

 Download:
Download:




-
Adverse reactions to food (ARF) are a major, worldwide public health and food safety problem. Among the various causes of ARF, food allergies (FA) are particularly serious as the immune response that is triggered can be fatal even at very low doses. FA usually occur as an adverse immune response arising from exposure to a specific given food; it is often the first clinical allergy appearance and the first link in the so-called “march of atopy” (1), representing one of the most common causes of anaphylaxis (2). Previous studies have shown that FA generally affects about 5% of adults and 8% of children — and can even manifest in up to 10% of children in high-income countries (3-5). The prevalence of FA has risen in the past 10 years (6); the types of foods causing allergies and serious allergic reactions are growing. FA can cause many physical and psychological disorders. It is a very serious problem, not only for patients and their families, but also for medical staff and local communities. Today, FA has become a well-recognized, major public health and food safety issue of global concern (7).
Due to allergenic agents being extremely heterogeneous in eliciting allergens, symptoms, and clinical signs (8), validly assessing FA has been difficult. Many studies on FA have used outpatients as subjects to investigate the clinical aspects of FA. However, only a fraction of the individuals who actually experience a food allergy visit a medical doctor. Therefore, it is presently unclear how representative these results are of the general population (9).
Very little is known regarding global variations in the prevalence of food allergies. Data about FA in most low- and middle-income countries are quite scarce (4). Limited, small-scale research shows that the confirmed FA prevalence is about 6% among children in China, which also demonstrates an upward trend consistent with the upward trend in global prevalence (10).
Food allergen labelling of the “Big-8” recommended by the Codex Alimentarius Commission (gluten, crustaceans, eggs, fish, milk, peanuts, soybeans, and tree nuts) (11) lacks support from Chinese epidemiologic data on FA, as their prevalence is poorly defined in the Chinese population. Epidemiologic studies on FA confirmed with double-blind placebo-controlled food challenges (DBPCFC) in the general population are thus necessary to be conducted in China.
This study aims to assess the unknown, epidemiological feature of ARF and FA in China. The results will form the baseline dataset for monitoring the trend of FA, provide support for updating the allergenic food labelling list in China, estimate the thresholds for food allergens where feasible, present scientific evidence for effective control measures, and inform policies for FA prevention and diagnosis.
-
Eight provincial-level administrative divisions (PLADs) were selected as study centers by random cluster sampling in China; three prefectures were selected randomly from each selected PLAD, then one county/district was selected from each prefecture as a sub-survey center.
Children were recruited from primary schools in both rural and urban regions, of which 4–6 schools generated by computer randomization were obtained for each sub-survey center. In these schools, children aged 6–11 years old were recruited from grades 1–5. For adults, towns or street districts were ranked according to their population size; 2 townships and 2 street districts were randomly selected in each sub-survey center, with adults aged 18–70 randomly recruited. Exclusion criteria of participants included: age outside of the aforementioned ranges; difficulty in completing the survey due to severe disease; and respondents or their parents (guardians) not providing consent.
-
Sample size estimation was mainly based on the case-control study: assuming the case-control study had 90% power to find an odds ratio of 2; 15% population were exposed to the risk factors (12). One control per case (e.g., 240 cases and 240 controls) was used. Given a 20% non-response rate in the case-control study, 5% and 3% prevalence rates of IgE-mediated FA were estimated in primary schoolchildren and adults, respectively. In total, 9,000 children and 12,000 adults for FA screening in each study center were estimated to be sufficient, i.e., 3,000 children and 4,000 adults for each sub-survey center. Each subject was coded uniformly, concealing his/her residence and personal information. Data were collected from 2020, and this research is expected to continue to be completed in the following ten years.
-
Modifications based on the habits and characteristics of the Chinese population were made to the translated EuroPrevall FA questionnaires before this methodology was applied. The questionnaires focused on demographic characteristics and adverse reactions to food: including food allergies, risk factors, and exposures.
-
This study mainly focused on IgE-mediated allergies to 20 priority foods (cow’s milk, hen’s eggs, fish, shrimp, crab, shellfish, beef, peanuts, sesame, soy, wheat, buckwheat, rice, peaches, oranges, mangos, hazelnuts, walnuts, almonds, and cashews) reported to commonly cause FA reactions and frequently consumed in China. The epidemiologic study consisted of three main consecutive stages.
In Stage I, subjects were screened using an FA questionnaire that focused on demography, ARF, causative foods, diagnosis methods of FA and other allergic diseases. For children, the screening questionnaires were completed by their parents or legal guardians; adults completed screening questionnaires themselves.
In Stage II, subjects who reported ARF symptoms to 1 of the 20 priority foods were regarded as cases (suspected FA); those who had “no reaction” to foods reported in Stage I were randomly matched to suspected FA cases with similar demographics as controls. All cases and controls were invited to the local hospital for clinical evaluation of FA, which involves skin prick testing (SPT), collection of serum for IgE testing, and clinical interviews. The face-to-face interviews were conducted by well-trained clinicians with detailed questionnaires that focused on socio-demographics, FA, living environments, lifestyle behaviors, and presence of any family history of allergy. SPT was performed with 20 food allergens, along with negative and positive controls, standardized allergen extracts, and control solutions obtained from GREER (Madrid, German). Valid controls and largest wheal diameter ≥3 mm were regarded as positive. All serum samples were sent to the laboratory of Peking Union Medical College Hospital to test for total IgE and specific IgE (sIgE) using the commercially available ImmunoCAP 250 (Phadia, Uppsala, Sweden): this study followed the manufacturer’s instructions, whereby an sIgE value of ≥0.35 kUA/L is considered positive (9).
In Stage III, an individual with probable FA who self-reported an ARF (Stage I and/or Stage II) and matched food sensitization (positive SPT or sIgE) (12) to one of 9 priority foods (milk, eggs, fish, shrimp, peanuts, hazelnuts, peaches, mangos, or apples) was scheduled for a comprehensive clinical evaluation, including DBPCFC (13). Subjects with a history of anaphylactic food reactions were excluded. DBPCFC was performed on two separate days with subjects and medical staff blinded to the order of food/placebo given. Gradually, the dose of placebo or causative food was increased at 20-minute intervals, and the test was ended until the participant either exhibited objective symptoms, exhibited significant subjective symptoms lasting >45 minutes, or consumed all the food samples (13). Participants who had a reaction of any duration on the active day (but not on the placebo day) were considered positive. Participants who did not react either on the active or placebo days were classified as tolerant, and participants who reacted on the placebo day were considered placebo responders (9). FA threshold information was recorded during DBPCFCs.
-
ARF is defined as reporting illness or trouble after consuming food. Self-reported FA was referred to as FA in the questionnaires. Doctor-diagnosed FA was referred to as FA diagnosed by a doctor. Food sensitivity (FS) was considered to be positive results for SPT or sIgE. Probable FA refers to a clinical history matched with IgE sensitization to the same food. Confirmed FA was defined as positive results in the DBPCFC.
-
Continuous variables were expressed as mean ± standard deviation and compared by a t-test or analysis of variance. Categorical variables were presented with frequencies and percentages: compared by a Chi-square test. Single factor and multivariate regression analysis were used to evaluate the relationship between food allergies and potential risk factors, as well as analyze possible confounding factors. FA prevalence in the case-control stage or confirmation stage were weighted back to the population in FA screening. Statistical analysis was performed with SPSS software (version 25.0, IBM Corp., Armonk, NY, USA). P values of <0.05 were considered significant.
-
The expert group formulated a Manual of Procedures, including standard operating procedures (SOP). All staff members were trained in SOP and all study centers followed the Manual of Procedures and standardized methodology. Each study center identified strategies to maximize response rates, such as mobilization meetings, text messages, phone calls, or emails. Data were cross-checked and verified by two people, which formed a database accessible via a web APP (Information Management System of Chinese FA Epidemiological Investigation) specifically designed for this project.
-
Ethical approval (Number 2019027) was obtained from the China National Center for Food Safety Risk Assessment ethical committee, and written, informed consent was obtained from the participants or their legal guardians.
-
This methodology of epidemiologic study on FA was implemented in Jiangxi, China in 2020.
-
The sub-survey centers were described in Figure 1A. Figure 1B showed a sampling flow chart. A total of 21,273 FA screening questionnaires were distributed in Jiangxi Province. The valid response rate was 97.8%. A total of 11,935 adults and 8,856 children were screened for FA; the mean age was 45±13 years and 8.7±1.3 years, respectively.
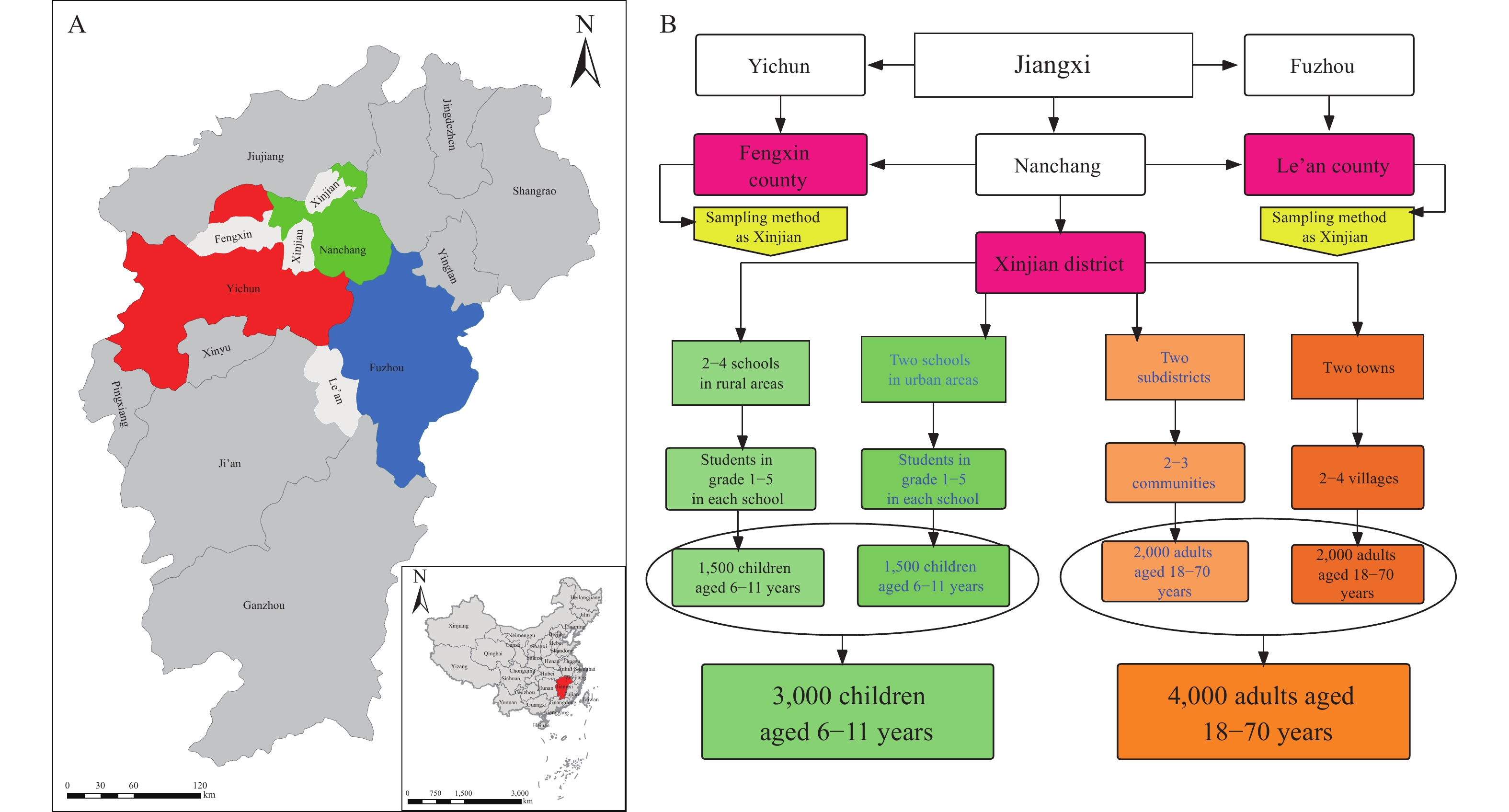 Figure 1.
Figure 1.Distribution of sub-survey centers and sampling flow chart in the study center of Jiangxi Province, 2020. (A) Distribution of sub-survey centers. (B) Sample size and sampling flow chart among adults and school children.
Note: In panel A, three prefectures were randomly selected in Jiangxi Province, they are Yichun, Nanchang, and Fuzhou, respectively, then Fengxin, Xinjan, and Le’an were randomly selected from the three prefectures as the sub-survey centers. In panel B, three prefectures were randomly selected in Jiangxi as sub-survey centers, and then about 3,000 school children and 4,000 adults were selected from each sub-survey centers by stratified cluster random sampling. -
Among all participants, 5.8% of responders reported ARF and 4.3% reported FA. Table 1 described the demographic characteristics of those who self-reported ARF and FA. Doctor-diagnosed FA was 2.20%, of which, 11.3% were diagnosed by oral food challenges where the main verifier of doctor-diagnosed FA was sIgE testing. This 3 stages of study across Jiangxi survey centers were presented in Figure 2.
Variables Population ARF FA N Percentage (%) Percentage (%) χ2 P Percentage (%) χ2 P Total 20,791 100.00 5.79 / / 4.29 / / Age Adult 11,935 42.60 8.21 165.35 0.00 2.90 145.71 0.00 Child 8,856 57.40 4.00 6.15 Gender Male 10,517 50.58 5.47 4.09 0.04 4.06 2.71 0.09 Female 10,274 49.42 6.12 4.52 Residence Rural area 10,755 51.76 5.74 0.09 0.76 4.12 2.10 0.15 Urban area 10,030 48.24 5.84 4.47 Sub-survey center Fengxin 6,670 32.08 6.99 40.98 0.00 5.53 57.36 0.00 Le’an 7,005 34.13 5.99 4.48 Xinjian 7,026 33.79 4.45 2.96 Ethnic Han 20,754 99.82 5.79 0.06 0.80 4.28 0.78 0.38 Others 37 0.18 8.11 8.11 Abbreviation: FA=food allergy; ARF=adverse reaction to food. Table 1. The demographic characteristics and prevalence of self-reported ARF and FA among children and adults in the study center of Jiangxi Province, 2020.
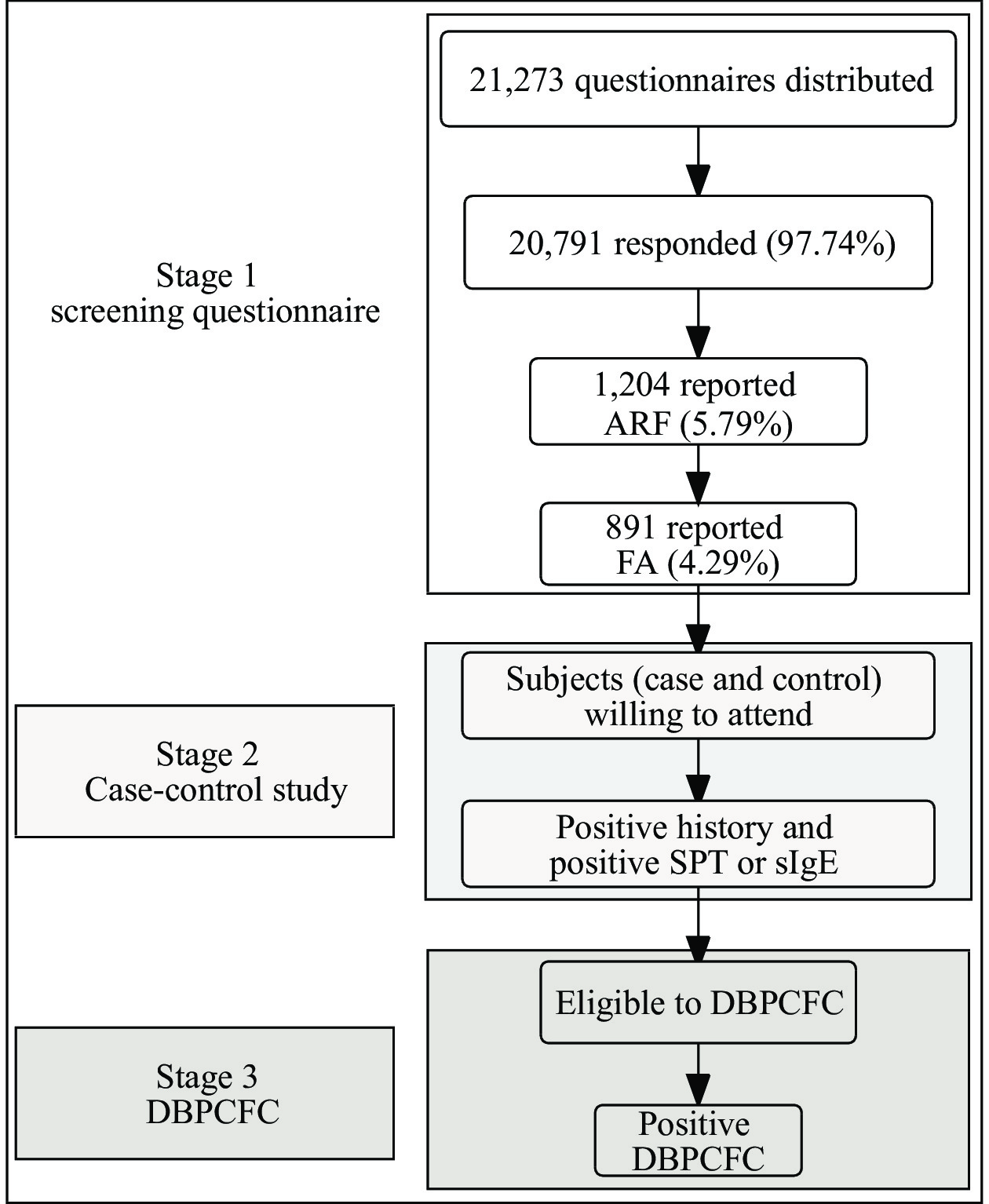 Figure 2.
Figure 2.Study population and multilevel assessment of FA among adults and school children in the study center of Jiangxi Province, 2020.
Note: The comprehensive clinical assessment of food allergy consists of three stages; the main research includes food allergy screening, structured interview, IgE sensitivity test, and oral food challenge test.
Abbreviation: ARF=adverse reaction to food; FA=food allergy; SPT=skin prick test; sIgE=Specific IgE; DBPCFC=double blind placebo-controlled food challenge.
-
The 8 most common causative foods were, in descending order, shrimp, mangos, shellfish, eggs, fish, beef, milk, and mutton; their prevalence was 1.95%, 1.22%, 1.07%, 0.68%, 0.49%, 0.35%, 0.34%, and 0.25%, respectively. Figure 3A shows the distribution of incriminated foods. Unlike in Europe, beef and mutton as offending foods were more common than peanuts and soybeans. Skin symptoms, such as rash or pruritus (itching), were the most frequently reported manifestation. Oral allergy symptoms were reported by 20.6% of subjects. Figure 3B presents the common symptoms of this self-reported FA.
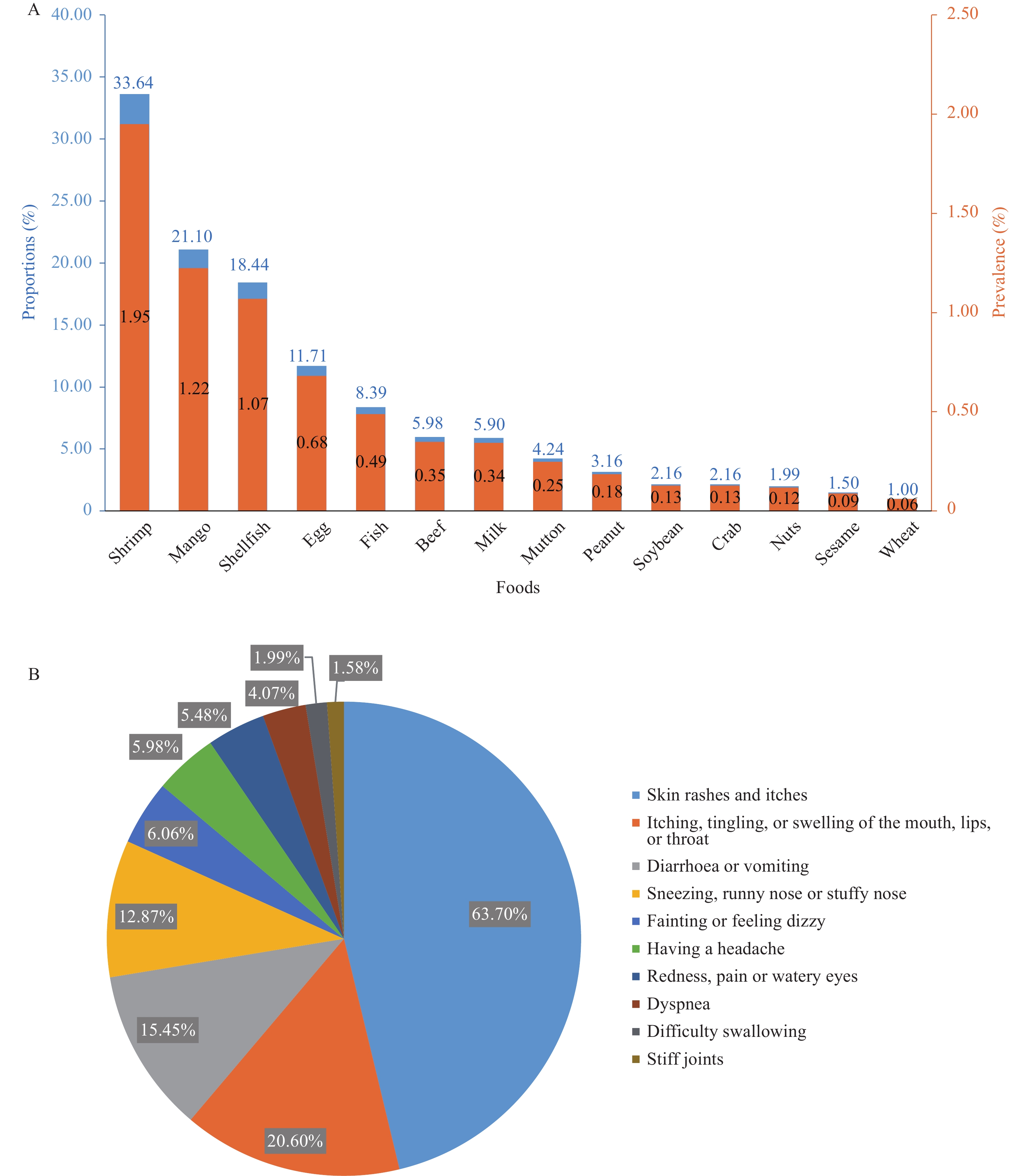 Figure 3.
Figure 3.Common causative foods and symptoms in the study center of Jiangxi Province, 2020. (A) Distribution of causative foods among adults and school children. (B) Percentage of common symptoms among adults and school children with food allergy.
-
The epidemic characteristics of FA are diverse across different countries and regions. In this study, the prevalence of self-reported ARF and FA was 5.79% and 4.29%, respectively, where shrimp was the most common offending food. Peanuts as a causative food was uncommon, unlike in America or Europe. Animal-derived foods were dominant as causative foods in China, but plant foods were dominant among adults with FA in most other countries (13). The most common FA in this study are different from those in high-income countries; this difference may mean that cultural, dietary, industrialization (1), and biological factors (14) play important roles in FA.
This is the first and largest multicenter, population-based cross-sectional study on FA with case-control nested in China, as well as the first to use a multilevel technical approach, including DBPCFC, to assess FA and threshold value, which ensures better comparability of data on FA across different countries or regions. The potential for non-response in different stages will be assessed and weighted back to the population of the FA screening so that results can more accurately reflect prevalence among the general population, including those not assessed (8).
This methodology also has limitations: the possible FA and the DBPCFC-confirmed FA are mainly focused on 20 priority foods and 9 common foods, respectively. Other foods are not considered and allergies to other types of foods could not be included. Geographically, there are regional differences in the effects of environmental exposure and dietary habits on food allergens; only eight PLADs were randomly selected as study centers, and the results may not completely reflect FA prevalence and variation across China overall.
This study provides baseline information about FA in China. The results will contribute to updating the labelling list of allergenic food, identifying the risk factors for the occurrence and development of food allergies, and estimating thresholds for the major food allergens. The study will also contribute to the improvement of preventive, administrative, and treatment strategies for food allergies in China.
-
No conflicts of interest.
HTML
Sampling Strategies
Sample Size
Questionnaires
Multistage of Study
Definition and Clinical Evaluation
Statistical Analyses
Study Management
Ethical Approval
Subjects
Self-reported ARF and FA
Common Causative Foods and Symptoms
| Citation: |

|