
 Download:
Download:




-
Herpes zoster (shingles) is a skin condition caused by the reactivation of varicella-zoster virus along dorsal nerve roots to the nerve root distribution on the skin, which causes a painful rash with blisters. Shingles mainly affect immunocompromised individuals and older adults (1). The most common complication of shingles is postherpetic neuralgia: a debilitating, burning pain that lasts long after the shingles blisters have healed. Treatment of shingles with antivirals can shorten the length and severity of shingles, but antiviral therapy should be started within 72 hours of the onset of the acute shingles rash and usually cannot be started in time (2). As such, vaccination is the best preventive measure. Recombinant zoster vaccines have been marketed in China for two years. Selecting the most suitable vaccine recipients can promote the implementation of the vaccine in China and effectively reduce the incidence of shingles. This study used a clustering methodology to partition age groups by shingles incidence using diagnostic data from January 1, 2017 through December 31, 2019 in Yichang, China. The highest risk age group was adults 55 years or older, with an average incidence of 10.13 episodes of shingles per 1,000 person-years. This age group is therefore the priority target for zoster vaccination. Among adults aged 28–54 years, shingles incidence increased with increasing age, requiring further study to identify potential shingles triggers.
In 2020, the recombinant zoster vaccine (RZV) was approved by China’s National Medical Products Administration for market authorization. RZV is a two-dose, subunit vaccine of a recombinant glycoprotein E with a novel adjuvant (AS01B) shown to prevent shingles in adults aged 50 and above with normal immune functioning (3). RZV is administered in 0.5-mL intramuscular injections in the deltoid region of the upper arm, with the 2 doses separated by 2–6 months. Post-licensure data showed vaccine efficacy to be 97.2% (95% CI: 93.7–99.0) in adults 50 years or older, with a relatively long duration of protection; 4 years after vaccination, efficacy is 93.1% (95% CI: 81.2–98.2) among adults greater than or equal to 50 years and 87.9% (95% CI: 73.3–95.4) among adults greater than or equal to 70 years. RZV is a non-program vaccine; the 2-dose series costs approximately CNY 3,240.
Effective and efficient use of RZV requires the identification of an optimal target population for vaccination. Because target population identification has great public health significance, real-world evidence from a large population-base of epidemiological data is needed. Real-world data from Yichang, China provided an epidemiological basis for determining the optimal age for shingles vaccination. Under the constraint of limited vaccine resources, maximizing public health value requires maximizing the reduction of the burden of disease by careful selection of priority target populations.
Data for this study came from the government-led Healthcare Big Data Platform in Yichang from January 1, 2017 through December 31, 2019. All shingles outpatient and inpatient cases from 49 medical institutions in 6 urban districts of Yichang were included in this study’s analyses. Shingles case inclusion criteria were an International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) disease code containing "B02" and diagnosis of "shingles." Clinical diagnostic criteria for case definitions required the following three symptoms or signs to be present simultaneously: clusters of blisters in the affected skin and distribution along a unilateral peripheral nerve dermatome, neuralgia with local lymph node enlargement, and normal skin outside of the affected dermatome.
This study estimated the number of permanent urban residents in all ages in 2017–2019 based on the total population of Yichang in 2020. The study calculated the year-of-age-specific incidences of shingles for 0 through 79 years of age; 80 years and above was considered as 1 age group. Age-group-specific shingles incidences during the 2017–2019 study period were ordered for cluster analysis with the K-means method. The K-means method is an unsupervised learning technique in which objects (year-of-age groupings for this study) are divided into clusters based on the epidemiological distance between objects, so that the data (incidence) would be maximally similar within a cluster but maximally dis-similar between clusters (4). The initial step was to determine the number of clusters, k, using the silhouette coefficient (SC) method. Values of SCs were between −1 and 1. The closer the SC values were to 1, the more optimal was the clustering. Once the optimal number of clusters was determined, the K-means method was used for cluster analysis. Data were analyzed using SPSS software (version 27.0, IBM Corp, Armonk, NY, USA), and the model was implemented in Python (version 3.10.4, Python Software Foundation, Fredericksburg, VA, US).
Based on the number of permanent (more than 6 months) urban residents and their duration of residence during 2017 to 2019, this study’s analytic dataset contained 5,691,939 person-years of observation: 2,872,042 men person-years and 2,819,897 women person-years. The overall incidence of shingles was 5.82 per 1,000 person-years (33,130/5,691,939); the incidence among women was 6.29 per 1,000 person-years (17,743/2,819,897) and the incidence among men was 5.36 per 1,000 person-years (15,387/2,872,042). Shingles incidence was thus significantly greater in women (P<0.05).
Shingles occurred in all age groups and increased with age. The incidence of shingles among children 0–9 years of age was low, but not 0. Shingles incidence increased significantly between 10 and 27 years of age and then plateaued between 30 and 50 years of age; incidence increased again after 55 years of age (Figure 1).
 Figure 1.
Figure 1.Age-specific incidence of shingles from 2017–2019 in Yichang, China.
Notes: Age-specific incidence in 2017–2019 was calculated by the following formulas: n=total urban permanent resident population×age composition ratio of Yichang in 2020; total observed person-years=n×observation years:
age-specific incidence=$\dfrac{{\rm{number\;of\;shingles\;cases\;at\;all\;ages}}}{{\rm{{total}\;{observed}\;{person}-{years}\;{in}\;{the}\;{fixed}\;{time}\;{period}}}}$.
There were 3 age-group categories that differed by incidence (k=3) (Figure 2): 0–27 years, 28–54 years, and 55 years and above (Figure 3). Mean shingles incidences were 1.86 per 1,000 person-years for 0–27-year-olds, 4.85 per 1,000 person-years for 28–54-year-olds, and 10.13 per 1,000 person-years for those 55 years or older.
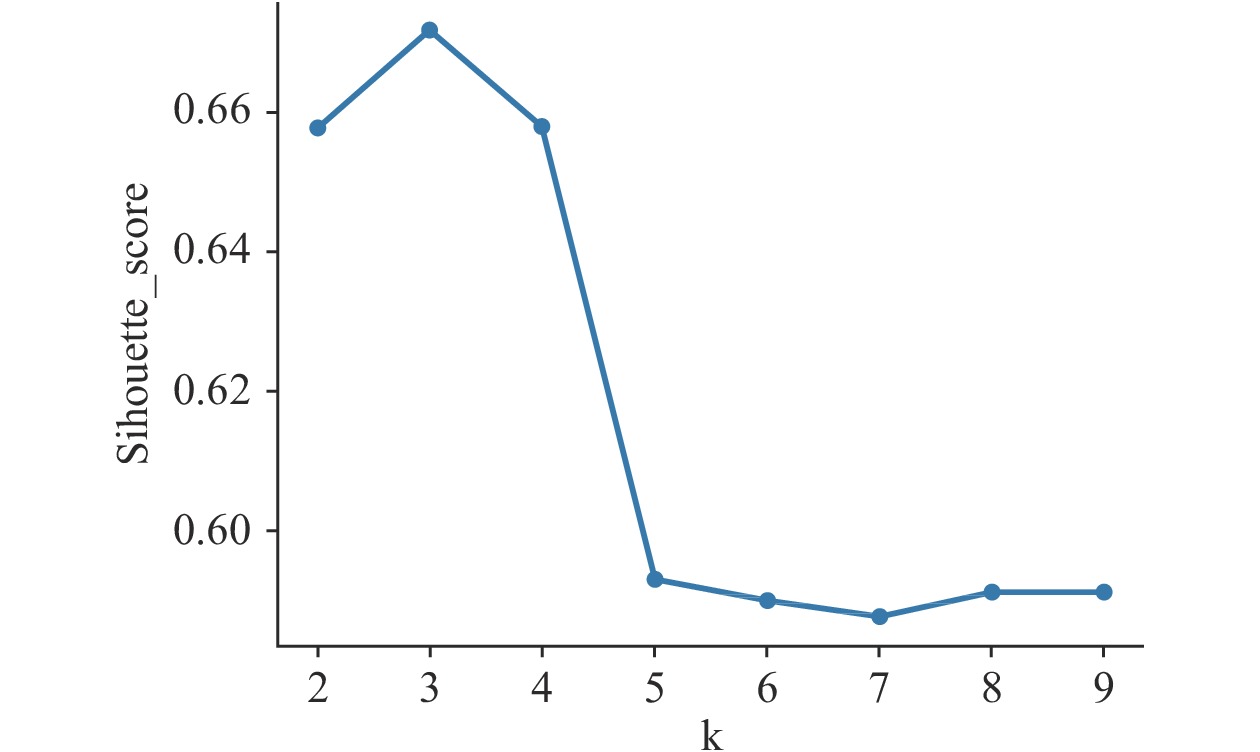 Figure 2.
Figure 2.The relationship between k and SC.
Notes: The higher the SC value, the better the clustering effect; k=3, SC(max)=0.6723.
Abbreviations: SC=silhouette coefficient/score (range –1 to 1); k=number of clusters.
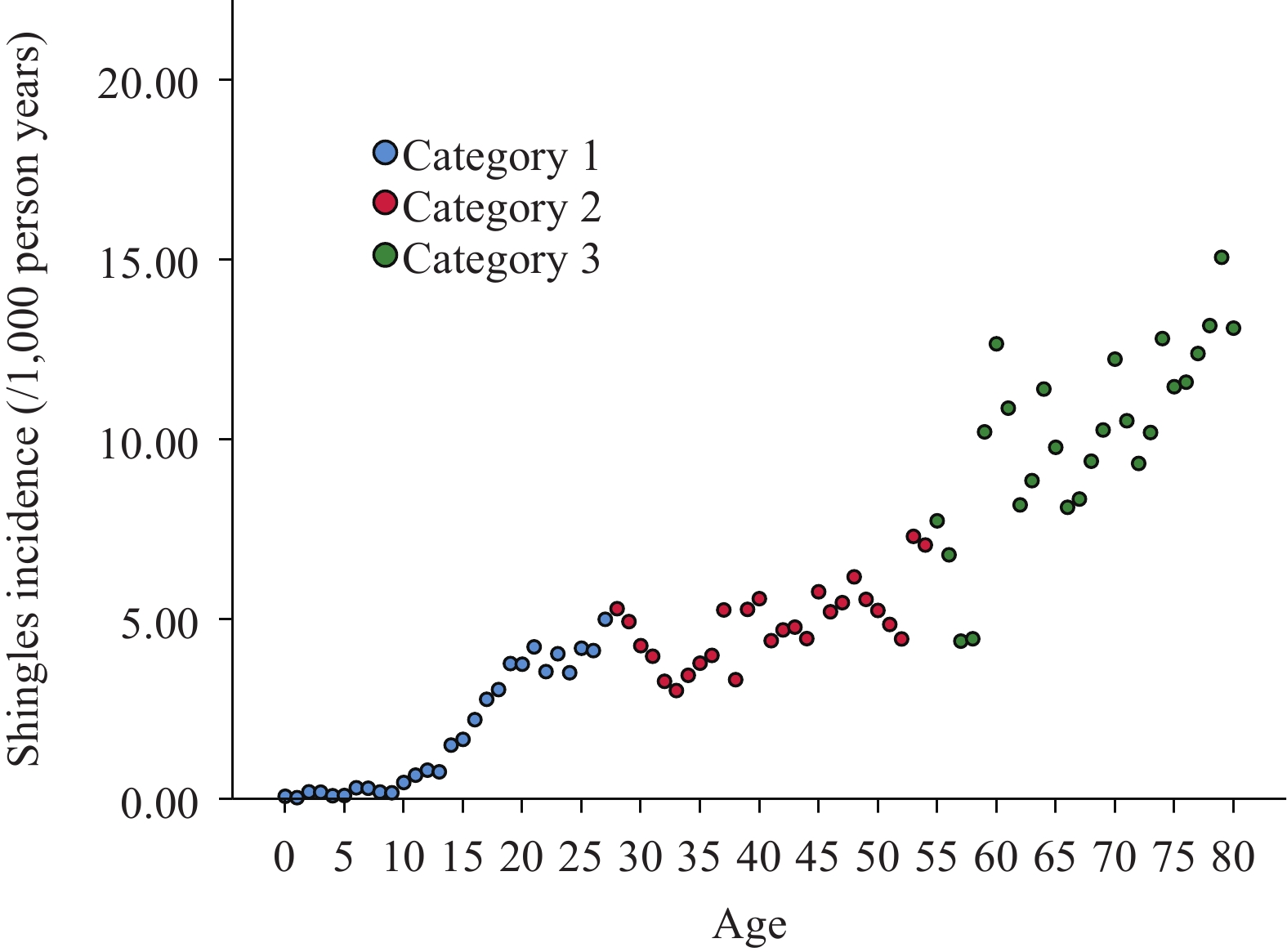 Figure 3.
Figure 3.Shingles incidence clusters arranged by age in Yichang, China, 2017–2019.
Notes: k=3 (1: 0–27 years; 2: 28–54 years; 3: ≥55 years). -
This study found that individuals of 55 years or older had the highest average incidence of shingles at 10.13 per 1,000 person-years of observation, accounting for 56.50% (18,720/33,130) of all cases in Yichang. Thus, shingles mainly affects older adults. China has more elderly people than any other country, and the proportion of the elderly population in China is becoming one of the highest in both Asia and the world (
5). In generalizing these results from Yichang to China’s population using the 6th population census, China is expected to have 12.58 million patients with shingles, including 5.27 million among those 55 years or older — an enormous burden of disease. This study of age-specific shingles incidence showed that vaccinating people 55 or older would have the greatest impact on the burden of shingles. However, the recommended age for shingles vaccination needs to also consider vaccine clinical trial populations and results, post-marketing monitoring, and other factors such as economic analyses. This study recommends conducting comprehensive socioeconomic evaluation and impact research with the Yichang Information System during vaccine implementation to provide a robust evidence base to refine vaccine target population selection.
This study found a plateau in incidence among 28–54-year-olds, although occurring with a relatively large incidence. In generalizing the 6th census data to all of China, it is estimated that 5.11 million young and middle-aged individuals will have shingles episodes — similar to the expected number of elderly cases (5.27 million). Shingles in this age are clearly worthy of attention. In addition to age, immunodeficiency is a well-known risk factor for shingles. The advancing age of onset (younger and younger ages) may be related to common, immuno-compromising, environmental conditions of modern middle-aged and young adults: such as high stress, low immunity, or fatigue. Case-control studies should be conducted in this age group to determine whether there is an association between these factors and shingles, and if so, to identify preventive measures.
Shingles incidence in Yichang from 2017 to 2019 was 5.82 per 1,000 person-years, which is slightly higher than in other studies (3–5 per 1,000 person-years) (6). Differences could be due to a variety of factors, such as genetic make-up, region, or study year. That the incidence of shingles increased with age and was concentrated in people 55 years or older is consistent with other studies (7). Similarly, the higher incidence in women is consistent with studies in Guangdong, China and the Republic of Korea (8-9). However, the mechanistic relationship between sex and shingles remains unclear (10).
Previous shingles epidemiological data in China was among people more than 50 years of age. Data in this study came from the Healthcare Big Data Platform of Yichang, which includes permanent urban residents of all ages. This study’s inclusive and large sample size allows for more fine-grained analyses. It was resultantly able to not only observe the entire population, but also refine analyses to obtain age-specific incidence rates all the way down to 1-year-olds. The objective and scientific clustering method used created age groupings based on clusters of single-year incidence rates. The finding that individuals 55 years or older had the highest shingles incidence, combined with census data on age structure, allowed a conclusion that, given limited immunization resources, the greatest public health benefit can be achieved by vaccinating that age group.
The study was subject to at least two limitations. First, no shingles monitoring system exists in the mainland of China. Hence some cases might not have been detected based on the big data from the hospital information system, underestimating the incidence. Second, demographic data for 1-year-olds in Yichang from 2017 to 2019 were not available. As such, data from the 7th population census in 2020 were used to estimate incidences in age groups from 2017 to 2019.
In conclusion, based on the epidemiological data analysis of the urban population in Yichang, China, individuals 55 years or older had the highest risk group of shingles. This age group should be considered as the priority target population for shingles vaccination. Attention should also be paid to the relatively high incidence of shingles in young and middle-aged people.
-
No conflicts of interest.
HTML
| Citation: |

|