
 Download:
Download:




-
Malaria is one of the most serious global public health problems. In 2020, there was an estimated 241 million malaria cases, up from 227 million in 2019, and primarily due to health service disruptions during the coronavirus disease 2019 (COVID-19) pandemic (1). The World Health Organization (WHO) certified China as malaria-free on June 30, 2021 (2) — a great inspiration to progress in global malaria elimination, which had unfortunately stalled. Anhui Province is in the eastern part of China; local transmission of malaria in Anhui has been interrupted since 2014 (3). In May 2021, long-term work for malaria elimination in the province was evaluated and affirmed by an independent Malaria Elimination Certification Panel organized by the WHO. Presently, prevention of malaria re-establishment is the priority in the province. However, this effort faces serious challenges from the COVID-19 epidemic. In this paper, we reported a case-based retrospective study of surveillance and response to imported malaria in Anhui Province from 2019 to 2021, including the time of COVID-19, with the aim of providing evidence for refinement of strategies and development of targeted interventions.
Every suspected malaria case in China is mandatorily reported through the China Information System for Disease Control and Prevention (CISDCP). We extracted data on malaria cases reported in Anhui Province between January 1, 2019 and December 31, 2021 from CISDCP and the Information System for Parasitic Disease Control and Prevention. Extracted data included demographic, epidemiological, diagnostic information of cases, and indicators of malaria surveillance and response. Reported cases were divided into two groups — reported before (first stage) or reported after (second stage) January 24, 2020, when the first-level response to COVID-19 was launched in Anhui Province. We compared malaria surveillance and response data between the first stage (January 1, 2019 – January 23, 2020) and the second stage (January 24, 2020 – December 31, 2021). Normally distributed quantitative variables were presented as means and standard deviations, and categorical data were presented as percentages. Differences in proportions were tested for statistical significance using Pearson’s chi-square (χ2) test or Fisher’s exact test, as appropriate. P values less than 0.05 were considered statistically significant.
There were 151 imported malaria cases reported in Anhui Province during the study period. The mean age was 44.0±10.3 years, and 148 cases (98.0%) were among males. There were 111 cases of Plasmodium falciparum (P. falciparum) infection and 36 cases of infection with other Plasmodium species including 4 Plasmodium vivax (P. vivax) cases, 24 Plasmodium ovale (P. ovale) cases, 8 Plasmodium malariae (P. malariae) cases, and 4 mixed infections (Figure 1). The number of imported malaria cases decreased from 98 in 2019 to 18 in 2021. The proportion of non-P. falciparum malaria increased from 17.3% in 2019 to 61.1% in 2021 (χ2=16.065, P<0.001).
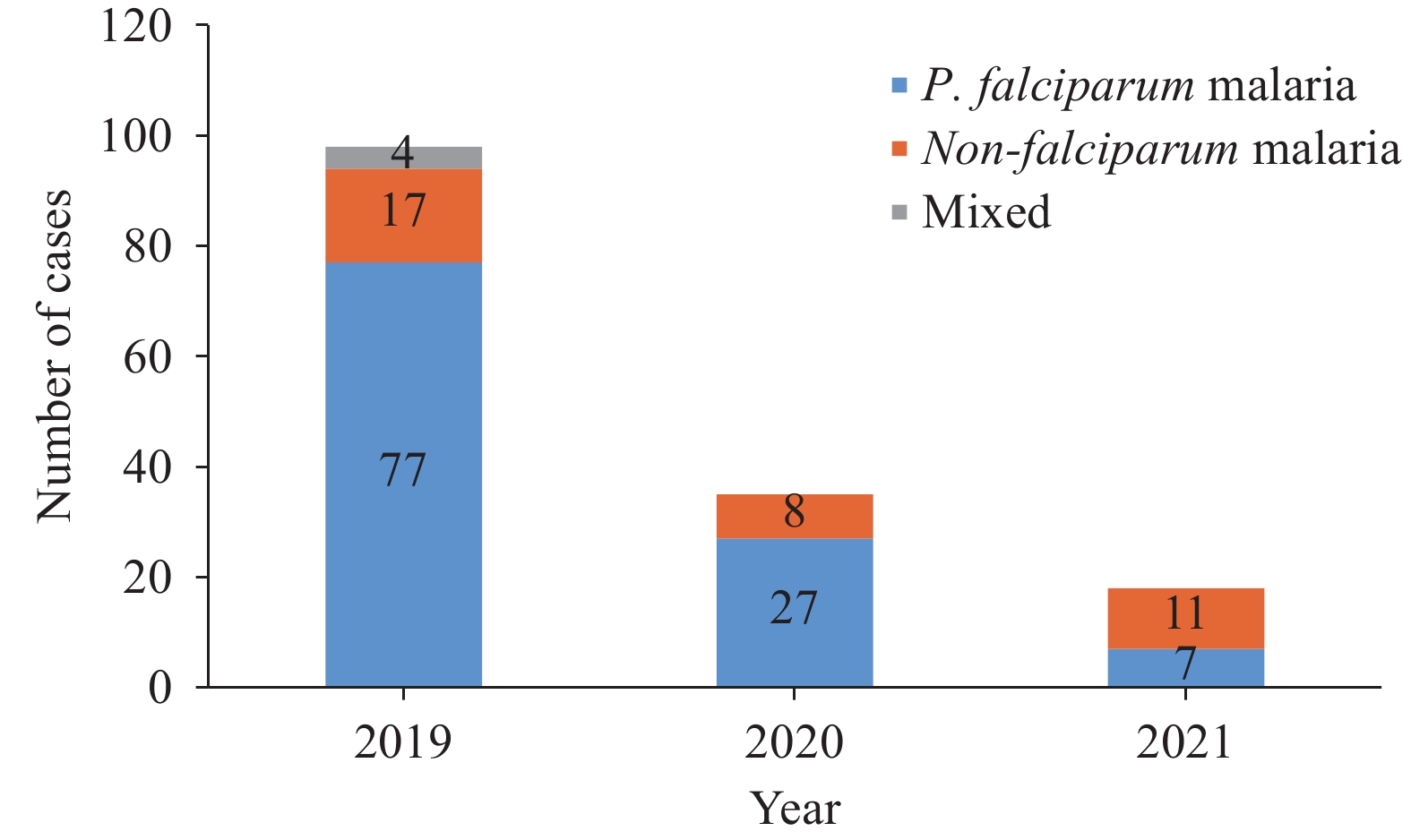 Figure 1.
Figure 1.Imported malaria cases reported in Anhui Province, 2019–2021.
A total of 110 cases were reported in the first stage. The time between arrival in China to symptom onset was shorter in the first stage than in the second stage (χ2=28.115, P<0.001). The percent of patients who received medical care during their first visit to a prefectural and county-level medical facility was 57.3% (63/110) in the first stage and 80.5% (33/41) in the second stage. Case profiles from onset to diagnosis were shown in Table 1.
Characteristics First stage,
n (%)Second stage,
n (%)χ2 P Time from arrival in China to symptom onset 28.115 <0.001 ≤30 days 102 (92.7) 23 (56.1) >30 days 8 (7.3) 18 (43.9) Time from onset to the first medical visit 0.016 0.901 ≤3 days 93 (84.5) 35 (85.4) >3 days 17 (15.5) 6 (14.6) Time from the first medical visit to diagnosis 0.108 0.743 ≤1 day 72 (65.5) 28 (68.3) >1 day 38 (34.5) 13 (31.7) Species 14.682 <0.001 P. falciparum 89 (84.0) 22 (53.7) Non-P. falciparum* 17 (16.0) 19 (46.3) Level of medical facilities at the first medical visit 6.951 0.008 County or prefectural level 63 (57.3) 33 (80.5) Other† 47 (42.7) 8 (19.5) Diagnosis at the first medical visit 0.003 0.953 Other diseases 37 (33.6) 14 (34.1) Malaria 73 (66.4) 27 (65.9) * non-P. falciparum includes P. vivax, P. ovale, and P. malariae. † medical facilities at provincial and township levels, and private facilities. Table 1. Profile of imported malaria cases from onset to diagnosis in Anhui Province, 2019–2021.
The percentages of cases reported within 1 day, of epidemiological investigation performed within 3 days, and investigated and disposed of within 7 days were 100% (110/110), 95.5% (105/110), and 98.1% (102/104), in the first stage, respectively, compared with of 100% (41/41), 95.1% (39/41), and 100% (40/40) during the second stage. Among first-stage cases, 98.2% (108/110) were initially detected parasitologically, 85.5% (94/110) were accurately identified by Plasmodium species, and all were confirmed by both PCR and microscopy. In contrast, 100% (41/41) of second-stage cases were detected parasitologically and confirmed, but only 70.7% (29/41) were correctly identified by species, significantly lower than in the first stage (χ2=4.286, P=0.038) (Table 2).
Stages Case management Laboratory detection Reported within one day
n (%)Case investigation within three days
n (%)Focus investigation and action within seven days*
n (%)Parasite detection¶
n (%)Species identification**
n (%)Rate of laboratory confirmation
n (%)First stage 110 (100.0) 105 (95.5) 102 (98.1) *,† 108 (98.2) 94 (85.5) 110 (100.0) Second stage 41 (100.0) 39 (95.1) 40 (100.0)*,§ 41 (100.0) 29 (70.7) 41 (100.0) χ2 NA 4.286 NA P 1.000†† 1.000†† 1.000†† 0.038 Abbreviation: NA=not applicable.
* Focus investigation and disposal within seven days: calculated according to the number of the current address in Anhui province.
† A total of 104 foci in the first stage.
§ A total of 40 foci in the second stage.
¶ Parasite detection: calculated according to whether or not malaria parasites were detected initially.
** Species identification: calculated based on the number of correctly identified species.
†† Fisher’s exact test.Table 2. Surveillance and response to imported malaria in Anhui Province, 2019–2021.
-
The COVID-19 pandemic has become one of the world’s most important public health concerns. Many malaria symptoms are similar to COVID-19 symptoms. The epidemic has disrupted health service delivery and timely malaria detection, reporting, diagnosis, and treatment (1). As China adheres to its dynamic zero-COVID policy to tackle imported and domestic SARS-CoV-2 infections, several strict measures have been implemented across the nation that affect case management of imported malaria.
Our study found that the number of imported malaria cases decreased dramatically in Anhui Province during the study period, with only 18 cases reported in 2021 — a reduction of 81.6% compared to the 98 cases reported in 2019, which is similar to the national trend (4-5). This decrease is likely due to international travel restrictions. Therefore, after the COVID-19 epidemic subsides and international population movement resumes, there may be a sharp increase in imported cases. It is essential to formulate scientific emergency plans to ensure effective management of imported malaria.
The larger percent of imported cases of non-P. falciparum (especially P. ovale) malaria was different from earlier studies that showed most cases imported into Anhui to be P. falciparum infections of people returning from endemic African countries (6). The change in imported malaria type is potentially attributed to the 14-or-more day quarantine for COVID-19 upon entry to China, which facilitates detection and reporting of P. falciparum infection during the quarantine period in the port of entry (7). Non-P. falciparum species such as P. vivax and P. ovale have a dormant hypnozoite stage that can trigger multiple episodes of malaria with longer latency. Some infected individuals do not develop symptoms until a year after returning to China (8), resulting in most non-P. falciparum cases being less likely to be detected during the quarantine period but being found and reported after returning to Anhui Province. Non-P. falciparum cases require more sensitive detection techniques for early identification. It is worth noting that the species identification rate during the second stage was lower than in the first stage (70.7% vs. 85.5%). This was possibly caused by the increased proportion of imported malaria cases infected with non-P. falciparum, which is difficult to identify by light microscope owing to similarities in morphology, especially between P. ovale and P. vivax (8), and by malaria rapid diagnostic tests, which are most efficient for detection of P. falciparum. Therefore, more sensitive and specific point-of-care detection methods for non-P. falciparum species need to be developed and introduced.
We found that 80.5% of cases received care during the first medical visit at prefectural and county-level facilities in the second stage, which was higher than the 57.3% rate in the first stage. This may be due to prohibition of primary medical institutions from dealing with fever cases, instead referring them to medical institutions with standardized fever clinics during the COVID-19 period. This turned out to also be beneficial for prompt diagnosis and appropriate treatment of malaria cases, because it was found that misdiagnosis rates in the first medical visits at primary medical institutions were high (9).
Our study also evaluated the implementation of the “1-3-7” approach. This approach was developed in 2012 and has guided malaria elimination in China. It includes three steps: case reporting within 24 hours, case investigation within 3 days, and focus investigation and disposal within 7 days to reduce the risk of secondary local transmission (10). In the post-elimination phase, the “1-3-7” approach is still used as a core indicator to evaluate the quality of malaria surveillance and response activities in China. In our study, all cases were reported within 24 hours and all foci were investigated and disposed of within 7 days, but there were 2 cases whose investigation took longer than 3 days due to staff involvement in the COVID-19 response. In general, malaria surveillance and response during the COVID-19 epidemic in Anhui Province remained sensitive, however, it is necessary to pay attention to a reasonable allocation of human resources for disease control and prevention.
In summary, due to international travel restrictions, entry quarantine, and the use of fever clinics during the COVID-19 period, imported malaria cases in Anhui Province decreased significantly, but a higher proportion of non-P. falciparum malaria infections were reported and a higher proportion of cases received medical care at the first visit. It is necessary to be vigilant about imported malaria during the COVID-19 epidemic, especially for non-P. falciparum infections, which are more difficult to detect.
-
No conflicts of interest reported.
-
The staff of medical and health institutions at different levels in Anhui for assistance.
HTML
| Citation: |

|