
 Download:
Download:




-
Non-pharmacological interventions (NPIs) have contributed substantially to the control of coronavirus disease 2019 (COVID-19) (1-2) and have bought time for vaccine development and promotion. With increasing vaccine coverage, some countries have relaxed NPIs. However, breakthrough infections, especially from viral variants, caused significant rebounds of COVID-19 epidemics (3) that were unable to be controlled without re-tightening NPIs (4).
Despite the effectiveness of NPIs, they negatively impact daily life and the economy (5). Given the well-documented high efficacy of COVID-19 booster doses (a dose of COVID-19 vaccine 6 months after completing a primary series) (6), China initiated a booster vaccination campaign, with an expectation to return to normal life and lift NPIs (7). With booster vaccinations, it is a concern that when and how NPIs could be lifted without devastating the healthcare system. This includes questions of how many medical resources, such as hospital beds, intensive care unit (ICU) beds, and hotel rooms for border quarantine, are necessary as different levels of NPIs are lifted.
To address these critical questions, we used real-world data from multiple sources as input to a susceptible-infectious-recovered (SIR) model that we augmented with additional compartments to more accurately represent COVID-19 epidemiology and control policy in China. For 2022, we projected the magnitude of the COVID-19 epidemic in Guangdong Province under different NPI lifting policies, booster dose uptake, and overseas importation pressures.
-
Starting with an SIR framework, we introduced additional compartments to model risks, factoring in people entering from overseas, border quarantine, and booster vaccination coverage (Figure 1). Details of the model are in the Supplementary Material.
 Figure 1.
Figure 1.Conception model incorporating booster vaccination and NPIs.
Note: Details of the model are in the Supplementary Material (available inhttp://weekly.chinacdc.cn ).Abbreviation: NPIs=non-pharmacological interventions. -
We estimated the number of infected people entering Guangdong from overseas as follow:
$$ {I}_{in}=\sum {Passenger}_{t}\times 0.98\% $$ where Passengert denotes the number of passengers from overseas at date t, which was obtained from flight data in VariFlight (https://www.variflight.com/en/). We used flight data from 2019 — the pre-pandemic level of passengers — to project flights in 2022 under various levels of restriction. We used the prevalence of COVID-19 cases imported from overseas to Guangdong from August 7, 2021 to November 14, 2021 (0.98%) to estimate the number of imported infections each day projected onto 2022 travel levels.
-
Two scenarios for booster vaccination in 2022 were used for modeling. The first scenario was 60% of the population receiving a booster by June 30 and 85% receiving a booster by December 31. The second scenario was 50% and 75% booster vaccination by June 30 and December 31. Rationale for the scenarios is in the Supplementary Material.
-
Inactivated COVID-19 vaccines have been the most widely used vaccines in China; their effectiveness against infection is 65.70% for fully vaccination (8). With a booster dose, vaccine effectiveness (VE) is 88.00% (6). Therefore, we used 65.70% and 88.00% for the VE parameters, Pprotect2 and Pprotect3.
Vaccination reduces hospital admission, severe illness, and death. Based on previous studies (6,8-10), we set the hospital admission rate, ICU admission rate, and fatality rate to 4.30%, 0.39%, and 0.80%, respectively, for fully vaccinated but infected individuals, and 0.30%, 0.03%, and 0.15%, respectively, for booster-vaccinated infected individuals.
-
Border Quarantine: We developed five scenarios of border quarantine of people coming from overseas to Guangdong in 2022: 1) no border quarantine; 2) 7 days of quarantine; 3) 14 days of quarantine; 4) 7 days of quarantine for those entering before July, but no quarantine for those entering after July; and 5) 14 days of quarantine before July but 7 days for those entering after July.
A certain proportion of cases from overseas may not be detected during quarantine. Based on real-world data from Guangdong, 1.04% and 0.16% of cases from overseas were not detected during 7- and 14-day quarantines. We used these values to represent residual importation risk after testing negative during quarantine.
Infection Detection Measures: In our model, μ denotes the rate of infected people being detected and quarantined. For different infection detection measures, the interval from infection to quarantine was obtained from real-world data in Guangdong (Supplementary Table S1).
Personal Protection and Social Distancing: A meta-analysis indicated that relative risk (RR) reduction from masks and social distancing were 0.47 and 0.75, respectively (2). Given that the combined effect of personal protection and social distancing was rarely reported, we used the lowest RR (0.47) to represent this combined effectiveness.
-
We modeled 4 strategies that differed by combination of NPIs: 1) containment: 14 days of border quarantine of incoming travelers; use of personal protection, social distancing, and use of sensitive measures for infection detection (fever monitoring and contact tracing); 2) suppression: 7 days border quarantine; use of personal protection, social distancing, and sensitive measures for infection detection; 3) mitigation: no border quarantine; use of personal protection, social distancing, and routine measures for infection detection (fever monitoring but no contact tracing); and 4) coexistence: no border quarantine, no personal protection, no social distancing, and only routine measures for infection detection.
-
The transmission coefficient, β, was estimated using real-world data from a local epidemic triggered by imported cases from Africa in first half of 2020. The data indicated that the β with best fit was 0.14 (R2=84.71%, Root Mean Square Error=3.61). During that outbreak, vaccination was unavailable, and therefore this β represents transmission with local NPIs and no vaccination. Given viral variants can have higher transmission rates (transmissibility of variants can reach 1.97 times non-variant transmission) (11), we set β as 0.14×1.97=0.27 to represent the transmission rate in 2022. We also set β as 0.27/0.47=0.57 to represent transmission without personal protection and social distancing.
Detailed definitions and values of compartments and parameters are presented in Supplementary Table S2 and Supplementary Table S3. Statistical analyses were conducted with R software (version 3.6.2, R Foundation for Statistical Computing, Vienna, Austria). We used the R package “deSolve” for numerical treatment of our model’s system of differential equations in transmission dynamics analyses.
-
From January 1 to November 14, 2021, 3,768 flights carried 349,987 people into Guangdong from overseas; 2,702 (0.77%) were infected. The percent was higher near the end of 2021 (0.98%). Using the percent infected as a multiplier, Figure 2 shows projected overseas travelers and numbers infected in 2022 under assumptions of 20%, 50%, and 100% of travelers from overseas compared with 2019.
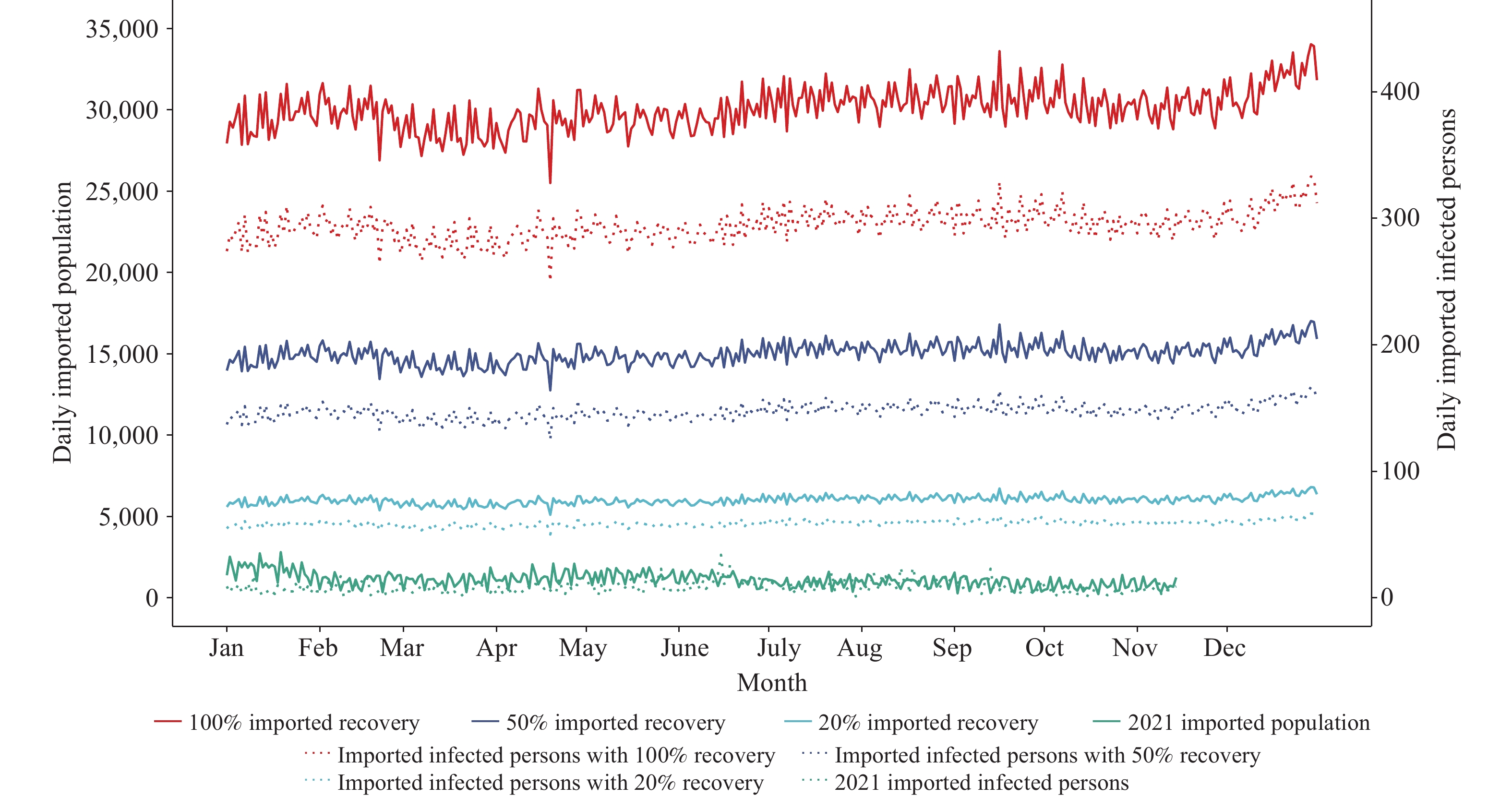 Figure 2.
Figure 2.Projected daily incoming travelers and number infected in 2022 and actual figures for 2021.
-
Modeling results were based on the percent of 2019 travel into Guangdong that occurs using the percent infected from real world data near the end of 2021 — 20%, 50%, and 100% of 2019 travel into Guangdong, called travel recovery.
Containment: With 2022 incoming travel at a 20% recovery of 2019 travel, a containment strategy controls the maximum number daily infections at low level (Figure 3), with annual cases and deaths of 215 and 2 (Figure 4). As booster dose coverage increases, daily cases become lower (Figure 3). With higher percentages recovery of 2019 travel, the epidemic is still controlled by containment.
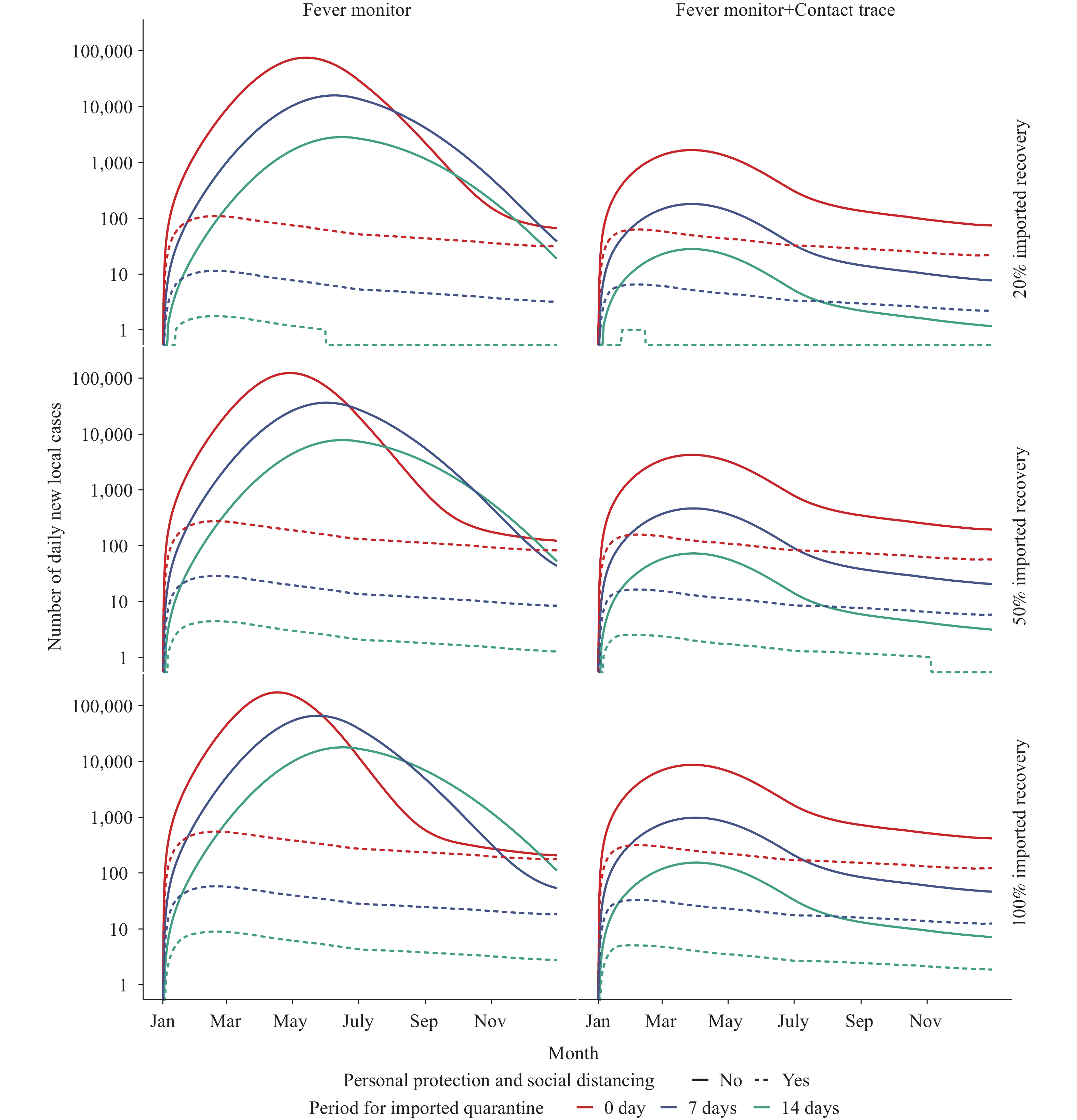 Figure 3.
Figure 3.Projected daily new COVID-19 local cases under different NPI lifting scenarios in Guangdong Province in 2022.
Note: A log10 transformed y-axis was used in this figure. 1) containment strategy: 14 days border quarantine of incoming travelers, use of personal protection and social distancing, sensitive measures for infection detection (fever monitoring and contact tracing); 2) suppression: 7 days border quarantine, use of personal protection and social distancing, sensitive measures for infection detection; 3) mitigation: no border quarantine for travelers, use of personal protection and social distancing, routine measures for infected persons detection (fever monitor without contact tracing); 4) coexistence: no border quarantine, no personal protection, no social distancing, routine measure for infected persons detection (no contact tracing). Abbreviations: COVID-19=coronavirus disease 2019; NPI=non-pharmacological interventions.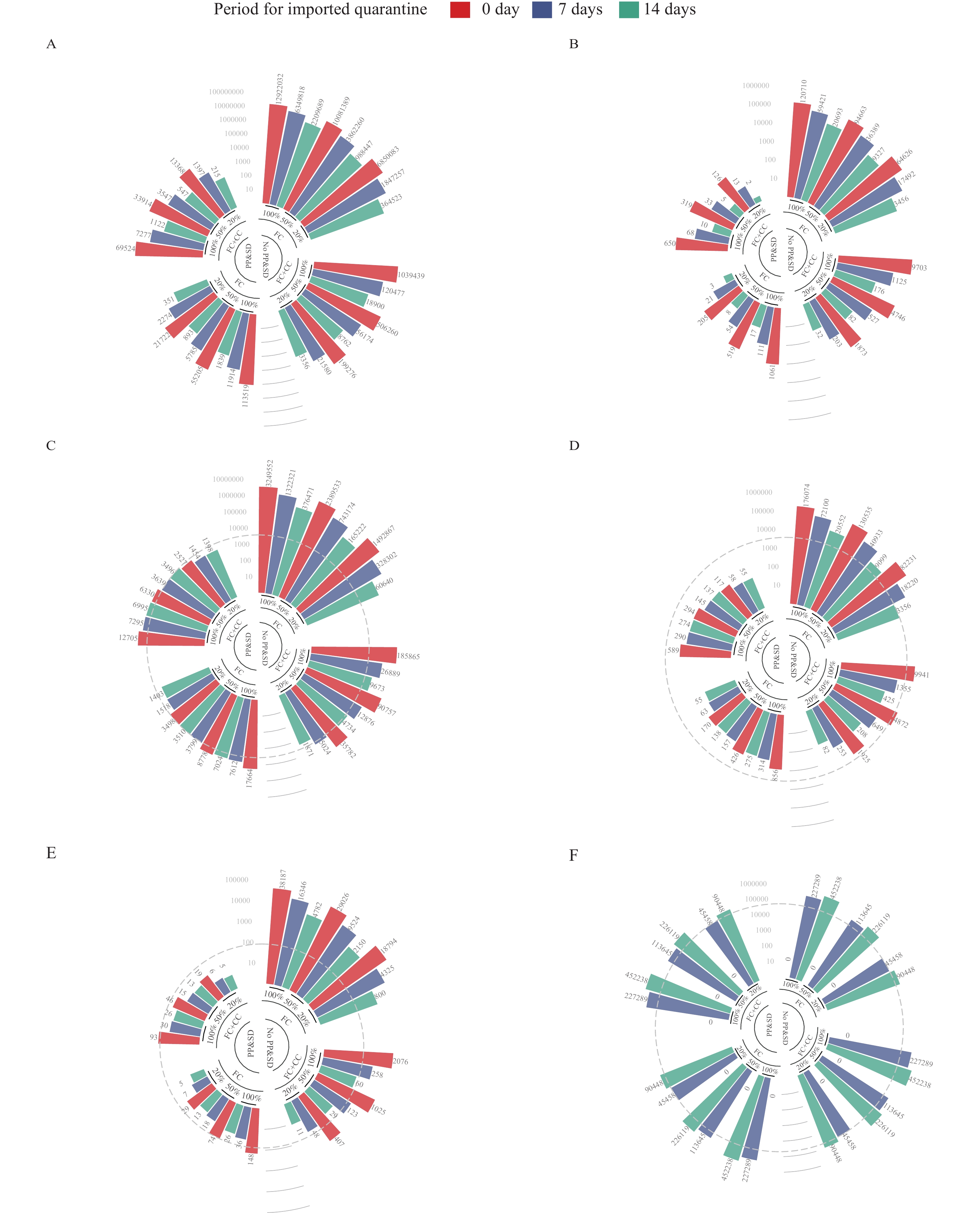 Figure 4.
Figure 4.Cumulative number of local COVID-19 cases and deaths, and the maximum required number of hospital beds, ICU beds, and hotel rooms for border quarantine under different scenarios. (A) Cumulative cases; (B) Cumulative deaths; (C) Required hospital beds (all infected persons hospitalized); (D) Required hospital beds (severe infected persons hospitalized); (E) Required ICU beds; (F) Required hotel rooms for imported quarantine.
Note: The grey dashed lines refer to the current capacity of medical resources in Guangdong Province. PP&SD refer to personal protection and social distancing; FC refers to fever clinic monitor; CC refers to close contact tracing; 20%, 50% and 100% refer to 20%, 50% and 100% travel recovery compared with 2019 incoming overseas travel. Abbreviations: COVID-19=coronavirus disease 2019; ICU=intensive care unit.Suppression: With 20% recovery of travel, a suppression strategy controls the maximum daily infections at 7 (Figure 3), with 1,397 total cases and 13 deaths (Figure 4). If booster dose uptake is 85%, the maximum daily number of local infections decreases to 2. With 50% and 100% of travel recovery, the cumulative number of cases is projected to become 3,547 and 7,277.
Mitigation: With 20% recovery of travel, a mitigation strategy results in a maximum of 63 infections per day, with 21,722 total cases and 205 deaths. A booster dose coverage of 85% reduces the maximum daily infections to 22. However, 50% and 100% travel recovery yields 55,205 and 113,519 total cases in Guangdong.
Coexistence: If most NPIs are lifted, 20% travel recovery brings the projected daily maximum of cases to 75,716, with annual cases and deaths of 6,850,083 and 64,626. With 50% and 100% travel recovery, Guangdong would suffer 10,081,389 or 12,922,032 cases in 2022.
-
Containment: At 20% travel recovery, at the peak of epidemic, 1,398 infected people, including locals and incoming travelers, will require quarantine and isolated treatment. Infected individuals are always hospitalized in China, implying the need for 1,398 hospital beds at epidemic peak. If only severe cases are hospitalized, 55 hospital beds and 5 ICU beds will be needed, but 90,448 hotel rooms will be needed for border quarantine. With 50% and 100% travel recovery, the peak needs for treatment will be 3,496 and 6,995 hospital beds and 226,119 and 452,238 quarantine rooms, respectively.
Suppression strategy: At 20% travel recovery, at the peak of the epidemic, 1,454 hospital beds will be needed. If only severe cases are hospitalized, 58 beds will be needed. Compared to containment, suppression requires fewer hotel rooms for imported quarantine (45,458), which is within Guangdong’s capacity. With 50% and 100% travel recovery, 3,639 and 7,295 hospital rooms will be needed at epidemic peak, and 113,645 and 227,289 quarantine hotel rooms will be needed, respectively.
Mitigation: With 20% travel recovery, 3,498 hospital beds will be needed at peak if all infected individuals are hospitalized; 170 hospital beds will be needed if only severe cases are hospitalized. A peak of 29 ICU beds would be needed. With travel recovery of 50% and 100% levels, 8,778 and 17,664 hospital beds will be needed.
Coexistence: With 20% travel recovery, 1,492,867 hospital beds would be required at peak. If only severe cases are hospitalized, 82,231 hospital beds will be required. With 50% and 100% travel recovery, Guangdong would have to arrange 2,389,533 and 3,249,552 hospital beds for treatment of infected individuals.
As shown in Supplementary Table S4, the epidemic would require more medical resources with slower booster vaccination progress. More sensitive infection detection measures would slow the epidemic.
-
We developed dynamic severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) transmission models to project the COVID-19 epidemic in Guangdong in 2022 under combinations of COVID-19 booster vaccination, increases of incoming international travel, and 4 NPI lifting strategies to identify appropriate NPI combinations that will keep the COVID-19 epidemic under control and utilize affordable levels of medical resources.
If incoming international travel recovers to 20% of the level in 2019 and the infection rate of incoming travelers is the same as in 2021 in Guangdong, a suppression strategy may be considered in 2022. Suppression involves reducing incoming quarantine to 7 days, using personal protection and social distancing, and contact tracing during outbreaks. Under this scenario, the required medical resources will be within the current capacity of Guangdong. Our model also indicated that with increasing uptake of booster doses, the number of daily new infections decreased significantly. We project that a high booster dose vaccination rate of 85% will allow more incoming travel and decreased use of NPIs by the end of 2022.
Furthermore, several antiviral medicines against COVID-19 are being developed and some have been granted regulatory approval (12-13). Effective antivirals raise the possibility that infected people with mild symptomatic may be able to be safely treated at home, partially alleviating stress on the medical system.
This study was subject to several limitations. We assumed that reinfection would not occur. This assumption may cause the model to underestimate the epidemic magnitude and peak. We also did not consider the waning of booster-dose-induced immunity over time and assumed that the prevalence of imported COVID-19 in 2022 will be the same as it was in 2021. Additionally, we were under the assumption that the transmissibility of the virus in 2022 will be the same as the Delta variant. Given that the Omicron variant has higher transmissibility than Delta and that future variants may also have high transmissibility, our results may be underestimates. Our model used an SIR structure rather than an SEIR (susceptible, exposed, infectious, and recovered) structure for simulation. However, given that COVID-19 cases can transmit during the incubation period (14), SIR models have been used successfully (15) and we believe that an SIR structure reasonably simulates COVID-19 epidemics. Finally, our model did not consider vaccination effectiveness against SARS-CoV-2 infectiousness (VEI).
As booster vaccination increases in 2022, incoming international travel could increase slightly, but a suppression strategy should be maintained to ensure that the resulting COVID-19 epidemic can be maintained under control. High coverage of booster dose vaccinations along with the use of antiviral medicines and increasing the availability of medical resources, could allow for the possibility of lifting border restrictions and NPIs in the near future.
-
No conflicts of interest.
HTML
Model Structure
COVID-19 Risk from Overseas Importation

Vaccination Rate in 2022
Vaccine Effectiveness
Four Strategies Against COVID-19
Transmission Coefficient (Beta)
Travelers from Overseas and Imported Infections
Projected Epidemic in 2022 by COVID-19 Strategy
Projected Medical Resource Requirements by Strategy
| Citation: |

|