
 Download:
Download:




-
The prevalence of food allergy (FA) is rising rapidly worldwide; it has become a major health burden in many jurisdictions, especially in children, but little is known about its prevalence in Jiangxi Province in China. Thus, this survey aimed to estimate the FA prevalence in school children across Nanchang City, Jiangxi Province. A cross-sectional survey on FA was performed using a standardized questionnaire of FA among school children in Nanchang in 2021. Children whose parents or legal guardians reported the children had or have FA were considered FA individuals. FA accounted for 67.3% of adverse reaction to food (ARF) and the prevalence of FA was 4.9%. The main foods triggering allergies were shrimp and mango: while severe food allergic reactions accounted for 26.0% of those reported. The prevalence of other allergic diseases was significantly higher in children with existing FA than in children without FA. Further epidemiological studies on FA in Jiangxi are warranted; and preventive strategies such as a comprehensive FA labeling system should be developed and implemented in line with the findings of epidemiological studies. In addition, preventive practices such as public awareness campaigns about FA should be conducted to increase people’s awareness of FA and assist them in recognizing the signs and symptoms of allergic reactions, especially among high-risk groups. A subset of susceptible individuals could have life-threatening FA anaphylactic reactions and, in many cases, may require urgent medical attention.
Geographical variability in the prevalence, the major allergenic food triggers, and the clinical presentation of FA — as well as differences in symptoms and clinical phenotypes due to race, ethnicity, age, and concomitant allergic disease — suggest that gene-environment interaction may play an important role in the development and presentation of FA (1-2). FA affects about 2 children in an average-sized classroom of 25 children; about 30.0% of allergic reactions occurred in children who were not previously known to have had FA (3). Moderate and severe reactions co-occur frequently: 42.3% of food-allergic children reported ≥1 severe FA (4). Living with FA is well recognized to impair one’s quality of life in childhood, parenthood, and adulthood (5) and has also been implicated in increasing pediatric asthma morbidity and life-threatening exacerbations (6). FA is becoming a major health burden in many countries, especially in children (7). To fill the gap in the epidemiological study on FA among children in Jiangxi Province and obtain a list of allergenic foods, this survey on FA was conducted in school children in Nanchang, Jiangxi Province in 2021.
Xinjian District was selected randomly from the six districts in Nanchang. All schools in the district were numbered, and five schools were selected randomly by computer; a representative sample of 6–11-year-old children was selected from the 5 elementary schools.
Ethical approval was obtained from the ethical committee of the China National Center for Food Safety Risk Assessment and written informed consent was obtained from the children’s legal guardians.
The survey was mainly based on the EuroPrevall FA screening questionnaire, and included demographic variables, ARF, FA, and other allergic diseases, etc. The questionnaires were distributed to the recruited children in school and completed at home by their parents or other guardians. Upon completion, they were collected and checked by teachers and investigators. Based on the response to the question of whether your child has/had a FA, if one reported “yes” to it, they were defined as a FA individual.
Data were double entered using EpiData (version 3.1, EpiData Association, Odense, Denmark) and statistical analysis was performed using SPSS (version 25.0, IBM Corp., NY, USA). Percentage rate was used to express the count data, and mean±standard deviation was used to describe the continuous data. Body mass index (BMI) was graded by the Chinese BMI grading standard. The chi-square (χ2) test and t test were used to evaluate the significance of the data: P<0.05 was considered a statistically significant difference.
A total of 3,003 questionnaires were distributed to the 5 selected schools. Ultimately, 2,997 valid questionnaires were collected with a valid response rate of 99.8%. There were 1,512 males and 1,485 female, 1,475 rural children and 1,522 urban children among the participants. Their mean age was 8.40±1.23 years, and mean family size was 5.28±1.41. The reported prevalence of FA was 4.9%. 3.9% of the participants did not know if they had FA; differences in reported FA prevalence were not significant for gender, age, or BMI, as shown in Table 1. Doctor-diagnosed FA prevalence was 3.0%, and the major method of FA diagnosis used by doctors was the serum special immunoglobulin E (sIgE) test (35.6%) with oral food challenge (OFC) and skin prick test (SPT): 16.7% and 10%, respectively.
Variable FA (n=146) No FA (n=2,734) χ2/t P FA (%) Total (N=2,997) Age (Mean±SD) 8.41±1.26 8.42±1.23 −0.990 0.921 4.9 8.40±1.23 Gender 0.093 0.760 Male 75 1,369 5.0 1,512 Female 71 1,365 4.8 1,485 Residence 1.966 0.161 Rural 81 1,354 5.5 1,475 Urban 65 1,380 4.3 1,522 Ethnic 0.000 1.000 Han 146 2,732 4.9 2,994 Others 0 2 0 3 BMI 2.587 0.274 Thin 25 365 6.1 407 Normal 85 1,758 4.5 1,908 Overweight and obesity 36 611 5.3 682 Family size (Mean±SD) 5.29±1.34 5.29±1.41 −0.026 0.979 4.9 5.28±1.41 Abbreviation: FA=food allergy; BMI=body mass index; SD=standard deviation. Table 1. Demographic characteristics and prevalence of food allergy among the school children in Nanchang, Jiangxi, China in 2021.
Shrimp (28.1%), mango (22.6%), and shellfish (18.5%) were the top 3 allergenic foods, while peanut was No. 8 on the list of allergenic foods with a reported rate of 5.3%. Among the 8 major allergenic foods, mango and beef were not included in the 8 categories of allergenic substances in the China National Food Labeling Standard (GB 7718-2011), as shown in Table 2. The main manifestations of FA were skin symptoms such as rash or itching (63.0%), severe allergic reactions (8) accounted for 26.0%. Figure 1 describes the main food allergic symptoms.
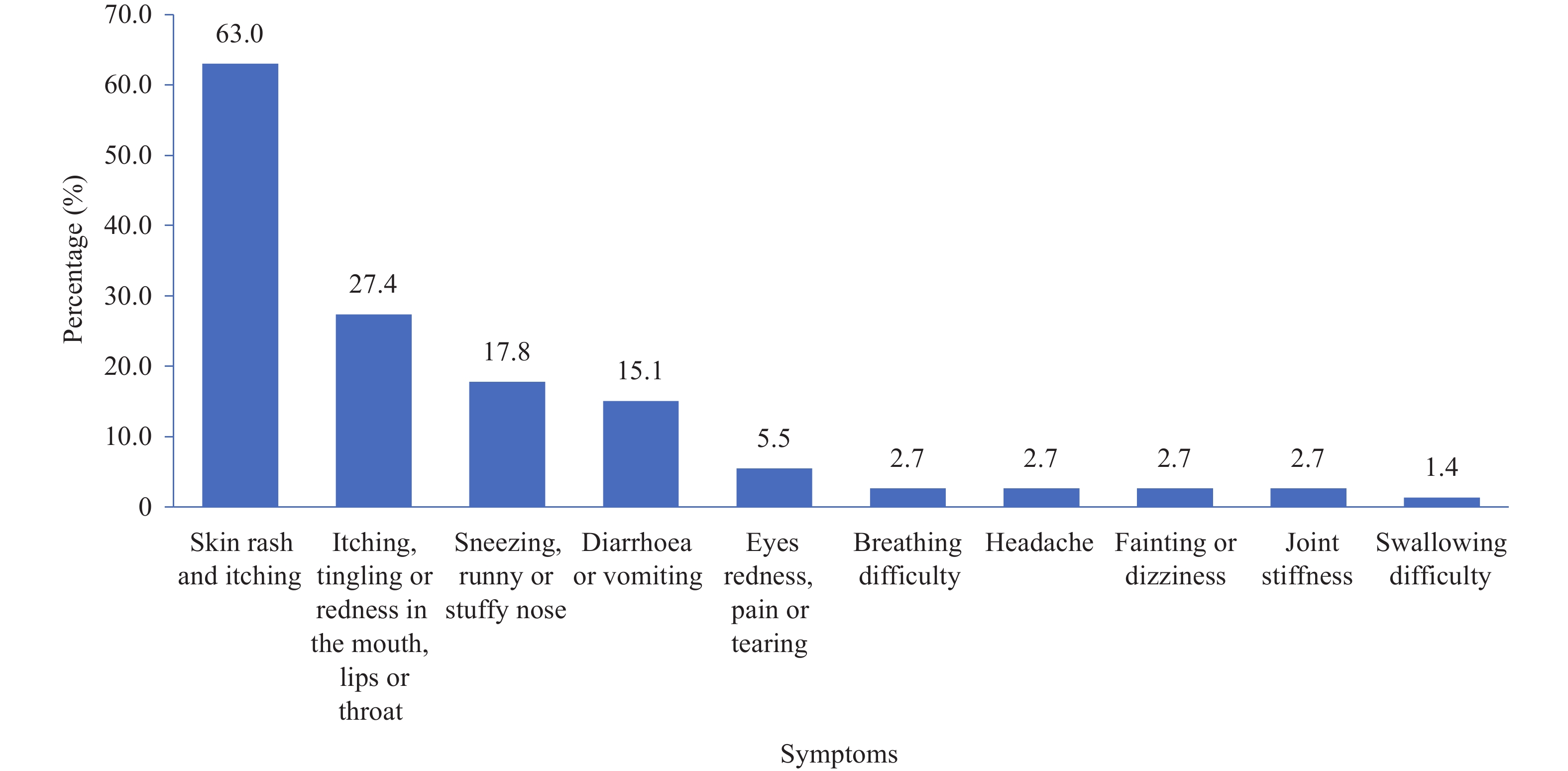 Figure 1.
Figure 1.Major symptoms of food allergy among the school children in Nanchang City, Jiangxi Province, China in 2021.
Note: The most common manifestations of FA in the children were skin symptoms such as rash or itching with 63.0% proportion, followed by itchy tingling or redness in the mouth, lips, throat, sneezing, runny or stuffy nose, diarrhea or vomiting, etc.Allergenic foods N (%) Rural Urban Included in GB 7718-2011 Shrimp 41 (28.1%) 24 (29.6%) 17 (26.2%) Yes Mango 33 (22.6%) 15 (18.5%) 18 (27.7%) No Shellfish 27 (18.5%) 14 (17.3%) 13 (20.0%) Yes Egg 19 (13.0%) 11 (13.6%) 8 (12.3%) Yes Milk 15 (10.3%) 8 (9.9%) 7 (10.8%) Yes Fish 7 (4.8%) 2 (2.5%) 5 (7.7%) Yes Beef 7 (4.8%) 3 (3.7%) 4 (6.2%) No Peanuts 7 (4.8%) 4 (4.9%) 3 (4.6%) Yes Nuts 5 (3.4%) 3 (3.7%) 2 (3.1%) Yes Soybeans 4 (2.7%) 2 (2.5%) 2 (3.1%) Yes Mutton 3 (2.1%) 0 (0.0%) 3 (4.6%) No Total 146 (100.0%) 81 (100%) 65 (100%) - Table 2. Common allergenic foods among the school children in Nanchang, Jiangxi, China in 2021.
The prevalence of atopic dermatitis, allergic rhinitis, and allergic asthma was 2.5%, 3.3% and 0.4%, respectively. All of these were lower than FA prevalence in school children. The distribution of other allergic diseases was significantly higher in the FA group than that in the non-FA group.
Supplementary Table S1 describes the prevalence of other allergic diseases. -
This is the first population-based survey that attempts to estimate reported FA (by parents/guardians) prevalence among school children in Nanchang, Jiangxi, China. The results showed the prevalence of reported FA among school children in Nanchang to be 4.9%: higher than the 1.8% reported in India, and lower than the 38% reported in Russia, 15% reported in Guangzhou, and 13% reported in Hong Kong (8). These differences in FA prevalence are probably due to differences in dietary exposures, early-life environment, and socioeconomic factors.
Allergenic foods vary in different countries or regions. Although the consumption of peanuts and peanut products is widespread in China, there have been fewer reports of peanut allergies; however, peanut allergy is the most common FA in the U.S. and Europe (4,9). This may reflect the differences that genetic background makes in susceptibility to the same food across different countries and races. In addition, mango was one of the primary reported allergenic foods in this study; however, it is not included in the Chinese GB 7718-2011, which was developed with reference to the International Codex Alimentarius Commission standards. This study suggests that key allergens differ between geographical jurisdictions and that standards should be specific to the Chinese population.
The common symptoms of FA reported in this study were skin and oral mucosal symptoms. However, a survey in 8 European countries showed the most common symptoms to be rash or gastrointestinal symptoms in children with FA (9). The variance of allergenic foods may cause differences in common FA symptoms; for example, the main allergenic foods are milk and eggs in European countries, which are different from the shrimp and mango primary allergens found in this survey. Previous studies have reported that FA was the first step of “allergy march”, and could increase the risk of other allergic diseases (10). Furthermore, this survey showed that the prevalence of other allergic diseases was significantly higher in the FA group than in the non-FA group.
Avoiding allergenic foods through diet and management of acute allergic reactions with antihistamines or epinephrine is the current standard of care for those diagnosed with FA (4). Managing FA in school children requires cooperation amongst school administrators, teachers, and families. Resources for managing FA should be provided to parents, school administrators, and teachers, and they should be offered information about planning and implementing strategies for preventing and reducing allergic reactions and treating life-threatening FA reactions (11).
Further epidemiological studies on FA should be conducted in Jiangxi; prevention strategies such as comprehensive relevant food allergen labeling systems should be developed according to the epidemic characteristics of prevalent food allergens; public awareness campaigns to increase FA knowledge should be conducted to assist people in recognizing the signs and symptoms of allergic reactions, especially among high-risk groups. Early detection and comprehensive prevention and control are important to reduce the health risks associated with FA in the population.
One potential limitation of this study is that using parent/guardian reported FA without objective indicators may not accurately estimate FA prevalence; Another disadvantage is that the selected school children only came from five primary schools, which may not be representative of all school children aged 6–11 years in Nanchang. However, preliminary results need to be confirmed in further studies with accurate diagnosis of FAs to confirm the reported epidemiological findings. The high response rate and strict quality control in this survey suggest the results reflect a problem among school children in Nanchang worthy of further investigation.
Increased doctor-diagnosed FA prevalence and tests to confirm FA such as SPT and sIgE test are ongoing. The next step will be to use DBPCFC to confirm suspected FA.
This study contributes to improving awareness of FA, filling in the gap in the epidemiological data on FA in school children. It also presents scientific evidence for updating the list of food allergens for China and developing policies for FA prevention and management in Jiangxi and other regions.
-
No conflicts of interest.
-
Staff in the Xinjian District CDC in Nanchang City; Teachers involved in this survey; Students participating in this survey; Professor Yuanan Lu in the School of Public Health, Hawaii University.
-
Other allergic diseases FA, n (%) No FA, n (%) χ2 P Allergic dermatitis 30 (20.5%) 37 (1.4%) 224.729 0.000 Allergic rhinitis 22 (15.1%) 65 (2.4%) 76.199 0.000 Allergic asthma 3 ( 2.1%) 6 (0.2%) 9.674 0.002 Else 6 ( 4.1%) 17 (0.6%) 21.282 0.000 Total 61 (41.8%) 125 (4.6%) 317.632 0.000 Abbreviation: FA=food allergy. Table S1. Other allergic diseases prevalence and distribution among the school children with food allergy in Nanchang, Jiangxi, China in 2021.
HTML
| Citation: |

|