalence of NTDs to 6/10,000 or lower, according to a bayesian model (13). However, a large-scale cross-sectional study showed that less than 10% of pregnant women in northwest China take folic acid effectively for more than 3 months (14). Based on the higher prevalence of NTDs, cleft palate, and CHD, interventions for effective folic acid administration should continue to be strengthened in Shaanxi Province.
CHD is the most prevalent BD and its rate increased dramatically from 2014 to 2020, both after 28 weeks of gestation and overall. The causes of CHD are complicated and their etiology is not clear. Some studies have shown that advanced maternal age (AMA) increases risk for aneuploidy, which is associated with an overall increased risk for major anomalies including CHD (15). The dramatic increase in the proportion of women with AMA may be an important reason for the rapidly increasing prevalence of CHD, with the enactment of a universal two-child policy. In addition, the incidence of CHD increased significantly in Shaanxi Province in 2020, which was attributed to changes in the diagnostic standards and the inclusion of micro-lesions in CHD. Note that the increasing number of women with AMA following a three-child policy might continue to contribute to the increasing prevalence of CHD.
This study had at least two limitations. First, as the underestimated proportion of BDs was calculated from provincial data, the results are not generalizable to the entire country. Second, because some congenital metabolic diseases and functional abnormalities may not be identified in infancy, the prevalence of BDs might still be underestimated. Nevertheless, considering the large sample size, the results depict the epidemiological characteristics of most structural malformations in Shaanxi Province.
-
No conflicts of interest.
-
We appreciate the contributions of all workers at 22 member hospitals in 10 districts in Shaanxi Province.
HTML
| Citation: |

|