Download:
Download:




-
Few studies have elucidated the associations between short-term exposure to ozone and respiratory morbidity, especially in developing countries. We designed this time series study (from 2013 to 2015) in 5 cities in China to investigate the relationships between ambient ozone concentrations and respiratory outpatient visits. Health data were obtained from 9 hospitals and exposure data were collected from fixed-site monitoring stations. Generalized additive models were used to analyze hospital-specific associations and then a random-effect meta-analysis was used to pool them. The average concentrations of ambient ozone for each city ranged from 40.89 μg/m3 to 75.56 μg/m3, and the daily mean counts of respiratory outpatient visits varied by hospital from 37 to 2,191. In the present study, we observed positive associations between ozone exposure and respiratory outpatient visits, and the associations remained robust in sensitivity analyses. For a 10 μg/m3 increase in ozone concentration (lag 03 days), there was a 0.91% (95% CI: 0.34%, 1.47%) increase in the count of outpatient visits for respiratory diseases. Furthermore, the significant associations occurred earlier and became slightly stronger during warm periods. This study suggested a significant and lagged association between short-term exposure to ozone and increased respiratory morbidity.
We conducted this time series study in the cities and municipalities of Shanghai, Zhoushan, Guangzhou, Wuhan, and Xi’an, which are located in different geographic regions with a wide diversity in ozone concentrations. The study period was from January 1, 2013 to December 31, 2015. Data on outpatient visits were obtained from 9 hospitals with 1 to 2 hospitals from each city, including tertiary and secondary hospitals to capture a more representative sample of patients. The hospitals were selected according to data accessibility. Outpatient visits for respiratory diseases were diagnosed and classified according the 10th International Classification of Diseases (ICD-10: J00-J99), and the daily counts were subsequently extracted by experienced physicians. The study was restricted to resident populations. Exposure data on the 5 criterial air pollutants and weather conditions were obtained from the National Urban Air Quality Real-time Publishing Platform and the China Meteorological Data Service Center, respectively. Daily concentrations of each air pollutant were averaged from all available measurements from fixed-site monitoring stations by city.
We applied a two-stage analytic strategy. In the first stage, we estimated hospital-specific associations using generalized additive models with quasi-Poisson regression. Several covariates were a prior added into the model (1) and details are provided in the supplementary material. According to the results from a previous study (2), a moving average of the current and previous 3 days (lag 03 d) exposure was used for the main model. In the second stage, we pooled hospital-specific estimates using a random-effect meta-analysis. To illustrate the pooled association between ozone and respiratory outpatient visits, we plotted an exposure–response (E-R) curve via the same approach as done in a previous study (3). We further conducted a stratified analysis by season (warm season, from May through October; cool season, from November through April). To examine the robustness of the main models, we performed 2 sensitivity analyses and details are provided in the supplementary material. All statistical analyses were conducted in R software (version 3.6.1, R Foundation for Statistical Computing, Austria) using the “mgcv” and “rmeta” packages. Effect estimates were presented as percentage changes and their 95% confidence intervals (CIs) in the count of respiratory outpatient visits that were associated with a 10 μg/m3 increase in ozone concentration. A two-sided p<0.05 was considered statistically significant.
Table 1 summarizes the descriptive statistics on ozone concentrations and counts of respiratory outpatient visits. The mean concentrations of ambient ozone ranged from 40.89 ± 23.95 μg/m3 in Xi’an to 75.56 ± 24.61 μg/m3 in Zhoushan. The average daily counts of outpatient visits varied substantially by hospital from 37 ± 13 in Hanyang Hospital of Wuhan to 2,191 ± 523 in Xinhua Hospital of Shanghai.
City/Hospital Mean SD Min P25 Median P75 Max Ozone Shanghai * 70.22 28.69 9.97 48.68 71.37 89.95 176.23 Zhoushan * 75.56 24.61 4.83 58.18 75.47 92.00 156.88 Guangzhou 46.99 24.32 4.81 27.98 43.27 61.77 147.44 Wuhan 59.38 29.85 7.27 35.27 57.34 79.69 166.25 Xi’an 40.89 23.95 6.70 20.82 35.73 57.25 128.19 Outpatient visit Hospital 1 (Shanghai) * 2,191 523 696 1,878 2,186 2,503 3,872 Hospital 2 (Zhoushan) * 412 81 110 360 411 464 678 Hospital 3 (Zhoushan) * 296 82 90 238 296 350 573 Hospital 4 (Guangzhou) 945 330 35 721 991 1,165 2,006 Hospital 5 (Guangzhou) 198 105 1 108 209 275 522 Hospital 6 (Wuhan) 43 17 0 33 43 52 147 Hospital 7 (Wuhan) 37 13 4 28 35 44 96 Hospital 8 (Xi'an) 488 188 44 382 529 621 894 Hospital 9 (Xi'an) 419 127 31 332 424 509 742 Abbreviations: SD=standard deviation; Min=minimum; Max=maximum; P25=25th percentile; P75=75th percentile.
* Data were from January 1, 2014 to December 31, 2015.Table 1. Summary statistics on ambient ozone concentrations in 5 cities and the count of outpatient visits for respiratory diseases in 9 hospitals from 2013 to 2015.
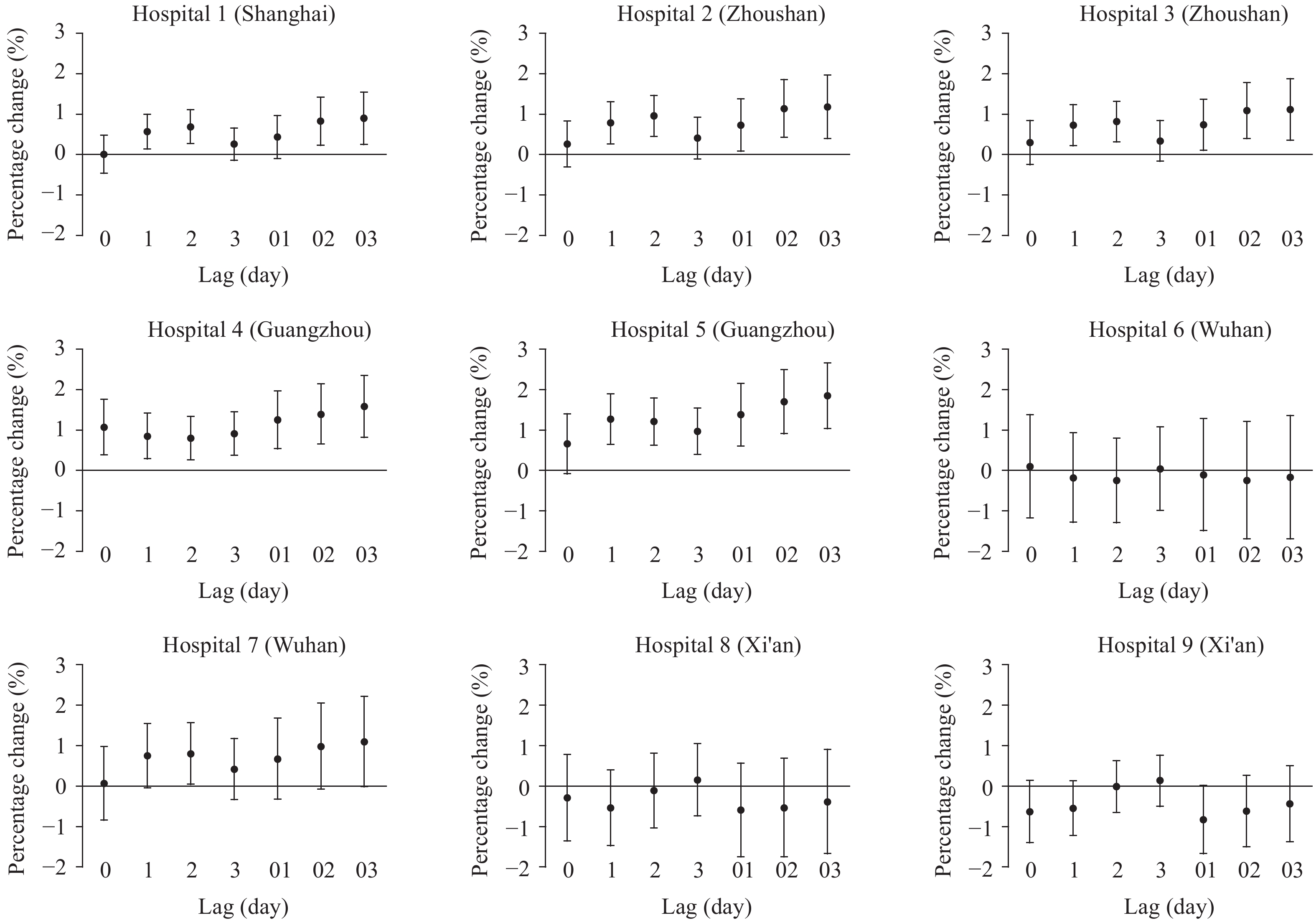
Figure 1 shows the lag pattern of the associations between ozone and outpatient visits for respiratory diseases. For the single-day lags, the significant association occurred at a lag of 1 day, became the strongest at a lag of 2 days, and then was attenuated over longer lag periods. When exposure was lagged over multiple days, the association became the strongest during the 0–3 days lag period. For this lag period, a 10 μg/m3 increase in ozone concentration was associated with a 0.91% (95% CI: 0.34%, 1.47%) increase in the count of outpatient visits for respiratory diseases. The estimates of hospital-specific associations between ozone and outpatient visits are available in the supplementary material (Supplementary Figure S1). Figure 1 also depicts the associations by season. In warm seasons, the association was significant in the present day of exposure and could last for 3 days, whereas the association in cool seasons became significant at a lag of 2 days. For multiple-day lags, the associations in warm seasons were slightly stronger than that in cool seasons. The pooled relationship between ozone and respiratory outpatient visits had no obvious changes after adjusting other air pollutants or altering the degrees of freedom of the smooth functions for time trend and weather conditions (Supplementary Table S1).
 Figure 1.
Figure 1.Percentage changes in the daily count of outpatient visits for respiratory diseases per 10- μg/m3 increase in ambient ozone concentration over different single-day and multiple-day lag periods. Warm season refers to the period from May through October and cool season refers to the period from November through April.
Figure 2 illustrates the E-R curve for the association of ozone exposure (lag 03 days) with respiratory outpatient visits. Specifically, the curve increases slowly at low concentrations (<50 μg/m3) and moderately at 50 μg/m3 to 100 μg/m3, levels off at 100 μg/m3 to 120 μg/m3, and raises rapidly when concentrations were >120 μg/m3.
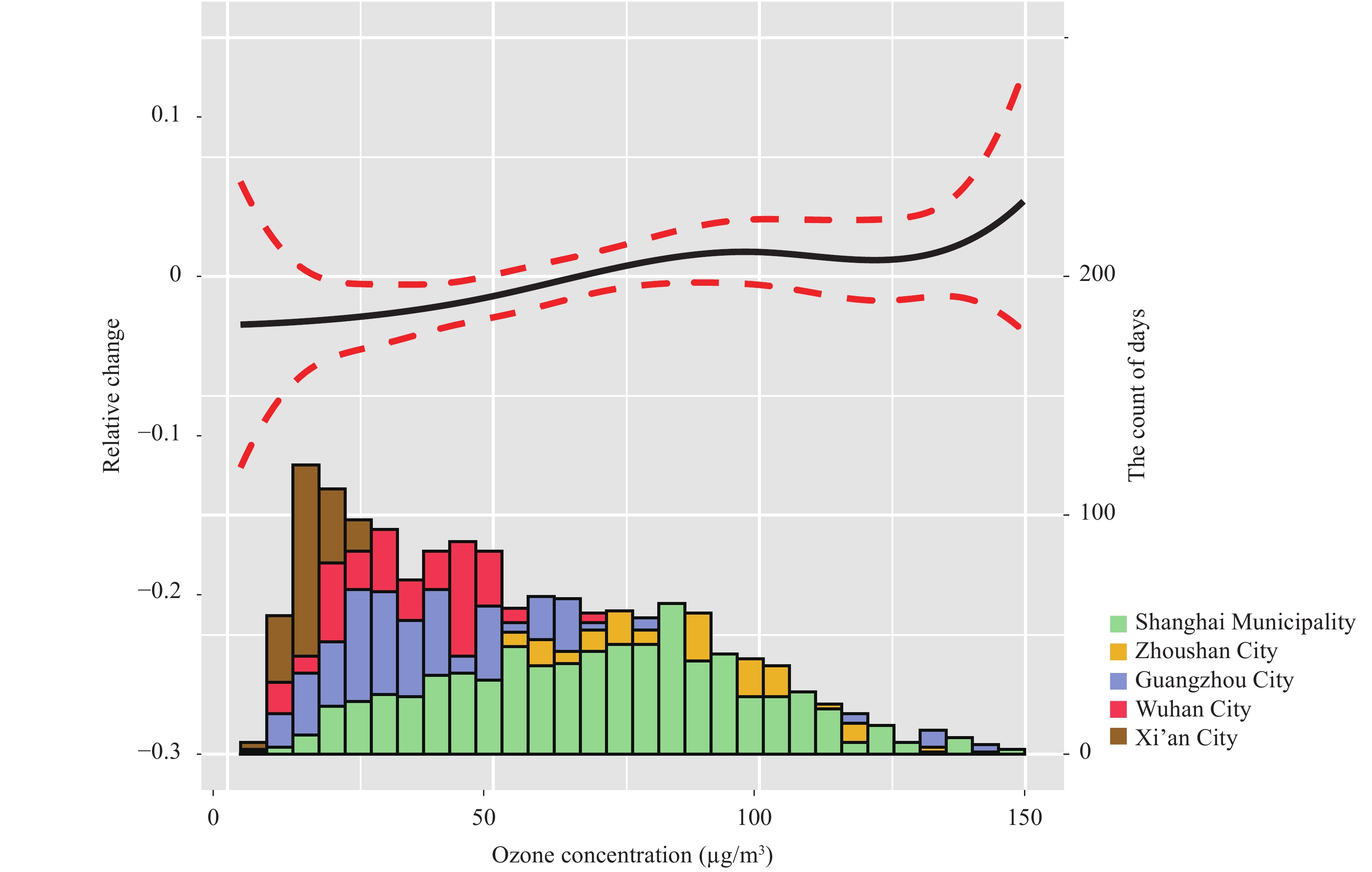 Figure 2.
Figure 2.Exposure-response curve for the association of ozone concentrations (lag 03 days) with outpatient visits for respiratory diseases and distributions of daily mean ozone concentrations by cities. The left Y-axis can be interpreted as the log-relative change from the mean effect of ozone on outpatient visits. The solid line represents the mean estimate, and the dashed lines represent 95% confidence intervals. The height of each bar in the histogram represents the number of days in each bin of ozone concentration.
HTML
-
We conducted a time series study in 5 cities in China to investigate the relationships between ozone exposure and respiratory morbidity. In this study, we found a significantly positive association between ambient ozone concentrations and outpatient visits for respiratory diseases. The pooled effect occurred earlier and were slightly stronger during warm periods. The E-R curve showed the strongest effects of ozone on respiratory outpatient visits at concentrations >120 μg/m3.
Our results suggested a significant association between short-term ozone exposure and increased respiratory morbidity. This finding was consistent with a number of previous epidemiological studies. For instance, a meta-analysis demonstrated that a 10-ppb increase in ozone concentration was associated with a 0.80% (95% CI: 0.19%–1.41%) increase in emergency department visits for respiratory diseases (4). A multi-site study in the US observed a 0.8% (95% CI: 0.6%–1.0%) increase in respiratory emergency department visits in relation to a 10-ppb increase in ozone concentration (5). Such positive associations were also found in Japan (6). For cause-specific respiratory morbidity, the associations between ozone exposure and increased hospital admission for pneumonia and chronic obstructive pulmonary disease have been reported previously (1,7). However, inconsistently, some studies did not find that ozone exposure could cause elevated risks for respiratory morbidity (8), which may result from differences in study population and ozone levels. The results of our study also suggested that there were relatively weaker relationships between ozone exposure and respiratory morbidity in cities with lower levels of ozone air pollution.
Furthermore, we found that the lag pattern of the associations was somewhat different between warm and cool seasons, and the magnitude of associations was slightly greater in warm seasons, suggesting a potential modification effect of ambient temperature on ozone-related respiratory morbidity. This finding was similar with many previous studies that found a significant interaction effect between temperature and ozone on health outcomes (9). Higher ozone concentrations and more outdoor activities on warm days may lead to higher ozone exposure and reduce exposure misclassification. This would consequently add more credibility to the results. The modification effect of temperature may be indicated by the E-R curve that slope is relatively small at low concentrations and becomes the largest when concentrations are >120 μg/m3.
This study was subject to at least three limitations. First, exposure misclassification was inevitable because we used fixed-site monitoring measurements as population exposure, and diagnosis misclassification was possible because cases were extracted according to ICD-10 codes from the database. Second, study areas and hospitals included in the study were selected according to data accessibility, which may lead to selection bias. Therefore, further studies conducted on a larger scale are warranted to confirm our results. Third, we cannot recognize susceptible populations to ozone exposure in this study because demographic data (such as age, sex, and education levels) were unavailable.
In summary, our findings provided relatively creditable evidence for the associations between ozone exposure and increased respiratory morbidity. The results could be used to better assess disease burden of short-term exposure to ozone and further guide policymaking to reduce ozone air pollution and improve public health.
Fundings: This study were funded by the National Natural Science Foundation of China (91843302) and China Medical Board Collaborating Program (16–250).
FootNote
| ① | including Xinhua Hospital (Shanghai Municipality), Putuo Hospital (Zhoushan City ), Zhoushan Hospital (Zhoushan City), the First Affiliated Hospital of Guangzhou Medical University (Guangzhou City), Liwan Central Hospital (Guangzhou City), Hankou Hospital (Wuhan City), Hanyang Hospital (Wuhan City), the First Affiliated Hospital of Xi’an Jiaotong University (Xi’an City), and the Second Affiliated Hospital of Xi'an Jiaotong University (Xi’an City). |
| Citation: |

|